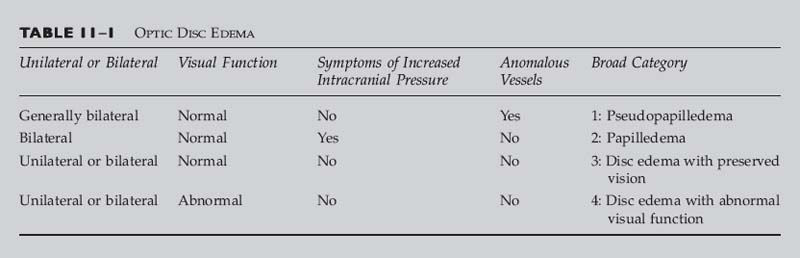
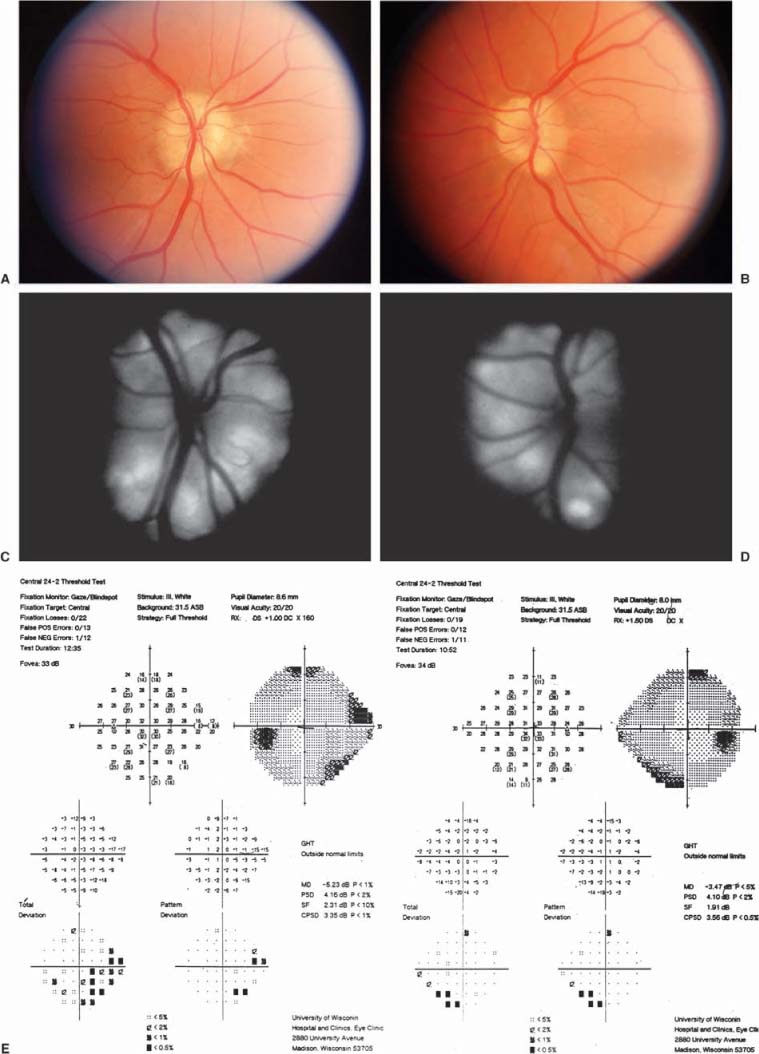
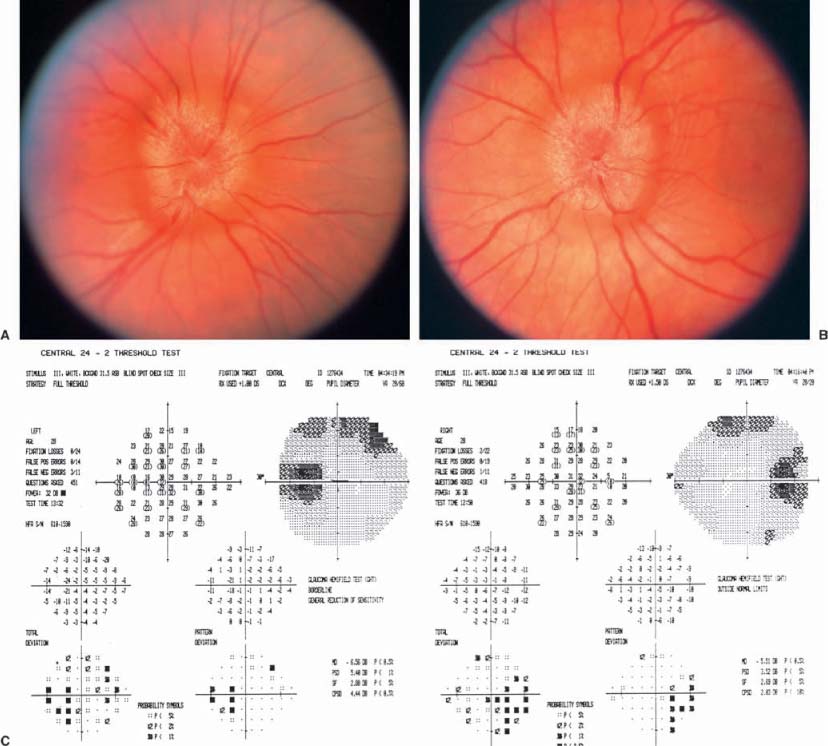
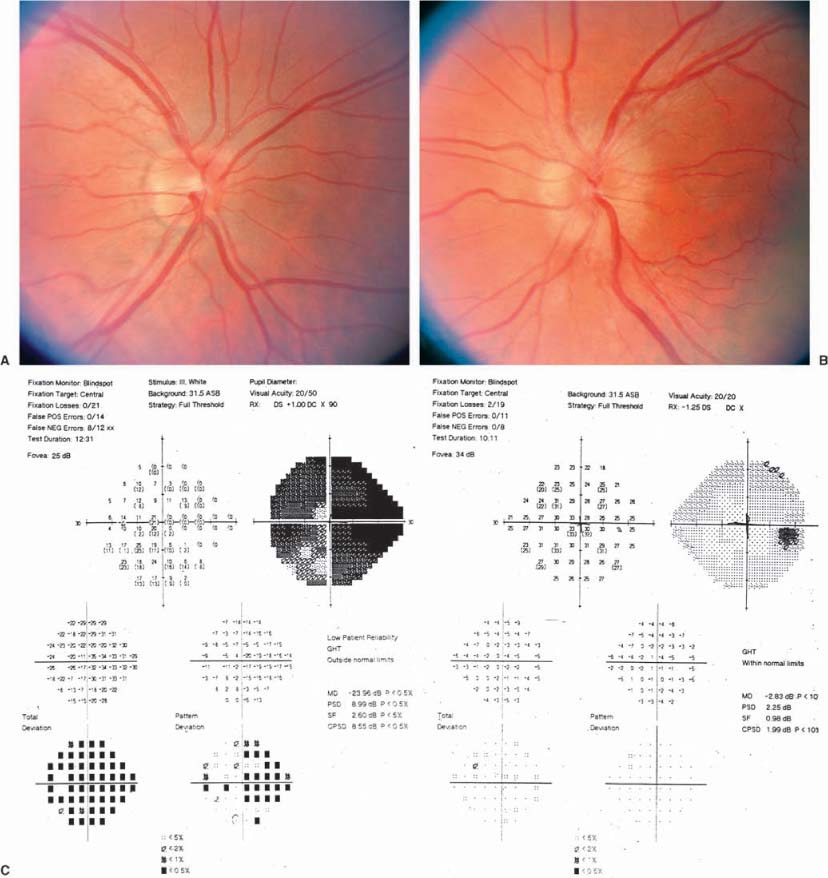
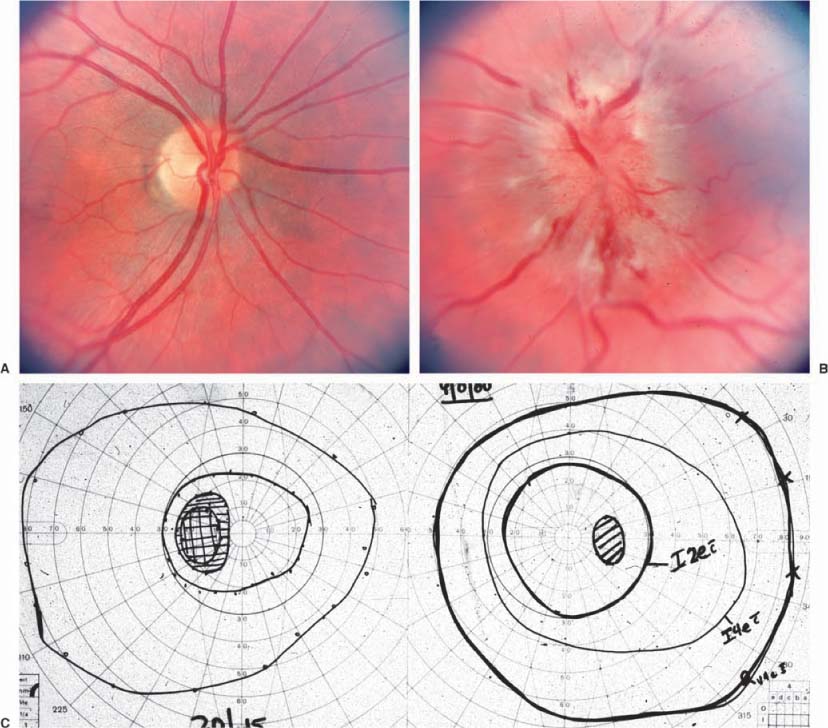
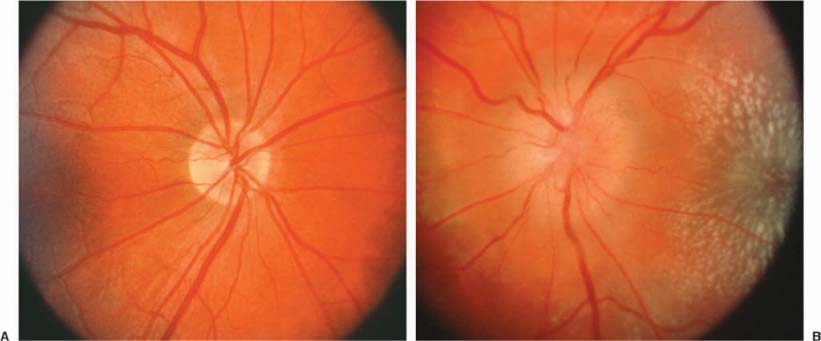
Chapter 11 Several disorders can simulate optic disc swelling, and numerous conditions can cause it. Table 11–1 lists the possible conditions that result in optic disc edema. This chapter is intended to help clarify the nature of the problem when the physician observes that the optic disc is swollen. Clinically distinguishing among the various causes of optic disc swelling requires careful review of the history and the elements of the eye examination (see Section I). The history should clarify whether or not there is subjective vision impairment, either transient or persistent. If persistent, was the onset abrupt or gradual? Is the disorder unilateral or bilateral? Is eye pain or headache a symptom? Are there associated systemic or neurologic diseases? Have there been symptoms of increased intracranial pressure such as headache, transient visual obscurations on standing, pulsatile tinnitus, or nausea and vomiting? Has there been any indication of an orbital disorder? The examination should indicate the level of mental alertness of the patient and the systemic blood pressure. The status of the vision, by measuring the best corrected visual acuity, the color vision, and the visual fields, is important in clarifying the problem. It is important to recall that there can be substantial impairment of vision without reduction of visual acuity. Observing the briskness of the pupil reaction to light helps estimate the function of the optic nerve. Evaluation for possible orbital abnormalities would include assessing exophthalmometry, orbital resiliency, and the presence of an orbital or cranial bruit. At times, performing fluorescein angiography to assess the circulation to the optic disc is of value. Although normal discs have late staining of the disc itself, extension of the leakage beyond the optic disc margins indicates pathologic