Optic Chiasm
The optic nerves elevate, and move medially as they extend intracranially to form the optic chiasm. The optic chiasm, which is the confluence of the optic nerves, sits approximately 10 mm above the dorsum sellae. At the chiasm, the nasal fibers of each optic nerve that represent the temporal visual field cross to the contralateral optic tract. Temporal optic nerve fibers which represent the nasal visual fields proceed posteriorly along the ipsilateral portion of the optic chiasm to join the crossing nasal fibers to form the ipsilateral optic tract. Posterior to the optic chiasm, the optic tracts are comprised of ipsilateral temporal fibers and contralateral nasal fibers.
Several anatomic features of the chiasm contribute to the specific types and patterns of visual field defects that occur with lesions in this region. Given that optic chiasm lies 10 mm above the roof of the pituitary fossa pituitary microadenomas do not produce visual field defects. The macular fibers, which comprise 90% of the optic fibers, cross in the posterior aspect of the chiasm. Inferior retinal fibers which represent the superior visual field are located in the inferior portion of the optic chiasm.
The position of the chiasm influences the pattern of visual field loss produced by lesions in the parachiasmal area. The most common position (approximately 80%) for the chiasm is on the diaphragm sellae projecting onto the dorsum sellae. In a prefixed chiasm (15%), the chiasm lies upon the tuberculum sellae or diaphragma sella, while in a postfixed chiasm (5%), the chiasm lies on the dorsum sella posterior to the fossa. The other important structure in the parachiasmal area is the cavernous sinus. The cavernous sinus is comprised of the venous space situated between the meningeal and periosteal layers of the dura mater on either side of the sphenoid bone. It extends from the end of the superior orbital fissure to the apex of the petrous bone. The cavernous sinus contains the carotid artery and the cranial nerves (CN) III, IV, and VI. Parachiasmal tumors may cause visual field defects as well as ocular motility disturbances.
Disorders of the optic chiasm initially may present with visual acuity loss. The clinical demonstration of a chiasmal pattern of visual loss enables the physician to order the appropriate tests and to establish the correct
diagnosis. The single most important nonradiologic test in determining if the optic chiasm is the involved site producing visual loss is the visual field. The confluence of the optic nerves and the crossing of the nasal fibers at the chiasm, combined with the 90-degree rotation that the visual fibers undergo en route to the chiasm from the retina, orient the nerve fibers along the vertical meridian. Therefore, visual field defects at the optic chiasm and posteriorly will characteristically respect the vertical meridian on perimetric testing.
diagnosis. The single most important nonradiologic test in determining if the optic chiasm is the involved site producing visual loss is the visual field. The confluence of the optic nerves and the crossing of the nasal fibers at the chiasm, combined with the 90-degree rotation that the visual fibers undergo en route to the chiasm from the retina, orient the nerve fibers along the vertical meridian. Therefore, visual field defects at the optic chiasm and posteriorly will characteristically respect the vertical meridian on perimetric testing.
TYPES OF VISUAL FIELD ABNORMALITIES IN CHIASMAL DISEASE
Junction Scotoma
Classically, this is a combination of a central scotoma in one eye and a temporal hemianopic defect in the other (Fig. 6-1). The localization of this visual field defect is the junction of the optic nerve, on the side of the central scotoma, and the optic chiasm. The classically accepted cause for this pattern of visual loss is the existence of Wilbrand’s knee, which is the anterior extension of the inferior nasal crossing fibers from one eye into the opposite optic nerve. Therefore, a lesion of the right optic nerve will produce a right central scotoma and a left superior temporal defect. However, modern studies in monkeys have failed to show the anatomic existence of Wilbrand’s knee, despite the fact that the junctional scotoma still is a valid sign that localizes lesions to the junction of the optic nerve and chiasm.
A lesion may involve only the crossing visual fibers at the anterior angle of the optic chiasm. This produces a monocular temporal hemianopic defect with no visual field loss in the contralateral eye (Fig. 6-2).
Bitemporal Hemianopia
It is described in textbooks as the classic visual field abnormality produced by lesions of the body of the optic chiasm. The visual field defects may be complete (Fig. 6-3A) or incomplete (Fig. 6-3B), but they always obey the vertical meridian. In most cases, however, pure bitemporal hemianopic defects are infrequent. Usually, there is decreased acuity in one or both eyes. A central bitemporal defect may occur in patients with prefixed chiasm or posterior growing tumors because the macular fibers are located posteriorly in the chiasm.
