Chapter 12 This chapter can be used to diagnose the patient with optic nerve pallor. The tables should be used for the broad classification of optic nerve pallor. It is assumed that you have just examined the patient, but have not performed a full neuro-ophthalmic examination. The following paragraph should assist in assigning the patient to the proper category. When examining a patient with the finding of optic nerve pallor, it is helpful to know whether or not the patient has any complaints regarding the vision in the affected eye (s). This can be specifically sought with leading questions regarding dimness, darkness, loss of color perception, or visual field defects. Further helpful information to elicit includes a known history of optic nerve disease, such as an event of ischemic optic neuropathy or optic neuritis, or perhaps a history of significant ocular or head trauma. History of associated illnesses such as brain tumor, multiple sclerosis, or metabolic disease should be elicited. Family history of neurologic and ophthalmic disorders may be of assistance in diagnosing such disorders as glaucoma, drusen, or Leber’s hereditary optic neuropathy. Examination of elements specific to optic nerve function including visual acuity, color vision, relative afferent pupillary defect, and visual field testing should be performed. Testing the remaining cranial nerves (including olfaction) may help in localization of an optic nerve disorder. Careful dilated fundus examination should include viewing of the peripheral retina because some forms of retinal disease can result in optic nerve pallor. The characteristics of the pallor should be noted. Altitudinal versus diffuse pallor and temporal versus bow-tie pallor may help in localizing the defect. Careful attention to the degree of cupping is warranted because glaucoma causes greater cupping than pallor, whereas other optic neuropathies may favor pallor. Ancillary testing with visual evoked responses (VERs) may be helpful to document amplitude and velocity of waveforms, but is usually not necessary if optic nerve function is carefully examined clinically. Contrast sensitivity testing is felt to be one of the most sensitive for detecting optic nerve dysfunction. Comparison to prior testing can be very helpful in ascertaining stability or progression of optic nerve function. If this information is not available, then one must either rely on the patient as a witness or assume that the optic neuropathy may be progressive. With the above information, it should be possible to determine the broad category of disease that best fits your patient using the table below. Within the text corresponding to the broad category are descriptions of findings from the history and physical examination to more precisely ascertain the diagnosis. The classic presentation for the disease will be described, as well as “red flags” that should alert you to the possibility that other diagnoses should be considered. You will then be referred to the chapter corresponding to that diagnosis wherein guidance for further testing and management can be found. Table 12–1 is used for patients with either normal or abnormal optic nerve function with optic nerve pallor. In this setting, it is important to distinguish between progressive visual loss due to progressive optic nerve dysfunction and visual loss due to either the normal process of aging or the advancement of other disorders, such as refractive error, macular degeneration, or cataract. Table 12–2 is used to determine the specific category of optic neuropathy. 1. Is optic nerve function truly normal? 2. Does the patient have visual complaints referable to the optic nerve? 3. These conditions are typically binocular, but may be asymmetric. These are congenital abnormalities that are associated with all levels of optic nerve function. Careful fundus examination should assist in making this diagnosis. In most cases, the nerve appears pale because sclera or lamina cribrosa are visible where the neuroretinal rim is expected. Tilted discs and scleral crescents are typically found in myopic patients (Fig. 12–1). • These may be associated with malformations of the iris, lens, and choroid. • May be unilateral or bilateral • Most often have abnormal visual fields, but may have only an enlarged blind spot • May be unilateral or bilateral • Majority have visual field defects (62%) • May be associated with serous retinal detachments • Typically seen in the moderate to high myope
OPTIC DISC PALLOR
BROAD CATEGORY 1: PSEUDO-PALLOR
QUESTIONS TO ASK AND POINTS TO KEEP IN MIND
ANOMALOUS OPTIC NERVES (SEE CHAPTER 23)
COLOBOMA
Classic Presentation
Red Flag
 Coloboma may be associated with other cranial malformations such as basal encephalocele.
Coloboma may be associated with other cranial malformations such as basal encephalocele.