swelling. Are there anomalous vessels on the disc surface that produce more than two branches of a parent vessel (trifurcations or tetrafurcations)? Table 11–1 indicates possible diagnostic considerations when there appears to be optic disc edema. The initial issue to resolve is whether there is truly pathologic acquired swelling of the disc, or just that the disc itself is congenitally elevated, that is, “pseudopapilledma,” best typified by optic nerve drusen. The lack of obscuring of the vessels as they pass over the edge of the elevated optic disc is a reliable indicator that the elevated disc is an anomaly, and that the disc is not pathologically swollen. The presence of anomalous vessels on the disc is common in pseudopapilledema. If the disc is truly swollen, the task then is to determine if it is papilledema (due to increased intracranial pressure) or another cause of optic disc edema. • The patient may be asymptomatic or have any symptom that is unrelated to the optic nerves (Fig. 11–1). • Can be unilateral (32%) or bilateral (68%), and occurs in all age groups. • Visual acuity is almost always normal, but nerve fiber bundle visual field defects are common. • A relative afferent pupil defect can occur if the optic nerve dysfunction is greater in one eye than in the other. • Small hemorrhages on the optic disc surface can rarely occur, and rarely peripapillary choroidal neovascularization can develop that may require laser photocoagulation. • The suspected presence of optic disc drusen can be confirmed by the presence of autofluorescence of the disc with fundus photography (Fig. 11–1c,d), or by demonstrating the drusen with ultrasonography or computed tomographic (CT) scans. • Some optic discs can be elevated despite our inability to demonstrate drusen, and either represent “buried” drusen deeper in the nerve, or simply more optic nerve tissue than normal, which is a congenital anomaly of the disc. Persons with congenital tortuosity of the retinal vessels or with substantial hyperopia also can have elevated discs that are not pathologically swollen. • The patient