CRANIAL NERVE III PALSY (OCULOMOTOR NERVE)
Cranial nerve III (CN III) innervates the superior, inferior, medial recti, and the inferior oblique muscles. It also innervates the levator palpebrae superioris and carries with it the parasympathetic innervation to the pupil. Involvement of CN III will produce a symptom complex that involves one or several of these muscles and usually results in double vision.
ANATOMY
The subnuclei that give rise to CN III reside in the midbrain. These subnuclei give rise to the fascicles of each of the extraocular muscles. The superior rectus subnuclei are crossed so that the fibers from the left superior rectus subnucleus eventually innervate the right superior rectus muscle. Another peculiarity of the nuclear structure of CN III is that the nucleus for the upper lids is a single midline structure innervating the levator muscles of both lids. The pupillary constrictor and accommodation muscles are under the control of an ipsilateral subnucleus.
As CN III leaves the brainstem near the medial aspect of the cerebral peduncle and enters the subarachnoid space, it travels between the superior cerebellar artery and the posterior cerebral artery next to the tip of the basilar artery. It then travels medially along the posterior communicating (PCOM) artery and lateral along the internal carotid artery. When the nerve enters the cavernous sinus, it lies in the lateral wall superior to CN IV and then goes through the superior orbital fissure dividing into a superior and an inferior division. The superior division contains the superior rectus and levator innervation, while the inferior division contains the rest of the innervation for CN III including the parasympathetic fibers from the ciliary ganglion. There is convincing evidence that the functional organization into a superior and an inferior division occurs before anatomic division occurs in the cavernous sinus.
ETIOLOGY AND PATHOPHYSIOLOGY
Cranial III neuropathy may be caused by a variety of processes, but the most frequent causes are either microvascular infarction of the nerve itself or compression. Microvascular
infarction occurs in older patients (over 50 years of age) and is due to occlusion of the vasa nervorum. This infarction involves the axial portion of CN III. Since the pupillary fibers are on the periphery of the nerve, the pupil is not usually involved by the axial infarction in microvascular disease. These patients often have identifiable risk factors such as diabetes mellitus, hypertension, atherosclerosis, and hyperlipidemia.
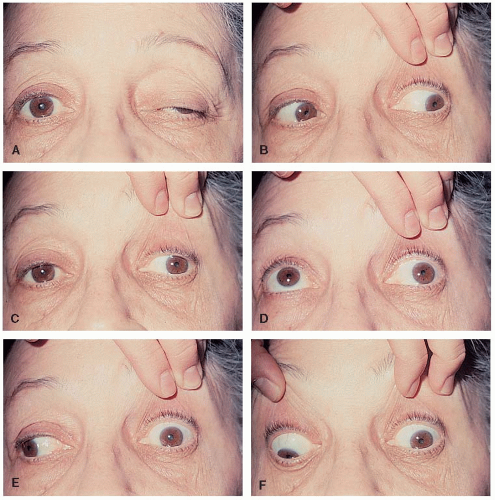
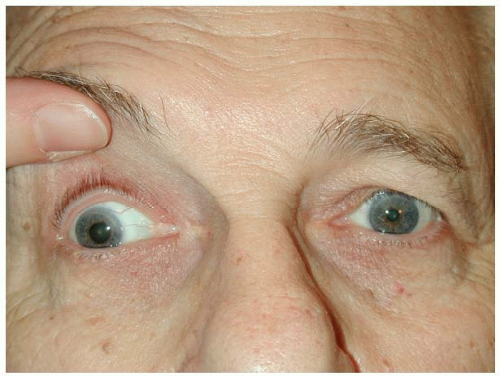
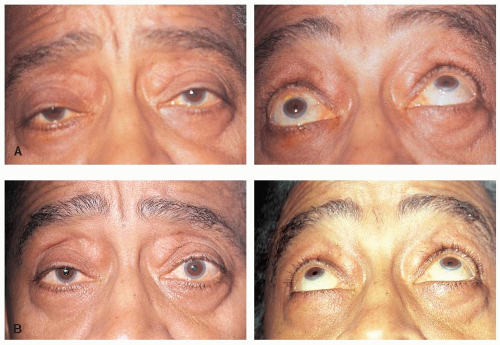
Compressive CN III palsies may be produced by tumors or aneurysms. The clinical syndrome of aneurysmal CN III palsy is an important one because it is a medical emergency. The patient will usually present with a painful (usually, but not always present) isolated CN III palsy. This is usually due to a PCOM artery aneurysm. The aneurysm exerts pressure from the outside; thus the pupillary fibers are often involved early and the CN III palsy is characterized by ptosis, ocular misalignment, and usually, a dilated pupil.
