Optic Nerve
Alex V. Levin
Thomas W. Wilson
J. Raymond Buncic
Agnes Wong
Wai-Ching Lam
The optic nerve arises as an outpouching of the anterior neural tube. The optic stalk, formed at the fourth week of gestation, is continuous with the forebrain at one end and the optic vesicle at the other. The optic vesicle, derived from neuroectoderm, forms the neurosensory retina and retinal pigmented epithelium. As early as the sixth week of gestation, ganglion cells in the optic vesicle become the first retinal cells to differentiate and their axons begin to reach the formative occipital cortex by the eighth week. Neural crest cells form the optic nerve sheath. Abnormalities of this process cause congenital anomalies of the optic nerve and optic disc.
Optic nerve function is often affected by underlying systemic illness or by local processes, including compression, inflammation, or the effects of other intracranial disease. The optic nerve may respond to the many pathologic processes by becoming edematous, hyperemic, or, with time, atrophic. Loss of optic nerve fiber is more readily appreciated in children because of visible changes in the normally thick nerve fiber layer in children. Congenital anomalies of the optic nerve may also be associated with underdevelopment of the macula.
Although sophisticated evaluation such as optical coherence tomography, Doppler ultrasound, and neuroimaging are helpful, any physician can assess the optic nerve using the ophthalmoscope.
 Figure 9.1 Normal Nerve Fiber Layer This photograph demonstrates a normal optic nerve and macula. The nerve fiber layer is thickest in the perifoveal area. The thickness is demonstrated by the relationship of the retinal blood vessels usually buried within the retina and overlying light reflexes. The central reflexes form a doughnut-shaped mound, with a perifoveal inner circular reflex and an outer reflex where the curvature of the macula evens out. Within the fovea, the nerve fiber layer is absent, thus highlighting the healthy surrounding circular macular mound (mound of Buncic) of the thick nerve fiber layer. Flattening of this mound indicates loss of thickness of the retinal nerve fiber layer and decrease in the number of axons into the optic nerve (Figs. 9.15 and 9.21). |
 Figure 9.2 Optic Nerve Aplasia Optic nerve aplasia is characterized by a complete absence of the optic nerve and retinal blood vessels. Eyes with aplastic optic nerves do not have any visual potential. This computed tomography scan illustrates the complete absence of the optic nerve structures bilaterally. As the globe is present and represents the end of the optic stalk, optic nerve aplasia is due to either failure of retinal ganglion cell development or abnormal invagination of the ventral fissure. Histopathologically, a vestigial nerve and optic nerve sheath may be found. This very rare disorder has only been observed sporadically. |
 Figure 9.3 Optic Nerve Hypoplasia Optic nerve hypoplasia is characterized by a small optic disc (thick arrow). It is often surrounded by a yellowish mottled peripapillary halo, bordered by a ring of increased or decreased pigmentation (the “double-ring” sign, thin arrow). The outer ring represents the normal junction between the sclera and lamina cribrosa, whereas the inner ring represents the termination of an abnormal extension of retina and pigmented epithelium over the lamina cribrosa. The hypoplasia may be unilateral or bilateral. The retinal vessels are often anomalous, as shown here. Visual acuity does not always correlate with the size of the optic disc, whereas the thickness of the macular mound may be helpful. Optic nerve hypoplasia is frequently associated with the de Morsier syndrome (septo-optic dysplasia), which refers to the constellation of hypoplastic anterior visual pathways, absence of the septum pellucidum, and thinning or agenesis of the corpus callosum. Ectopia of the posterior pituitary gland on magnetic resonance imaging may indicate pituitary deficiency. Other brain abnormalities may coexist. |
