Optical Rehabilitation of Aphakia with Epikeratophakia
Keith S. Morgan
Epikeratophakia is a form of refractive surgery wherein the anterior curvature of the cornea is altered by the addition of a tissue lens created from donor cornea. The tissue, procured through eye banks, is frozen and shaped on a cryolathe in a modification of one of the keratorefractive surgical procedures originated by Barraquer.1 In Barraquer’s keratomileusis procedure, a disc of anterior cornea is shaved off with the microkeratome, frozen on a cryolathe, carved to the required specifications intraoperatively, based on theoretic and empiric formulas, and replaced in the stromal bed. Epikeratophakia differs in that donor tissue rather than the patient’s own tissue is used, the tissue is precarved, and the resulting tissue lens is placed on the anterior surface of the recipient cornea (Figs. 1 AND 2). No microkeratome cuts are made in the patient’s cornea; the only modifications are the removal of the epithelium and the trephination of a partial-depth, circular incision into the stroma in the peripheral cornea. Therefore, Bowman’s layer remains intact across the central cornea, which makes the procedure extraocular, potentially reversible, and more easily adaptable to corneas of different sizes and shapes.
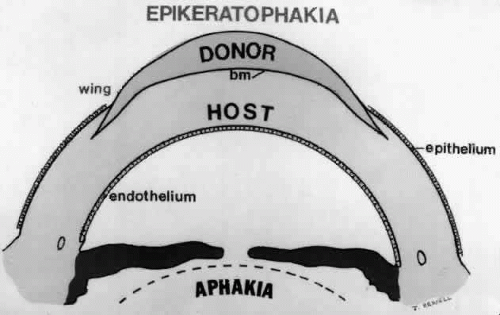 Fig. 1. Overview of relationship of donor lenticule to host cornea. |
 Fig. 2. Slit lamp picture of healed epikeratophakia lenticule, demonstrating double-thickness cornea. (Morgan KS, Ashell PA, Kaufman HE: Cataracts in children: Epikeratophakia for the correction of aphakia. Reproduced with permission from the Journal of the Louisiana State Medical Society, 135 [2]:23–25, 1986) |
Epikeratophakia tissue lenses are generally supplied from a commercial source, which processes the tissue to order and lyophilizes it for shipping and storage until surgery. During surgery the lyophilized tissue lens is hydrated and then sutured to the patient’s cornea. Alternative tissue preparation techniques include carving unfrozen tissue with the use of microkeratome instrumentation (BKS 1000, Allergan Medical Optics, Irvine, CA), as described by Krumeich and Swinger,2,3 or possibly by means of the excimer laser.4
INDICATIONS
Epikeratophakia has been used to correct aphakia in adults5 and children,6,7 as well as myopia,8 and to treat keratoconus.9 However, only epikeratophakia for pediatric aphakia is discussed here.
The first pediatric patients to undergo epikeratophakia were children with unilateral congenital or traumatic cataracts who were either intolerant to contact lens wear or who were considered to be poor candidates for successful contact lens wear.10,11,12,13,14 Although the procedure was originally envisioned as a permanent optical correction for young children with unilateral congenital cataracts, it soon became apparent that epikeratophakia was not well suited as a first or sole solution to this problem because it could not achieve the very high power correction required for neonates and infants.15 Also, the rapid changes in refraction in the first year of life required a more flexible and easily changed optical prosthesis. For these reasons, epikeratophakia has been recommended for contact lens-intolerant, aphakic children who are 1 year of age or older. In these cases, the changes in dioptric power requirements that occur with the passage of time can be corrected with changes in spectacle overcorrection.15
Children who have traumatic cataracts with corneal lacerations are well served by this procedure because the injury often destroys the capsular support that can be used to stabilize an intraocular lens.16,17,18 The epikeratophakia graft provides structural support for the weakened cornea and minimizes the induced irregular and regular astigmatism, in addition to correcting the optical error (Figs. 3 AND 4).
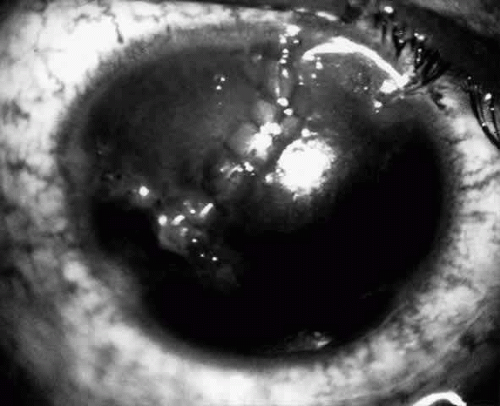 Fig. 3. Lacerated cornea with a hyphema. (Morgan KS, Ellis GS, Marvelli TL, Arffa RC: Epikeratophakia in children with traumatic cataracts. J Pediatr Ophthalmol Strabismus 23: 108–113, 1986) |
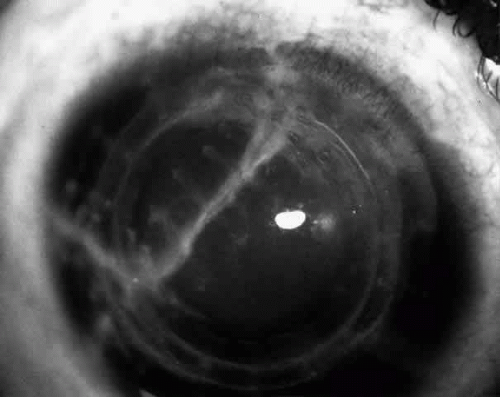 Fig. 4. Same patient as in Figure 11, with epikeratophakia lenticule in place 3 months after surgery. (Morgan KS, Ellis GS, Marvelli TL, Arffa RC: Epikeratophakia in children. with traumatic cataracts. J Pediatr Ophthalmol Strabismus 23:108–113, 1986) |
Although epikeratophakia is primarily a secondary procedure for children who cannot tolerate a contact lens, it may be combined with cataract extraction in children with acquired cataracts in whom contact lens compliance is unlikely. The results in these cases have been mixed.19,20 The accuracy of the achieved correction may be decreased with the combined procedure, compared with epikeratophakia alone, possibly because of the variation in intraocular pressure that occurs with a combined procedure, but there is no increase in nonoptical complications. The best example of a candidate for this usage would be a 2-year-old child with a subluxed lens who will not tolerate a trial of a contact lens prior to surgery.