may be asymptomatic or have any symptom that is unrelated to the optic nerves. • The patient is hyperopic. • There is normal visual function. • The discs are elevated, but there are no hemorrhages, obscuration of the vessels as they cross the disc margin, engorged veins, or cotton wool spots. When it is evident that there is pathologic optic disc swelling with obscured vessels, and perhaps associated hemorrhages and/or exudates, noting whether there is unilateral or bilateral involvement is important. It should be stressed that the term papilledema should be used to indicate optic disc swelling secondary to elevated intracranial pressure (ICP). It is almost always bilateral, and only rarely asymmetric (Fig. 11–2). When there is unilateral optic disc swelling, one considers as possible causes a local optic disc inflammation (the “papillitis” variant of optic neuritis, as opposed to “retrobulbar” optic neuritis) (Fig. 11–3); a vasculopathy such as ischemic optic neuropathy or papillophlebitis (Fig. 11–4); poorly understood inflammatory disorders such as neuroretinitis3 (Fig. 11–5), or the acute idiopathic blind spot enlargement (AIBSE) syndrome,4–6 or a neoplasm (as with an optic nerve sheath meningioma or glioma) (Fig. 11–6);4,5,7 With bilateral optic disc swelling, in addition to papilledema, one considers the possibilities of bilateral involvement with optic neuritis or ischemic optic neuropathy, systemic arterial hypertension, or diabetic papillopathy (Fig. 11–7).7–9 FIGURE 11–1 Optic disc drusen. The right (A) and left (B) optic discs of a 42-year-old woman in July 2000. The possibility of papilledema had been raised at a recent examination. Visual acuity was 20/20 OD and 20/30 OS. Visual field testing (E) showed inferior and nasal deficits, worse in the left eye than the right. The optic discs were mildly elevated, without obscuring of the vessels on the disc surface, and contained numerous drusen that demonstrated autofluorescence (C,D). Subsequent study revealed that she had undergone evaluation at another hospital 23 years prior, when the diagnosis was “pseudopapilledma