 Figure 9.4 Optic Nerve Coloboma Optic disc coloboma represents incomplete fusion of the embryonic fissure. The superior portion of the nerve appears normal, whereas the inferior portion is often yellowish white, excavated, and surrounded inferiorly by colobomatous choroid and retina. Systemic associations include CHARGE (coloboma, heart defects, atresia choanae, retarded growth and development, genitourinary abnormalities, and ear defects). Optic nerve coloboma can be part of a wide spectrum of coloboma ranging from involvement of the iris anteriorly to the macula posteriorly, with or without microphthalmia. The optic disc may appear enlarged, and if located within a larger chorioretinal coloboma, it may look quite dysplastic or even be unrecognizable. |
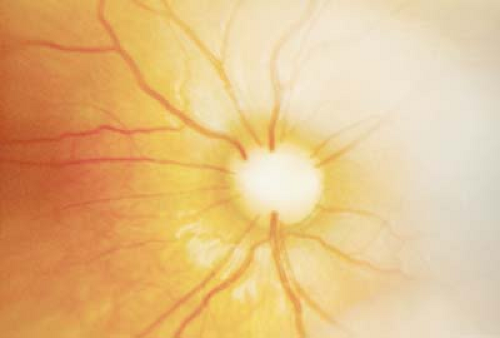 Figure 9.5 Morning Glory Disc The morning glory disc anomaly is a congenital, funnel-shaped excavation of the posterior fundus that incorporates the optic disc. It is characterized by a central white glial tuft, retinal vessels that exit radially from the borders of the optic nerves, and peripapillary pigmentation. The optic nerve is larger than normal and also has a funnel shape when visualized by neuroimaging or ultrasound. Morning glory disc is usually unilateral, more common in females, and less common in patients of African descent. Visual acuity can vary from normal to hand motion. Morning glory disc can be associated with basal encephalocele, and a midline notch in the upper lip is a signature sign. Vision loss can also occur from serous retinal detachment. Rarely, a morning glory disc can be contractile. |
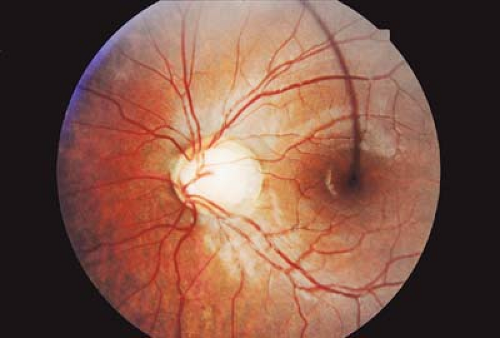 Figure 9.6 Optic Pit An optic pit (arrow) is an oval depression within the optic nerve. It is usually grayish in color and typically located centrally or temporally. An optic pit is usually unilateral and the affected disc is often slightly larger. Complications include serous detachment of the retina if associated with a temporally located pit. A macular hole can occur as a result of the serous retinal detachment. Without retinal detachment, optic pits rarely affect vision. |
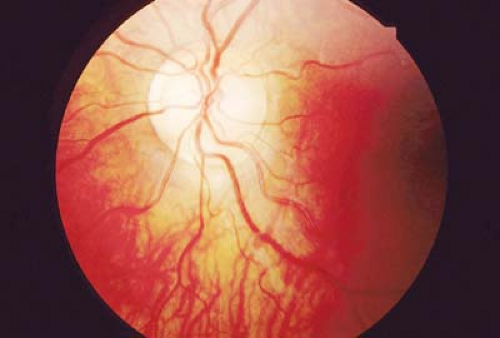 Figure 9.7 Megalopapilla Megalopapilla is a larger than normal optic disc. The cup-to-disc ratio is often increased, although there is no increased risk for pediatric glaucoma. Visual acuity and visual field are usually normal except for an enlarged blind spot. The cause of this disorder is unknown, although familial megalopapilla has been rarely described. It is not associated with coloboma (Fig. 9.4). |
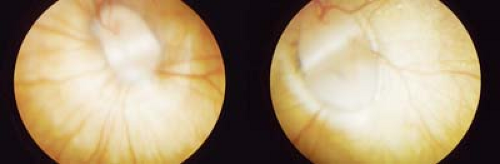 Figure 9.8 Bifid Disc Bifid disc, or doubling of the optic disc, is due to abnormal division of the optic nerve during ocular development. Both optic nerves typically have their own blood supply. As shown here, there is usually a white band between the two discs as well as some contiguous tissue. Visual acuity is subnormal. Only sporadic cases have been described. |
 Figure 9.9 Congenital Tilted Disc The tilted disc syndrome is a nonhereditary, usually bilateral disorder of the optic nerve. The optic disc is elevated superotemporally and depressed inferonasally, with an inferior scleral crescent. The disc is oval in shape and its long axis tends to be oriented obliquely. There is usually associated situs inversus (Fig. 9.10) of the retinal vessels. A pseudobitemporal hemianopia may be observed. This is considered to be a refractive scotoma related to regional myopia localized to the inferonasal retina. The hemianopia does not respect the vertical meridian and is reduced or eliminated with the use of minus lenses. |
 Figure 9.10 Situs Inversus Situs inversus is a variation of the course of the temporal retinal blood vessels. Normally, the temporal retinal blood vessels are directed temporally. In situs inversus, however, the temporal blood vessels course nasally first before turning temporally. Situs inversus is associated with tilted disc syndrome (Fig. 9.9) but can occur in entirely normal eyes. Retinal traction can cause a secondary acquired situs inversus. Primary congenital situs inversus has no visual significance. |
 Figure 9.11 Prepapillary Vascular Loops Prepapillary vascular loops are extensions of the normal retinal blood vessels into the vitreous. They often have a spiral configuration but do not extend to the posterior capsule and are therefore differentiated from persistent hyperplastic primary vitreous (Chapter 7: Lens, Figs. 7.14 and 7.15). These loops are remnants of the primitive hyaloid vascular system. The majority of the loops are arterial and can be associated with retinal artery occlusion. Otherwise the loops are entirely benign.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|