Optics of Gonioscopy
Jacob T. Wilensky
Examination of the anterior chamber angle, gonioscopy (from the Greek gonio meaning “angle”), is an essential pan of an ophthalmic examination. It is particularly valuable in differentiating between open-angle and angle-closure forms of glaucoma and is essential to detect traumatic angle recession or angle neovascularization. It may reveal the presence of foreign bodies, abnormal pigmentation, or even tumors within the angle. It is also important for therapy. Goniotomy, which has long been a standard treatment for congenital glaucoma, requires direct visualization of the chamber angle. A number of relatively new laser techniques for the treatment of glaucoma (most notably trabeculoplasty) are now in wide use, and each requires visualization of the chamber angle. Thus it is obvious that a solid understanding of and facility with gonioscopy is mandatory for the ophthalmologist.
When light passes at an angle from one medium to another, it bends according to the laws of refraction. Light bends toward the normal (a line perpendicular to the interface between the two media) if it enters a medium of higher index of refraction, or away from the normal if it enters a medium of lower index of refraction.
Consider a beam of light passing from one medium into another of lower index of refraction. As the angle of incidence progressively increases, the emerging light will be closer and closer to parallel to the interface between the media. At a certain angle of incidence, the light will be bent in the second medium such that it is parallel to the interface; that is, it will not enter the second medium. This angle of incidence is known as the critical angle. When the angle of incidence is greater than the critical angle, the light will not emerge but instead will be reflected back into the first medium (Fig. 1).
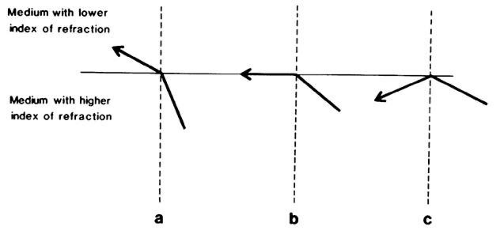 Fig. 1. (a) As the light ray enters a medium of lesser density, it is bent away from the normal. (b) When the critical angle is reached, the light ray is bent so that it is parallel to the interface between the two media. (c) When the critical angle is exceeded, the light ray is reflected internally. |
Light rays originating from the depths of the anterior chamber angle of a normal eye strike the corneal surface at an angle of incidence greater than the critical angle. Thus, these light rays are reflected completely internally (Fig. 2). Since light rays from the angle cannot leave the eye, the angle structures ordinarily are not viewable. In order to see the angle structures, the air-cornea interface must be modified or eliminated. This may be accomplished by using various types of gonioscopy lenses.
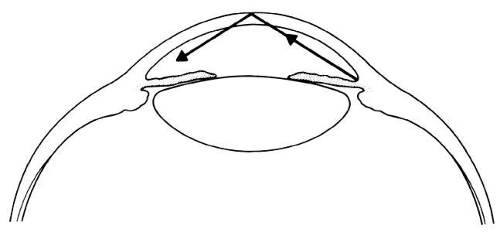 Fig. 2. Light rays originating in the recess of the chamber angle exceed the critical angle of the cornea-air interface and are reflected internally in the normal eye. |
The first person to practice gonioscopy is reported to have been Trantas, a Greek ophthalmologist,1 at about the beginning of the 20th century. In an eye with keratoglobus, he was able to see the angle using a direct ophthalmoscope. He also practiced indentation of the limbus to alter the anatomy of this region and was able to examine the angles of the eyes of a number of glaucoma patients by this technique. Saltzman, an Austrian ophthalmologist, appears to have developed a somewhat similar technique around the same time. Recognizing that it was in highly myopic eyes or in other eyes with a steeper cornea that he was able to visualize the chamber angle, he placed a corneal contact lens on normal eyes in an attempt to visualize their angles. The initial contact lens that he used caused considerable distortion, and he subsequently had a somewhat steeper lens made specially for him by Zeiss. This lens was further refined by Koeppe, who had a steeper, thicker lens manufactured to improve the visual quality of the image seen.
TYPES OF GONIOSCOPY LENSES
The use of goniolenses of this type (Koeppe) constitutes the direct method of gonioscopy. Since these goniolenses have a steeper curvature than the cornea, there is a space between the inner surface of the lens and the cornea, This space is filled with methylcellulose, saline, or some other solution. For all practical purposes this solution creates an optical continuity between the lens and the cornea (Fig. 3). The more steeply curved outer surface of the gonioscopy lens replaces the cornea-air interface, thus altering the critical angle and permitting visualization of the angle. The chamber angle is observed by viewing directly across the anterior chamber. A true image is seen with true spacial orientation. Magnifying loops, a hand-held microscope, or an operating microscope is used to magnify the image viewed (Fig. 4); the gonioscopy lens itself provides about 1.5 x magnification.
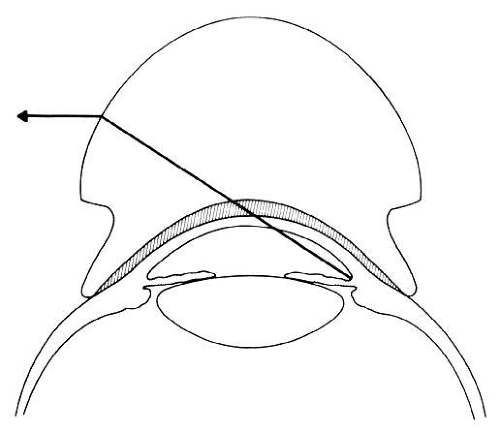 Fig. 3. Schematic drawing of a direct gonioscopy lens. The steeper radius of curvature of the gonioscopy lens is substituted for that of the cornea, permitting direct visualization of the angle recess. Note the fluid bridge between the cornea and the gonioscopy lens, which links them functionally into a single optical system. |
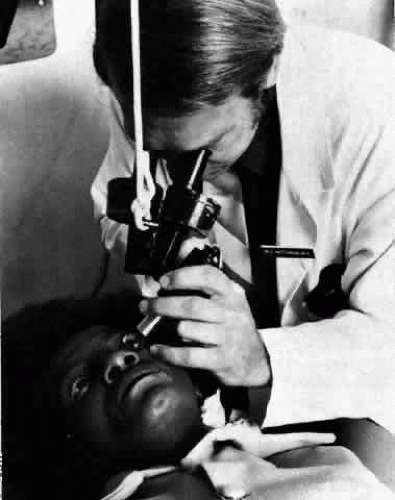 Fig. 4. Performance of direct gonioscopy. The hand-held microscope is partially supported by a counterweight, and illumination is supplied by a separate illuminator. |



