be read by a person with normal vision at 20 feet (6 m). The largest letter should be seen at 200 feet (60 m) by a person with normal vision. If a patient can see that letter at a distance of 20 feet and is unable to see any of the smaller letters, vision is 20/200. If the line read by a person with normal sight can be seen at 20 feet, and the patient is 20 feet from the chart, the vision is 20/20. If the patient is unable to read the largest letter on the chart, the distance at which he or she can count fingers accurately is recorded. If the patient cannot count fingers, the distance at which hand movements are perceived is determined. If this is not possible, whether the patient can perceive light is documented. Table 14.1 compares visual acuity with visual ability or disability. Vision is not a true fraction. In other words, 20/40 vision does not mean 50% of normal vision but that the patient can see at 20 feet what a person with normal sight can see at 40 feet (12 m). If the patient can see the 20/20 line by wearing glasses, his or her functional vision is probably just as good as that of someone who sees the line without glasses.
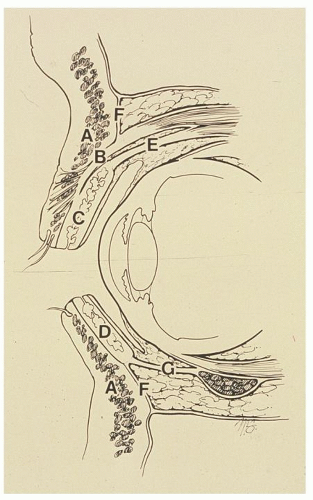 Figure 14.1 Cross-sectional anatomy of the orbital adnexae and globe: (A) orbicularis oculi muscles, (B) levator aponeurosis, (C) upper tarsal plate, (D) lower tarsal plate, (E) Mueller muscle, (F) orbital septum, and (G) lower eyelid retractors. Courtesy of the American Academy of Otolaryngology-Head and Neck Surgery, Inc. From: Holt JE, Holt GR. Ocular and orbital trauma 1983:10. |
reacts to accommodation but not to light, it is the classic Argyll Robertson pupil, often associated with syphilis. A Marcus Gunn pupil is an important physical sign in the evaluation for neurologic disease. It is elicited with the swinging flashlight test. Light is shined in one pupil for 2 or 3 seconds and then rapidly swung back and forth between eyes. Prompt constriction should appear if each pupil is normal. If optic nerve disease or injury is present in the affected eye, the pupil gradually dilates, indicating a decreased direct light reflex. With an impaired neural connection in the affected eye, the examiner will observe a diminished pupillary response in both eyes when the normal eye is stimulated. Thus, the direct response to stimulation of the affected eye and the consensual response in the normal eye are both reduced, compared to the responses when the normal eye is similarly stimulated. Such a reaction usually indicates damage to the optic nerve via the afferent pupillary fibers. This sign is positive early in optic nerve disease, when vision still is 20/30 or better. Abnormal pupillary reaction in any form generally indicates a serious eye disease. For the otolaryngologist, normal visual acuity and normal pupillary responses are comforting findings in evaluating eye problems.
TABLE 14.1 CORRELATION OF VISUAL IMPAIRMENT WITH VISUAL DISABILITY | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||
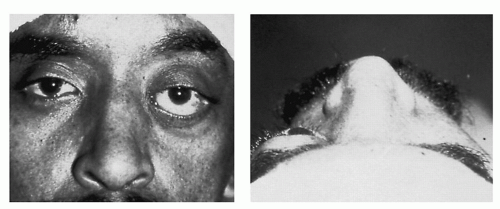 Figure 14.2 Proptosis of the left eye, viewed from anterior (left) and superior (right) positions. |
 Figure 14.3 Heterotropia is characterized by gross asymmetry of eye movement. |
the ophthalmoscope with a 16 diopter lens at a distance of approximately 1 foot (0.3 m). Any alteration in the red reflex indicates abnormality in one of the optical structures of the eye and is always important. The patient’s eye is then approached as closely as possible as the power of the lens in the ophthalmoscope is reduced until the optic disk comes into focus. The nerve head, at the back of the eye, should be evaluated for color, sharpness of margins, and appearance of the central depressed area, known as the cup. Systematic examination of the retinal vessels and background then is performed. The macular region deserves special attention for patients with vision loss. This examination is performed on both eyes.
and changes in protein content occur, almost without exception, to some degree in every person with increasing age; however, the loss of transparency can be so marked that visual function is seriously hampered. The term cataract usually is reserved for the latter situation. Cataract formation usually is evolutional, but it occasionally has a specific cause, such as galactosemia, galactokinase deficiency, diabetic ketoacidosis, postradiation therapy, or trauma. If a metabolic abnormality can be corrected early in the course of cataract formation, some lens opacity can be reversed; however, there is no known reversal of lens changes due to senile cataract. Treatment is surgical removal of the cataract. The need for surgery usually depends on the patient’s visual requirements and desires. In rare instances, the cataract damages the eye because of high pressure from rapid swelling and may have to be removed for other than optical reasons.
diagnosis, length of time detached, and avoidance of late surgical complications.
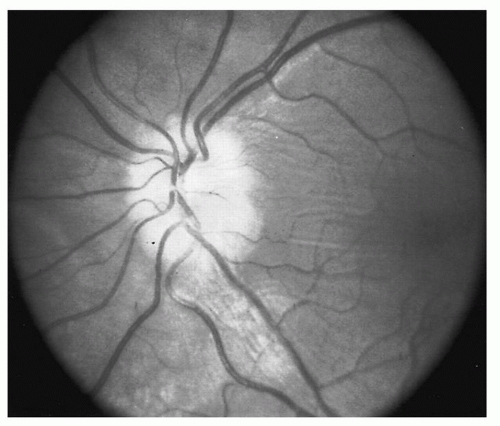 Figure 14.4 Edema of the optic disk indicates optic neuritis. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