PITS
Classic Presentation
TILTED DISC
Classic Presentation
Altitudinal pallor without cupping | Ischemic optic neuropathy |
Temporal pallor | Optic neuritis |
Bow-tie atrophy/pallor | Chiasmal or optic tract disease |
Chalk white | Leber’s hereditary optic neuropathy |
Gliosis | Prior edema, either papilledema or anterior ischemic optic neuropathy (AION) |
Cupping greater than pallor | Glaucoma |
Pale and elevated | Drusen, chronic papilledema, chronic inflammation, mass lesion |
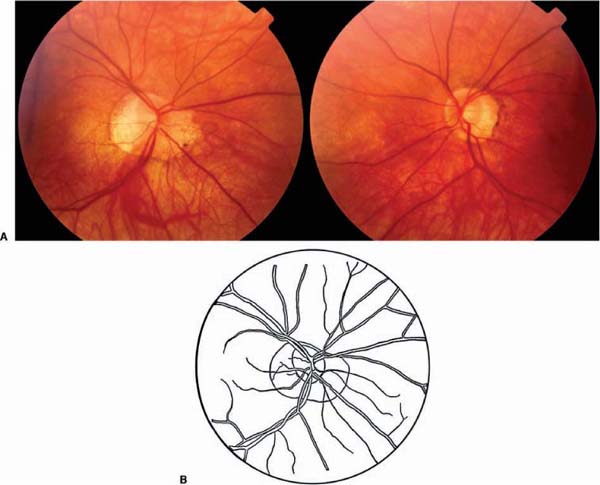
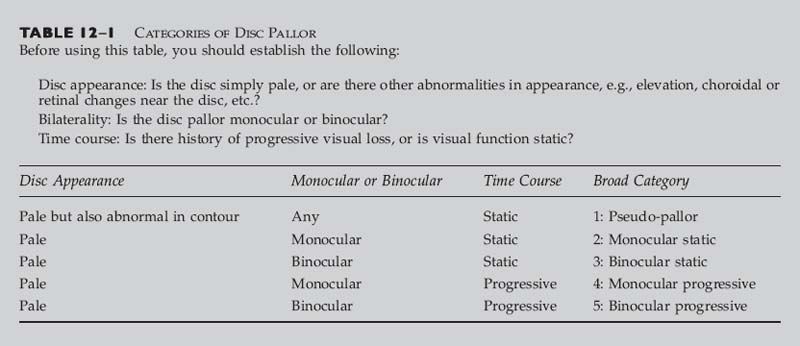
FIGURE 12–1 A 43-year-old woman referred for headaches and right optic neuropathy. She has myopia OU, more OD than OS. Vision 20/50 OD and 20/20 OS with normal color vision and no relative afferent pupillary defect. Note that the sclera is visible almost 360 degrees around the nerve OD. OS shows a more typical scleral crescent. The optic nerves themselves are normal and symmetric (A). The line drawing (B) more clearly delineates the optic nerve substance from the surrounding sclera OD.
• Optic nerve entering the globe at an oblique angle (nasal, temporal superior, or inferior projection) causes oval disc with depression on one side and elevation on the other. The nerve fiber layer on the depressed side is typically more splayed over the sclera, causing pale appearance.
• May have a visual field defect, but can be normal
• Visual field defect may resemble bitemporal hemianopia, and may improve with plus lenses.
• Mildest form is the scleral crescent
LARGE PHYSIOLOGIC CUP
Classic Presentation
• Normal optic nerve function
• May be more prevalent in African Americans
• Rim of healthy nerve tissue
• Vessels may penetrate nerve substance indicating congenital nature rather than atrophy
CONGENITALLY BLOND (LIGHT) FUNDUS
Classic Presentation
• Pseudo-pale retina is in proportion to pseudo-pale nerve
• Normal optic nerve function
• Typically found in blonds
Red Flag
 If iris transillumination defects are present, consider ocular albinism.
If iris transillumination defects are present, consider ocular albinism.
GLAUCOMA
Classic Presentation
• Enlarged cup-to-disc ratio (“cupping”) without pallor of the remaining neuroretinal rim
• Peripheral vision loss precedes central loss.
• Patients typically have no visual complaints unless at end stage.
• Family history may be present.
• Usually bilateral but may be asymmetric
• Central vision usually normal, intraocular pressure usually elevated
• Increased intraocular pressure is often, but not always, present.
Red Flag
 The presence of cupping does not exclude the possibility of a compressive lesion.
The presence of cupping does not exclude the possibility of a compressive lesion.
