Optics of Lamellar Refractive Keratoplasty
Robert C. Arffa
Refractive keratoplasty refers to a variety of surgical procedures that are performed on the cornea to correct refractive errors. Refractive keratoplasty was introduced in the United States approximately 25 years ago, but it was not until FDA approval of phototherapeutic keratectomy using the excimer laser that patient and physician interest accelerated. Refractive keratoplasty has been and continues to be a rapidly evolving field, and techniques are likely to change in the future. However, the underlying principles will not change, and understanding these principles will provide a basis for understanding future developments. This chapter reviews the refractive properties of the cornea, describes the various lamellar refractive keratoplasty procedures, and explains how these procedures change the refractive properties of the cornea.
REFRACTIVE PROPERTIES OF THE CORNEA
The anterior surface of the cornea is responsible for more than two-thirds of the refractive power of the eye. The refractive power of this surface, which converges light toward a focus at the retina, is due to the large difference in the refractive indices of air (1.000) and the cornea (1.376) and is proportional to the curvature of the anterior surface:
where Ps is the refractive power of the surface in diopters, n1 and n2 are the refractive indices of the first and second media, respectively, and r is the radius of curvature of the surface in meters. From Equation 1, an average anterior corneal surface with a radius of curvature of 7.7 mm has a refractive power of 48.8 diopters (D).
In reality, the anterior surface of the tear film that overlies the cornea is responsible for the refractive power described previously. However, the tear film is thin, and its curvature is determined by the curvature of the cornea. Additionally, the refractive index of the tear film is similar to that of the cornea. Thus, for simplicity, the tear film and cornea may be considered as one for the purposes of refractive calculations, with little loss of accuracy, bearing in mind that surgery that changes the shape of the anterior corneal surface also changes the shape of the anterior surface of the tear film.
Compared with the anterior surface, the posterior surface has a lesser and opposite effect on the refractive power of the cornea, even though the curvature of the posterior surface is steeper than the curvature of the anterior surface. This is because the refractive indices of the cornea (1.376) and aqueous humor (1.336) are close in value. Light is diverged by the posterior corneal surface as it passes from a medium of higher refractive index (cornea) to a medium of lower refractive index (aqueous humor), but the divergence is of a much lesser magnitude than the convergence produced at the anterior corneal surface. From Equation 1, an average posterior corneal surface with a radius of curvature of 6.9 mm has a refractive power of -5.8 D. Therefore, for an average cornea the net corneal refractive power is approximately 43 D.
Theoretically the refractive power of the cornea can be changed by altering the curvatures of the corneal surfaces or the refractive index of the cornea or both. Changes in the anterior corneal curvature affect the refractive power more than changes in the posterior corneal curvature because of the larger change in the refractive indices across the anterior surface. For example, steepening the anterior corneal curvature from 7.5 mm to 6.5 mm would increase the refractive power by approximately 7.7 D, whereas steepening the posterior corneal curvature by 1 mm would decrease the refractive power by less than 1 D.
ANALYSIS OF CORNEAL TOPOGRAPHY
Because most lamellar refractive procedures alter the anterior corneal surface, accurate information about this surface is essential in planning and analyzing these procedures. Early on it was found that changes in keratometry correlated poorly with the change in refraction observed.1,2,3 One hypothesis concerns the fact that the keratometer fits a curve through two points, approximately 3 mm apart, in each of two axes, assuming that the cornea is perfectly spherocylindrical between the points. This reading often does not reflect the postoperative corneal surface power accurately over the visual axis, where irregularity and multifocality may be present.
It is also important to recall that the dioptric power given by the keratometer is an estimate of the total corneal power based on the measured radius of curvature and assuming normal corneal thickness and posterior corneal curvature. Therefore, if the keratometer is used, the anterior surface curvature measurements are more reflective of the refractive change.
Keratoscopy provides more information about the shape and refractive power of the corneal surface than does keratometry (Fig. 1).4 Significantly more detail can be obtained by computer analysis of such images. Most currently used systems for corneal topographic examination utilize Placido disc images. Multiple illuminated concentric rings are placed in front of the cornea, and the reflections of the rings are viewed and analyzed. Corneal curvature can be determined at many points along each ring, giving a detailed image of the corneal surface power (Fig. 2). Unfortunately, this also requires some assumptions about corneal shape and may be less accurate on aspheric surfaces. Elevation maps can also be derived from the curvature data.