SYNDROMES ASSOCIATED WITH CN III PALSY
Nuclear III Nerve Lesions
• Ipsilateral CN III palsy, contralateral superior rectus paresis (because the superior rectus (SR) muscle is innervated by contralateral subnuclei), and bilateral ptosis (levators innervated by central midline nuclei)
• Bilateral CN III palsies without ptosis
• Bilateral ptosis alone
• Any isolated palsy of a muscle innervated by CN III
CN III Fascicle Syndromes
• Weber syndrome: Ipsilateral CN III paresis with contralateral hemiparesis (involvement of cerebral peduncle)
• Nothnagel syndrome: Ipsilateral CN III paresis and cerebellar ataxia (involvement of superior cerebellar peduncle)
• Benedikt syndrome: Ipsilateral CN III paresis with contralateral hemitremor (involvement of red nucleus)
Lesions in the Subarachnoid Space
• PCOM artery aneurysm: This is the most common cause of an isolated pupil involving CN III palsy with the aneurysm occurring at the junction of the PCOM artery and internal carotid artery.
• Uncal herniation: As CN III travels through the subarachnoid space, it rests on the edge of the tentorium cerebelli with the uncal portion of the temporal lobe above it. A supratentorial mass may cause a downward displacement and herniation of the uncus across the tentorial edge, compressing the nerve. The patient usually has an altered mental status.
Cavernous Sinus Syndrome
• CN III paresis inside the cavernous sinus usually occurs in association with paresis of other CNs (IV, V, or VI).
Orbital Syndromes
• Since CN III divides into a superior and an inferior division as it enters the orbit, involvement in the orbit may result in paresis of structures innervated by either of these divisions.
DIAGNOSTIC EVALUATION
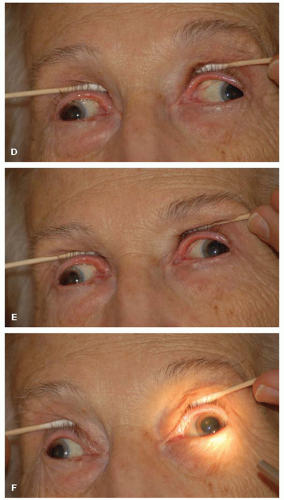
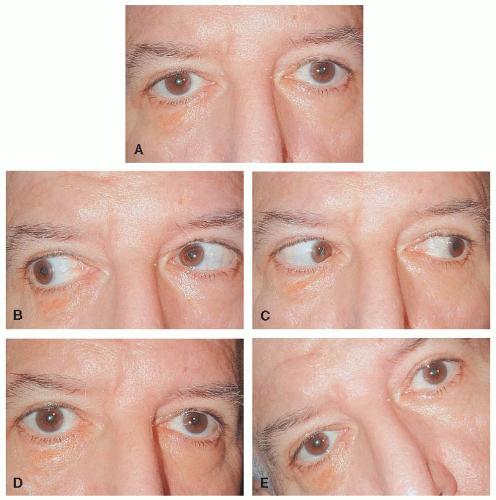
Once CN III palsy has been diagnosed, the next step is to determine whether the palsy is isolated. An associated CN VI deficit is usually easily seen, but an accompanying CN IV palsy may be less obvious. The primary action of CN IV is depression in adduction; however, in the presence of a complete CN III palsy, the eye cannot be adducted to test for CN IV integrity. The determination is made by looking for the secondary action of CN IV, intorsion of the globe. The patient is instructed to look down while the examiner looks for intorsion. Its absence indicates CN IV paresis (
Fig. 10-5).
The investigation of an isolated CN III palsy will depend on the age of the patient, the completeness of the palsy, and the state of the pupil. Guidelines for investigations using these factors are in
Table 10-2.
• Aneurysms are extraordinarily rare in children under 10 years of age, but ophthalmoplegic migraine is a frequent cause of CN III palsies with pupillary involvement; thus, the rationale for subjecting children with CN III palsies to MRI and MRA, but not catheter angiography.
• Patients in the vasculopathic age range with risk factors and no pupillary involvement require investigation to identify those risk factors if none are known to be present, for example, determination of glucose status and blood pressure. In addition, giant cell arteritis may present with any isolated CN palsy; so the patient should specifically be questioned regarding the signs and symptoms associated with giant cell arteritis. ESR/CRP may be helpful if this diagnosis is considered.
• However, if the pupil is involved, the patient should have an urgent MRI/MRA or CT/CTA, and if negative, because the chances of a PCOM aneurysm are still high, we still recommend catheter angiography.
