SURGICAL TECHNIQUE
General endotracheal anesthesia is induced with the patient in the supine position. The endotracheal tube is secured to the left side out of the surgical field. The head is secured in a doughnut, and eyes are carefully taped shut with Steri-Strips or thin pieces of tape after placement of lubricating ointment. The eyes should be palpated at the beginning of the case to assess firmness at baseline. They should remain accessible and clearly visible throughout the surgery should any orbital complication be suspected during the surgery. The nose is maximally decongested using cotton pledgets soaked in oxymetazoline. Image guidance is registered and verified at this juncture. The face is prepped and draped in the standard sterile fashion.
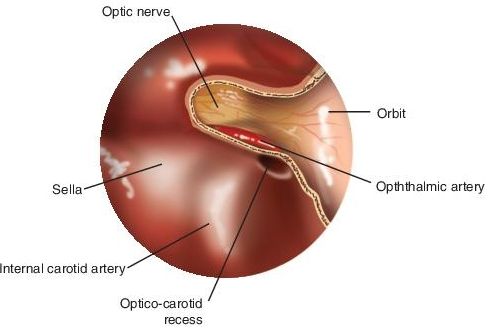
The procedure is started with a 0-degree endoscope. One percent lidocaine with 1:100,000 epinephrine is injected along the lateral nasal wall and the sphenopalatine foramen. In general, a transethmoid approach to the sphenoid sinus will provide the best exposure of the orbital apex and optic nerve region. A standard uncinectomy with maxillary antrostomy is performed to improve access to the middle meatus and to provide a place for blood to collect out of the surgical field. The floor of the orbit also provides a general landmark to the level of the sphenoid ostium in the SER. Total ethmoidectomy is now performed to skeletonize the orbit from the lacrimal system to the orbital apex. Great care is taken to avoid violating the lamina papyracea or periorbita as resulting herniation of orbital adipose tissue will obscure the surgeon’s vision. The superior turbinate is identified in the SER; the lower third is sharply resected to identify the sphenoid ostium. The sphenoid sinus is now opened widely to expose the optic nerve and ICA bulges. If the optic nerve courses through an Onodi cell, this should be fully dissected and the relationship between this cell and the sphenoid sinus established.
The bone at the orbital apex is now removed approximately 1 cm from the optic nerve tubercle. The bone at the orbital apex can be thick; a diamond burr drill may be required to expose the periorbita and annulus of Zinn. The bone over the medial optic canal is next addressed with a long 2- or 3-mm diamond burr drill. Concurrent suction irrigation is critical to clear bone dust and blood from the surgical field and to minimize transmission of heat to the optic nerve sheath (Fig. 1.1). The drill should be circumferentially visible when being used; this will decrease the risk of inadvertent injury to the ICA canal or the planum sphenoidale. The bone is initially blue lined with the drill and then can be subsequently removed with curettes or otologic picks. The entire optic nerve sheath, typically ranging from 10 to 15 mm, is exposed from the lateral wall of the sphenoid to the optic chiasm. The optic nerve sheath is decompressed 180 degrees along the medial and inferior aspects (Fig. 1.2).
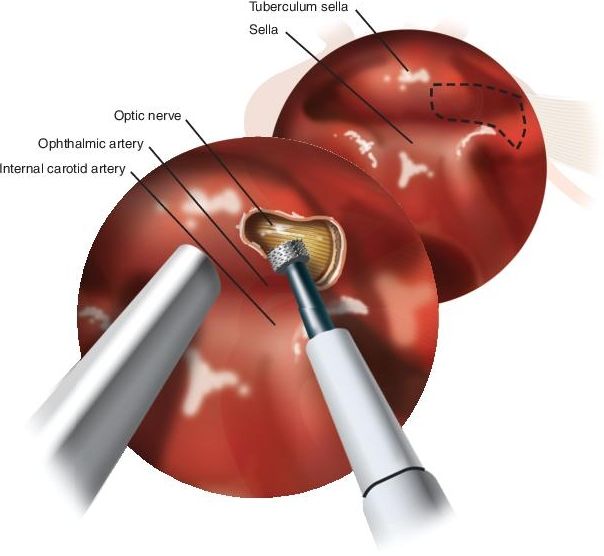
FIGURE 1.1 Endoscopic view demonstrates drilling of the medial optic canal with a diamond burr. Concurrent irrigation is critical to minimize heat transmission, and suction is imperative to clear blood and bone dust from the operative field.