PSEUDOPHAKIA
Classic Presentation
• Results from removal of the naturally yellow native lens and implantation of a clear intraocular lens during cataract surgery, making the retina and optic nerve appear less yellow
• When compared with phakic (native lens) eye, the pseudophakic eye may appear pale, but the neuroretinal rim will be of similar thickness (Fig. 12–2).
Red Flag
 The cataract may have been removed in an attempt to improve visual function in an eye with an optic neuropathy. Make sure the optic nerve function is normal as well.
The cataract may have been removed in an attempt to improve visual function in an eye with an optic neuropathy. Make sure the optic nerve function is normal as well.
MYELINATED NERVE FIBER LAYER
Classic Presentation
• May be present from birth, or may appear during childhood
• May cause visual field defects
• May be unilateral or bilateral
• Myelination of the nerve fiber layer beyond the lamina cribrosa can cause a dense, streaky patch of white tissue at the nerve margin.
• Myelination typically obscures the retinal vessels.
Red Flag
 May be difficult to distinguish from nerve fiber layer infarct or “cotton wool spot”
May be difficult to distinguish from nerve fiber layer infarct or “cotton wool spot”
BROAD CATEGORY 2: MONOCULAR STATIC
Many of the entities described in this section may become bilateral, but typically present unilaterally. For entities that are usually present bilaterally, see the next section.
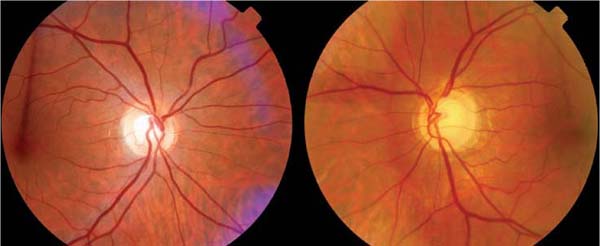
FIGURE 12–2 A 66-year-old woman referred for optic nerve patlor OD. Normal vision and color vision OU. No relative afferent pupillary defect. IOL OD and nuclear sclerosis OS. Follow-up visual field normal OU. Note the difference in coloration of the retina. The pseudophakia is causing a false appearance of pallor OD.
QUESTIONS TO ASK AND POINTS TO KEEP IN MIND
1. Is the patient sure that vision hasn’t changed?
2. How did the visual loss occur?
3. What was the patient told caused the visual loss?
4. Review of prior records is often helpful.
5. Optic nerve appearance may assist in sorting out the category of optic neuropathy.
6. Look for pattern of pallor/atrophy, presence of vascular attenuation, and gliosis.
7. Remember to carefully view the other nerve.
Red Flag
 Any patient with unexplained optic neuropathy in whom progression is uncertain or follow-up is unpredictable should undergo neuroimaging. The previous diagnosis may have been erroneous.
Any patient with unexplained optic neuropathy in whom progression is uncertain or follow-up is unpredictable should undergo neuroimaging. The previous diagnosis may have been erroneous.
PRIOR ACUTE OPTIC NEUROPATHY
An episode of optic neuropathy usually results in the appearance of disc pallor several weeks later. This disc pallor is permanent. Therefore, the presence of static disc pallor is often a sign of a distant optic neuropathy, or one that is started at least several weeks before examination.
PRIOR NONARTERITIC ANTERIOR ISCHEMIC OPTIC NEUROPATHY (NAION)
Classic Presentation
• Typically person over 50 years of age with prior altitudinal visual field defect with matching altitudinal optic nerve pallor and/or atrophy
• History of acute painless visual loss with slight or no recovery
• Vessels may be attenuated and gliotic.
• May have small cup-to-disc ratio (“disc at risk”) in unaffected eye. This small crowded nerve is found more often in younger patients (Fig. 12–3).
• Patients may have a higher incidence of high cholesterol, hypertension, diabetes, and hypercoagulable state.
For further information, see Chapter 19.
PRIOR ARTERITIC ANTERIOR ISCHEMIC OPTIC NEUROPATHY (AAION)
Classic Presentation
• History of rapid loss of vision in one or both eyes
• Age greater than 60
Symptoms of giant cell (temporal) arteritis: headache, scalp tenderness, pain on chewing (jaw claudication), weight loss, anorexia, proximal myalgia
FIGURE 12–3
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