• Patients younger than the vasculopathic age range but older than 10 years require MRI and MRA to rule out tumors or aneurysms even if the pupil is normal. If the pupil is abnormal, however, catheter angiography should be performed even if the neuroimaging is negative. If all imaging tests are unrevealing, then further hematologic and spinal fluid investigations are recommended.
DIFFERENTIAL DIAGNOSIS
• A variety of entities produce ocular motor syndromes that can be confused with complete or partial CN III palsies.
NATURAL HISTORY
• Vasculopathic CN III palsies will resolve spontaneously over a period of 6 to 12 weeks. It is very uncommon for there to be residual diplopia.
• CN palsies due to compression will resolve if the compression is removed or will resolve in a pattern called aberrant regeneration.
• The conditions that should prompt investigation of a CN III palsy under observation are listed in
Table 10-3.
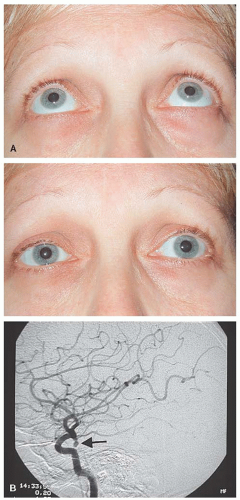
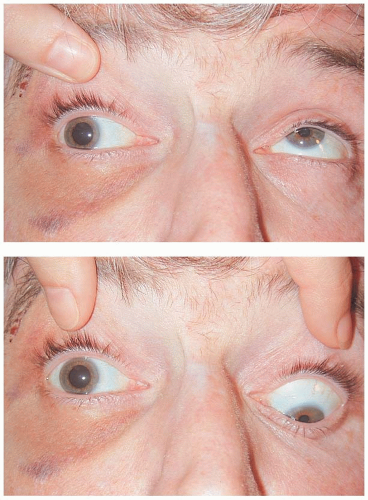
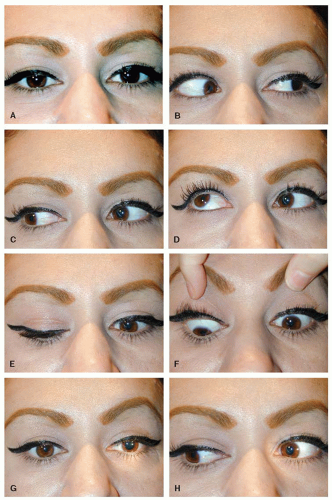
ABERRANT REGENERATION OF CN III
Aberrant regeneration of CN III (
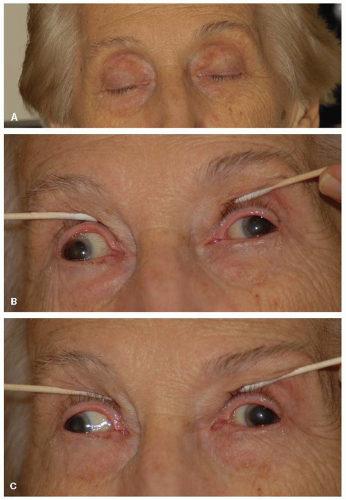
Fig. 10-8), a stereotypic pattern, most often follows an acute CN III palsy due to a PCOM aneurysm or pituitary apoplexy. The ptosis resolves completely or is minimally evident. The eye usually will not elevate or depress well, but adduction usually is restored. Aberrant regeneration can be either lid-gaze dyskinesis or pupil-gaze dyskinesis. In pupil-gaze dyskinesis, some of the medial rectus fibers innervate the pupillary sphincter so that there is more pupil constriction on adduction than to light stimulation (a pseudo-Argyll Robertson pupil). With lid-gaze dyskinesis some of the inferior rectus or medial rectus fibers innervate the levator so that the upper lid elevates on adduction and downgaze fissure. This widening of the interpalpebral fissure on downgaze is known as the pseudo-Graefe sign.
Aberrant regeneration is a pattern of resolution in compressive or traumatic CN III palsies. It should never be attributed to vasculopathic CN III palsy.
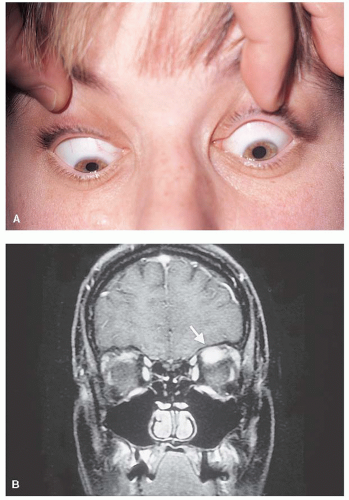
Primary Aberrant Regeneration
Some patients never experience acute CN III palsy but develop a slowly progressive form of CN III aberrant regeneration. Slow growing compressive lesions, usually within the cavernous sinus, produce this syndrome. These lesions are usually meningiomas or cavernous sinus aneurysms, although other causes have been reported.