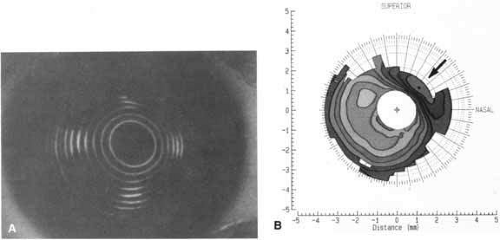 Fig. 1 A. Keratoscope photograph of a cornea 1 year after epikeratophakia for myopia. With a refraction of -1.50 + 1.00 × 50°, the visual acuity is 20/25 +. B. Keratometry reveals 6 D of astigmatism at 45°, which is evident in the keratoscope photograph (arrow). (Courtesy of Stephen D. Klyce, Ph.D., and Steven A. Dingeldein, M.D., LSU Eye Center, New Orleans) |
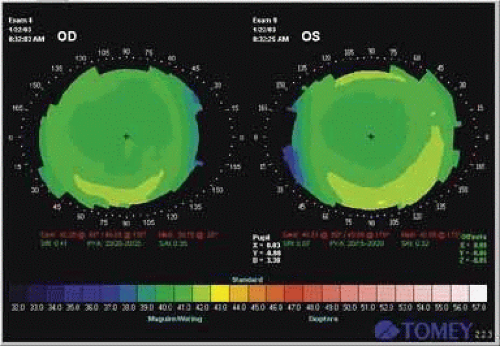 Fig. 2 Computerized analysis of corneal topography after LASIK for myopia. Note central flattening in each eye. |
Many other non-Placido disc systems have been used for corneal topography analysis. The most commonly used today (Orbscan, Bausch & Lomb, Rochester, NY) is based on analysis of multiple Scheimpflug slit images of the cornea. Anterior corneal elevation, corneal thickness, and posterior corneal shape can be determined.
LAMELLAR REFRACTIVE KERATOPLASTY PROCEDURES
Refractive keratoplasty can be divided into lamellar procedures and nonlamellar procedures. Nonlamellar procedures alter corneal curvature without the addition or removal of tissue. Radial keratotomy and various types of incisional surgery for astigmatism are the most common nonlamellar procedures.
Lamellar procedures involve the removal of tissue from the cornea or the addition of tissue or synthetic material to change its refractive power. Most lamellar procedures change the refractive power by altering the anterior corneal curvature, which can be accomplished in several ways. A tissue or hydrogel lens can be placed within the corneal stroma (keratophakia and intrastromal hydrogel lens implantation); a tissue lens can be placed on the anterior corneal surface (epikeratophakia); the anterior lamellae of the cornea can be removed, shaped, and replaced (keratomileusis); or the excimer laser can be used to remove corneal stroma, either on the surface or within the stroma. In one lamellar procedure (intrastromal polysulfone lens implantation), a synthetic lens with a high refractive index was placed within the cornea and changed the refractive properties of the cornea without altering the anterior corneal curvature. Each of these procedures is briefly described in the following sections.
KERATOPHAKIA AND INTRASTROMAL LENS IMPLANTATION
Modern lamellar refractive keratoplasty originated with Jose I. Barraquer’s work in Colombia, South America. In 1949, Barraquer developed keratophakia for the correction of aphakia because of the dissatisfaction with aphakic spectacles and the contact lenses and intraocular lenses that were available at that time. His results were first reported in 1963,5 and the procedure was introduced in the United States in 1977.6 Attempts to adapt Barraquer’s classic form of keratophakia for the correction of myopia have not been successful.
In keratophakia, a plus-powered tissue lens of donor corneal stroma is implanted intrastromally into the patient’s cornea (Fig. 3). The portion of the patient’s cornea that overlies the implanted tissue lens conforms to the anterior surface of the tissue lens, and the anterior corneal curvature steepens.