Homonymous Hemianopia
A parasellar lesion may produce an incongruous homonymous hemianopia by involving the optic tracts. This may occur with mass lesions that are directed posteriorly or because the optic chiasm is prefixed. The homonymous hemianopia often is associated with a central scotoma and a relative afferent pupillary defect (RAPD) on the side of the mass lesion. This is known as the optic tract syndrome (page 194).
Binasal Visual Field Defect
This is said to occur in a patient with a postfixed chiasm in which the lesion is located between both optic nerves along the anterior aspect of the chiasm displacing the optic nerves laterally against the supraclinoid internal carotid arteries or A1 segments of the anterior cerebral arteries. This is such an extraordinarily uncommon visual field defect that we have never encountered it.
Any patient with decreased vision of unknown etiology requires a visual field. When the visual field shows one of the defects associated with chiasmal involvement, the next test to perform is an MRI scan.
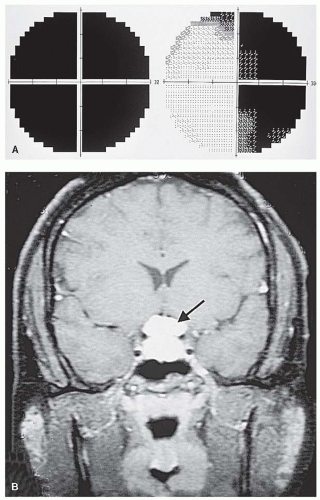 FIGURE 6-1. A. Temporal hemianopic defect in the right eye and central scotoma in the left. B. Causal lesion is perichiasmal mass (arrow). |
 FIGURE 6-2. Patient with a large suprasellar meningioma presented with a temporal hemianopic defect and decreased vision in the left eye with no defect in the right. |
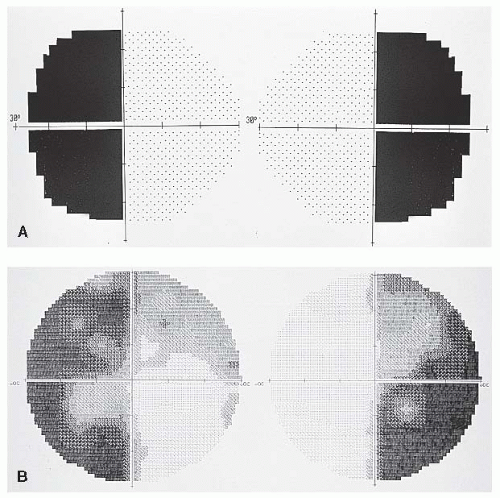 FIGURE 6-3. A. Complete bitemporal hemianopia. B. Incomplete bitemporal hemianopia. |
ETIOLOGY
Approximately 90% of the disorders that produce chiasmal syndromes are mass lesions. The most frequent of these are listed in Table 6-1.
CLINICAL CHARACTERISTICS
Symptoms
Visual loss is the most frequent and most important symptom of parachiasmal disorders; other symptoms may be associated with it but are infrequent in the absence of visual loss.
Headache may be seen with pituitary tumors and implies a stretching of the meninges in the area.
Diplopia: parachiasmal lesions may cause double vision in several ways:
Extension of a mass into either or both cavernous sinuses with involvement of CN III, IV, or VI on one or both sides (Fig. 6-4). This produces a variety of diplopia patterns depending on which CNs are affected.
A form of diplopia without presumed ocular misalignment is the so-called hemifield slide phenomenon. This phenomenon occurs when patients lose the ability to fuse because the bitemporal hemianopia produces a situation where there is no binocular area of overlapping or interlocking visual field. Thus, the eyes can slide in a vertical plane. These patients have difficulty adding a column of numbers because the numbers from one line suddenly appear on the line above or below. It is difficult, however, to explain how this could occur without ocular misalignment.
Postfixation blindness: This is a peculiar type of visual disability that afflicts patients with chiasmal disease. The bitemporal hemianopia causes patients to have an area of blindness immediately beyond the point of fixation when viewing something at near (Fig. 6-5). This occurs because when converging on a point, the area beyond the point of regard falls within the blind bitemporal fields.
Depth perception problems: Patients may complain of difficulty with depth perception, near tasks, or using precision tools.
Photophobia may occur in patients with parasellar tumors. Possible mechanisms postulated include hypersensitivity of trigeminal nerve endings, chemical meningitis or a “central dazzle” due to damage to the hypothalamic-thalamic axis.
TABLE 6-1. Frequency of Pituitary Mass Lesions*
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
|---|