of the optic discs.” The patient was unchanged in July 2001. • Bilateral, similar optic disc edema with good optic nerve function (Fig. 11–2). • Symptoms of elevated intracranial pressure such as headache, nausea, vomiting, or diplopia due to an esotropia caused by cranial nerve VI dysfunction. • Transient obscurations of vision lasting 5 to 10 seconds, especially with posture changes. • Early in the course, the visual acuity is normal, and visual fields show enlarged blind spots. • Degree of fundus vascular changes (hemorrhages, exudates) relates to rapidity and severity of the rise in ICP. • With protracted and severe papilledema, ischemic insults to the optic nerves can cause inferior nasal visual field defects initially, though generalized peripheral visual field loss and even blindness can occur with severe involvement. FIGURE 11–2 Papilledema. The right (A) and left (B) optic discs of a 28-year-old graduate student with variable headache for a year, and transient obscurations of vision for 6 weeks. Visual acuity was 20/20 OD and 20/60 in the amblyopic OS. Visual field testing (C) showed enlarged blind spots bilaterally. Evaluation revealed marked hydrocephalus. Resolution of the papilledema followed placement of a ventriculoperitoneal shunt. FIGURE 11–3 Papillitis. The right (A) and left (B) optic discs of a 43-year-old woman who had experienced pain with movement of the left eye for 2 weeks, and blurred vision of that eye for 1 week. Visual acuity was 20/20 OD and 20/50 OS. There was a moderate relative afferent pupil defect OS. Visual field testing (C) showed diffusely reduced sensitivity in the central field of the left eye, especially nasally. The right optic disc was normal, and the left was mildly swollen. Without treatment, the patient subsequently had improvement of the visual field abnormality and pupillary sluggishness, though the visual acuity remained impaired a year later. FIGURE 11–4 Papillophlebitis. The right (A) and left (B) optic discs of a 28-year-old graduate student who had a 10-day history of painless mild blurring of the left eye in 