 Fig. 3 Keratophakia. An anterior section of the patient’s cornea is removed and replaced over a tissue lens of donor corneal stroma. The anterior corneal surface is steepened. |
Prior to surgery, the donor corneal stroma is lathed with a cryolathe, which is a modified contact lens lathe that keeps the tissue frozen as it is being lathed. At the time of surgery, an anterior lamellar section of tissue is removed from the patient’s cornea with a microkeratome, which is similar to a carpenter’s plane. The prelathed tissue lens is placed on the exposed stromal bed, and the anterior lamellar section that was previously removed from the patient’s cornea is sutured back into place on top of the tissue lens. It is necessary to remove an anterior lamellar section of tissue from the patient’s cornea before implanting the tissue lens. If the tissue lens is placed in a lamellar pocket without a 360° anterior incision that penetrates Bowman’s layer, there is little effect on the anterior corneal curvature;7,8 unless Bowman’s layer is severed completely, the posterior layers of the cornea change shape rather than the relatively inelastic anterior layers (Fig. 4).
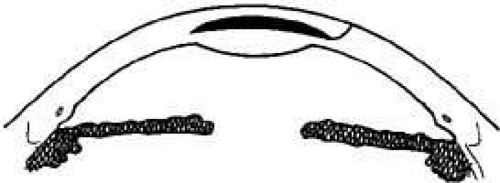 Fig. 4 If an anterior section of the patient’s cornea is not removed and the tissue lens is implanted in a lamellar pocket, the posterior rather than the anterior corneal surface is altered. |
Changes in anterior corneal curvature and refractive power have also been achieved with intrastromal hydrogel lenses, which have a refractive index (1.381) similar to that of the cornea. Both plus-powered9,10,11 and minus-powered12 hydrogel lenses have survived implantation into the corneas of experimental animals by means of the keratophakia technique, but the accuracy of the optical results and the long-term safety were not sufficient to warrant clinical use.
Intrastromal polysulfone lenses have also been used to correct hyperopia and myopia.13,14 Polysulfone has a high refractive index (1.633); a plus or minus lens can be made from this material and implanted in a pocket in the corneal stroma. Unlike tissue lenses and hydrogel lenses, which change the refraction of the cornea by altering the curvature of the anterior corneal surface, polysulfone lenses change the refractive power of the cornea by altering the path of light as it passes through the cornea–lens interface within the cornea. No change in the anterior corneal curvature is necessary to achieve this effect. Therefore, these lenses can be implanted into a lamellar pocket without the need for removing an anterior lamellar section of tissue.
KERATOMILEUSIS
In 1964, Barraquer developed keratomileusis for the correction of myopia.15 He later adapted the technique for the correction of hyperopia and first reported his results in 1981.16
In keratomileusis, an anterior lamellar section of tissue is removed from the patient’s cornea with a microkeratome (Fig. 5). This tissue is lathed, from the posterior surface, on a cryolathe and is then sutured back onto the stromal bed (Fig. 5). If more tissue is removed from the periphery of the tissue than from the center, the anterior corneal curvature steepens; if more tissue is removed from the center than from the periphery, the anterior corneal curvature flattens. This autoplastic keratomileusis procedure requires no donor tissue. However, a prelathed donor tissue lens can be used, in which case the procedure is called homoplastic keratomileusis.
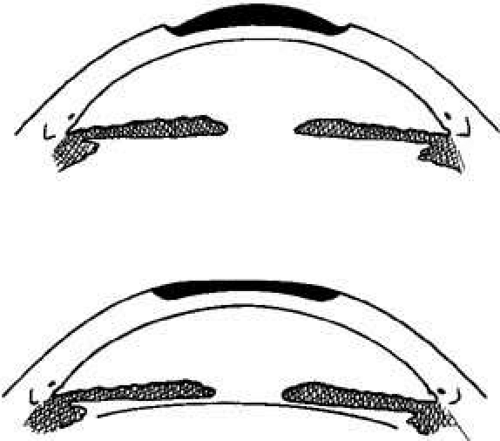 Fig. 5 Keratomileusis for aphakia (top) and myopia (bottom). An anterior section of the patient’s cornea is removed, shaped from the posterior surface, and replaced, altering the anterior corneal surface. |