Epikeratophakia is also useful in older children who are contact lens-noncompliant.7 The results actually seem to be somewhat better in these older children, perhaps because they are better able to cooperate with not rubbing their eyes but are still able to benefit from the more rapid healing common to young patients. Also, amblyopia is generally not a factor, so the problems of patching do not arise. In uniocular aphakia in older children, many would argue the advantage of an intraocular lens. However, epikeratophakia is likely safer, with less potential for severe complications, is reversible, and has good but not excellent power predictability. Optical rehabilitation is slightly slower than with intraocular lens implantation. The advantages that may be expected with an intraocular lens (faster rate of recovery and better power predictability) must be balanced against the possibility of long-term risks in a young person, and the difficulties associated with the removal or exchange of an intraocular lens.
Epikeratophakia has been used in selected cases of bilateral aphakia in children.20 Such use must be approached with caution, however, because amblyopia could be induced if one eye develops complications that reduce vision. This is a special concern in that most bilaterally aphakic children do tolerate spectacle correction, so the parents must be fully informed and the risk-benefit ratio of surgical correction must be weighed carefully.
In a contact lens-intolerant child who has an intraocular lens in one eye, an epikeratophakia graft may be an appropriate option for the other eye. In these cases, epikeratophakia may avoid the long-term problems that could be associated with bilateral intraocular lens implantation, while leaving the options open for future surgery in the adult years, if necessary or desired.
CONTRAINDICATIONS
As a procedure that involves the surface modification of the cornea, epikeratophakia would be contraindicated in patients with severe ocular surface problems, including uncontrolled blepharitis and keratitis sicca. Also any child who exhibits poor wound healing or has a compromised metabolic status would not be a good candidate for this procedure. The most crucial part of healing is the reestablishment of the epithelial cover. If the child has extremely poor vision and is prone to ocular digital stimulation, this habit may prevent proper healing.
Children who have had radiation treatment for ocular or orbital disease or who have radiation-induced cataracts will often develop surface ocular problems from radiation keratitis.21 These children seem to do poorly with contact lenses and epikeratophakia over the long haul and they should be considered for intraocular lens implantation.
One is often confronted with a child who has had a severe corneal laceration and requires penetrating keratoplasty. Correcting these children’s eyes with an epikeratophakia tissue lens seems to be almost impossible. A variety of techniques such as placing the epikeratophakia graft inside the corneal transplant or combining it with the corneal transplant have been tried but the results have been poor. Although the tissue lens can be coaxed into healing, it often does so at the cost of the viability of the corneal transplant. For these reasons I am conservative in recommending corneal transplantation for young children who are in the age group at risk for amblyopia because of the difficulties in correcting aphakia in conjunction with penetrating keratoplasty. In such patients, an epikeratophakia lens over the corneal scar may provide adequate visual rehabilitation, or if a corneal transplantation is unavoidable, an intraocular lens implant may be the best option for optical correction of aphakia.
Extremely small eyes with corneal diameters less than 9 mm present a special problem for epikeratophakia.20 In these cases, there appears to be a higher incidence of complications because the keratectomy into which the edge of the graft is sutured extends out to the limbus, leading to problems with vascularization.
PROCEDURE
POWER CALCULATION
After a complete ophthalmologic examination, the child may be sedated with chloral hydrate, if necessary, and keratometry and retinoscopy are performed. A-scan axial lengths must be obtained when retinoscopy is not possible. The measurements provide the parameters for ordering the tissue lens, which is prepared at a commercial facility and shipped to the hospital.
There have been technical difficulties in calculating powers for young children. The most commonly utilized formulas were designed for adult eyes and when they were used for short eyes with steep corneas, as seen in infants, the results were erroneous.22 Newer formulas seem to alleviate this problem.23,24 However, no formula is ever as accurate as retinoscopy in children’s eyes. Thus, retinoscopy should be used whenever possible-either with trial lenses alone or with trial lenses over an aphakic trial lens.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