CRANIAL NERVE IV PALSY
Cranial nerve IV (CN IV) innervates only the superior oblique muscle, which depresses the eye in adduction and intorts the eye. CN IV is the only CN that exits the brainstem dorsally, and it has the longest intracranial course. It also decussates so that the right nucleus of CN IV will eventually innervate the left superior oblique muscle. CN IV is enveloped in the anterior medullary velum where it is vulnerable to head trauma.
ETIOLOGY
• Head trauma
• Microvascular infarction
• Congenital
• Other causes such as tumors, multiple sclerosis, and inflammation are less frequent
SYNDROMES ASSOCIATED WITH CN IV PALSY
• Nuclear-fascicular lesions: CN IV palsy with a contralateral Horner syndrome since the sympathetic pathways descend through the midbrain adjacent to the trochlear fascicles.
• Subarachnoid space lesions: Usually produces an isolated CN IV palsy; bilateral CN IV palsies may occur when the site of injury is at the anterior medullary velum.
• Cavernous sinus lesions: CN IV palsy is seen in combination with CN III palsy. To diagnose CN IV paresis, the patient should be
instructed to abduct the eye and then asked to look down. The ability of the eye to intort in this position is an indication of intact CN IV function.
• Orbital lesions: In the orbit, CN IV palsy occurs in conjunction with other CN palsies as well as other features of orbital disease such as proptosis, chemosis, or conjunctival injection.
DIAGNOSTIC EVALUATION
In the presence of isolated CN IV palsy, a history of head trauma should be sought. In the absence of history of head trauma, isolated CN IV palsy in a patient over 50 years of age is assumed to be vasculopathic in nature. Patients younger than the vasculopathic age group should undergo neuroimaging. Patients over the age of 55 years should be investigated for giant cell arteritis. Congenital CN IV palsies may become manifest later in life. These patients complain of intermittent diplopia that becomes more frequent and more prolonged. Examination reveals increased vertical fusional amplitudes, which establishes the diagnosis of a congenital process. Examining old family photographs likewise may reveal a long-standing head tilt, another clue to the congenital nature of the strabismus. In patients with increased vertical fusional amplitudes, no further investigations are required. Vertical fusional amplitudes should be measured in all patients with CN IV palsy.
NATURAL HISTORY
• Patients in the vasculopathic age group with an isolated CN IV palsy and normal vertical fusional amplitudes require investigation for risk factors (e.g., diabetes mellitus and hypertension). These patients may then be observed since most of these palsies will resolve spontaneously within 6 to 12 weeks.
• Patients with traumatic CN IV palsies may also be observed. The misalignment, however, may take longer to resolve.
BILATERAL CN IV PALSIES
Trauma often produces bilateral CN IV palsies. The bilaterality of the process may be masked and patients will sometimes appear to have a unilateral palsy. Clues to bilateral involvement include the following:
• Large cyclorotational misalignment: Patients with an apparent “unilateral” CN IV palsy but with excyclotorsion greater than 10 degrees should be suspected of having bilateral CN IV palsies.
• V-pattern esotropia
• Alternating hypertropia (right hypertropia on left gaze and left hypertropia on right gaze)
SKEW DEVIATION
Askew deviation is a vertical/torsional strabismus caused by a supranuclear lesion which must be differentiated from CN IV palsy. It is usually caused by a lesion in the prenuclear vestibular inputs to the oculomotor nuclei. It may be part of a full ocular tilt reaction (see below). Characteristics of a skew deviation include the following:
• Comitant or incomitant vertical misalignment
• With lower brainstem lesions the ipsilateral eye is usually hypotropic while with pons or
midbrain lesions the ipsilateral eye is hypertropic. An alternating skew is characteristic of cerebellar degeneration with the abducting eye being hypertropic.
• The upright-supine test: A vertical deviation that decreases by 50% from the upright to supine position suggests skew deviation.
• Rarely, it may alternate with eye position so that there is right hypertropia in right gaze and left hypertropia in left gaze.
• Skew deviation may be associated with the ocular tilt reaction which is the triad of the following:
Skew deviation
Ocular torsion—such that the upper poles of both eyes rotate in the same direction as that of the head tilt (i.e., the hypotropic eye is excyclotorted and the hypertropic eye incyclotorted). This is the opposite of the physiologic counterroll during which the upper poles of both eyes rotate in the opposite direction to that of the head tilt.
Head tilt—the pathologic head tilt is ipsilateral to the hypotropic eye.



 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access