9/80. Visual acuity was 20/15 in each eye, and the pupils reacted equally without a relative afferent pupil defect. Visual field testing (C) showed a mildly enlarged blind spot OS. The right optic disc was normal, and the left was 2 to 3 diopters elevated with peripapillary hemorrhages and cotton wool spots. After a brief time of observation, treatment with prednisone was followed by rapid resolution of the optic disc swelling and vision symptoms. Twenty years later, the visual acuity was 20/20 in each eye, and there was only equivocal pallor of the left optic disc. Though the patient had developed regional enteritis several years after the papillophlebitis, no definite cause for the ocular disorder was established. FIGURE 11–5
OPTIC DISC EDEMA
BROAD CATEGORY 1: PSEUDOPAPILLEDEMA
OPTIC DISC DRUSEN (SEE CHAPTER 23)
Classic Presentation1,2
HYPEROPIC DISCS
Classic Presentation
Red Flag
 The presence of any additional fundus abnormalities should prompt pursuit of an alternative diagnosis.
The presence of any additional fundus abnormalities should prompt pursuit of an alternative diagnosis.
BROAD CATEGORY 2: PAPILLEDEMA
PAPILLEDEMA
Classic Presentation
Red Flags
 The diagnosis of pseudotumor cerebri as the cause for papilledema should not be made until neuroimaging excludes the possibilities of hydrocephalus, a mass, or a dural venous sinus thrombosis, and a lumbar puncture reveals an elevated ICP with normal cerebrospinal fluid10 (see Chapter 17).
The diagnosis of pseudotumor cerebri as the cause for papilledema should not be made until neuroimaging excludes the possibilities of hydrocephalus, a mass, or a dural venous sinus thrombosis, and a lumbar puncture reveals an elevated ICP with normal cerebrospinal fluid10 (see Chapter 17).
 In an asymptomatic patient, the presence of true papilledema is uncommon, but normal optic discs do not rule out elevated intracranial pressure.
In an asymptomatic patient, the presence of true papilledema is uncommon, but normal optic discs do not rule out elevated intracranial pressure.
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


