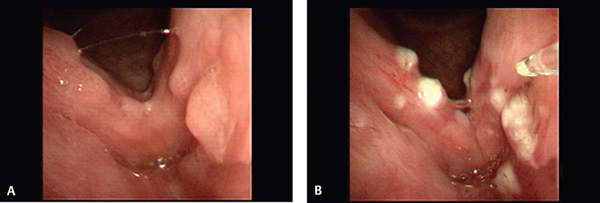
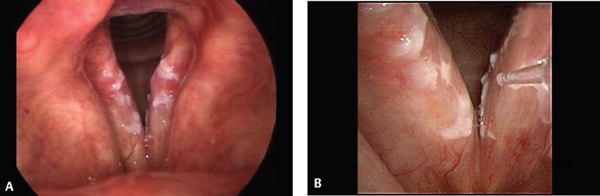
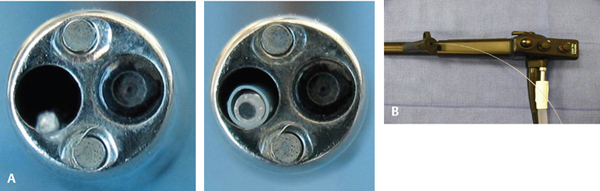
9 Office Procedures in Laryngology: Office-Based Laryngeal Laser Surgery with Local Anesthesia Office-based transoral laryngeal surgery was performed initially and routinely in surgeons’ offices in the 19th century. Migration to the operating room in the early 20th century occurred with direct laryngoscopic surgery, which was optimized by assistants administering anesthesia and procedural support. Improvements in imaging provided by the surgical microscope, along with hemostatic cutting facilitated by the carbon dioxide laser, anchored precise endolaryngeal surgery to the operating theater. Recent advancements in distal-chip flexible endoscopic technology and fiber-based lasers have allowed for the creation of office-based laryngeal laser surgery, which was first instituted in 2001 and first presented at the American Laryngological Association in 2003.1 Fig. 9.1 shows a patient undergoing office-based flexible laryngoscopic laser surgery with topical local anesthesia. In this minimally invasive approach, an assistant holds the laser fiber as it courses from the laser to the side-port working channel of the flexible laryngoscope and the surgeon observes the surgical field on the monitor. Our current treatment strategies using office-based laryngeal laser surgery are primarily limited to treatment of benign epithelial proliferative disorders such as dysplasia and papilloma. Precise microsurgery of phonatory mucosa (nodules, polyps, cysts, ectasias, and varices) is optimally managed by means of general anesthesia with stereoscopic magnification and bimanual dissection to maximally preserve the normal overlying epithelium and underlying superficial lamina propria (SLP). Fiber-based lasers currently widely utilized in office-based laryngeal laser surgery include the selective photoangiolytic 532-nm potassium-titanyl-phosphate (KTP) pulsed laser2 and the ablative 2013-nm continuous-wave thulium laser.3 Figure 9.1 Office-based treatment of a patient with glottic papillomatosis, using pulsed potassium-titanyl-phosphate laser. The laser fiber (green due to a pulse of 532-nm laser energy) is passed through the side-port working channel of a flexible laryngoscope. In the 1980s, Anderson et al4–6 proposed concepts of selective photothermolysis that allowed for specific targeted damage to cells by “suitably brief pulses” of optical radiation based on properties of the target tissue. Anderson, a dermatologist, applied selective photothermolysis to the development of yellow light (585 to 600 nm) pulsed-dye laser (PDL) for the treatment of vascular malformations by targeting oxyhemoglobin.6 This concept eventually evolved into two angiolytic lasers: the 585-nm PDL and the 532-nm pulsed KTP laser. These wavelengths are precisely selected to target absorbance peaks of oxyhemoglobin (~571 nm and ~541 nm) and can fully penetrate intraluminal blood and deposit heat uniformly into the vessel, thereby causing intravascular coagulation and “photoangiolysis” of the subepithelial microcirculation. The short pulse width is precisely selected to contain the heat to the vessel without causing collateral damage to the extravascular soft tissue from heat conduction. The output of these lasers is transmitted through a thin flexible glass fiber (≤ 0.6 mm). When applied to vocal folds, the precise coagulation of subepithelial microcirculation within the layered microstructure of the phonatory mucosa has since been shown to be an effective strategy to treat papillomatosis,2,7–12 dysplasia,13–15 and microvascular angiomata.16–18 The KTP laser has also been demonstrated to be effective for treating early glottic cancer.19,20 Photoangiolytic lasers, which were originally used by our group over 10 years ago to facilitate microflap resection of vocal fold dysplasia, are now used routinely in office-based laryngeal surgery to involute premalignant laryngeal disease and papilloma without resection.2,15 Fig. 9.2 shows vocal folds with diffuse dysplasia (Fig. 9.2A) being treated in the office setting with pulsed KTP laser photoangiolysis (Fig. 9.2B). The selectivity of photoangiolytic lasers leads to improved vocal outcomes by allowing for aggressive treatment of dysplasia and papilloma with maximum preservation of the layered microstructure of the vocal fold including the SLP. Figure 9.2 (A) Rigid transoral examination showing diffuse bilateral vocal fold dysplasia with keratosis (white) and erythematous (red) regions. (B) This same patient is undergoing office-based pulsed potassium-titanyl-phosphate laser photoangiolysis via transnasal endoscopy. Note the laser fiber (right side of image) treating disease on the medial surface of the left vocal fold. Our current treatment strategies using office-based laryngeal laser surgery are limited to the treatment of dysplasia and papilloma, and we do not favor the use of office-based techniques in the management of malignancy, microvascular angiomata, benign phonotraumatic lesions such as polyps, or chronic inflammatory conditions such as polypoid corditis unless the patient’s medical comorbidities prohibit general anesthesia.21,22 Office-based laryngeal laser surgery sacrifices a certain degree of precision due to the loss of binocular visualization, high-powered magnification, and an immobile and insensate operative field that exists when surgery is performed in patients who are under general anesthesia. Office-based laryngeal laser surgery is advantageous in cases of recurrent dysplasia and papilloma due to the avoidance of multiple general anesthetics and the ability to treat regrowth of disease more often with less recovery time. Dysplasia and papillomatosis are the two most common indications for photoangiolysis using pulsed KTP laser, both in the operating room and in the office.23 Our current strategy is to treat patients initially in the operating room where the extent of epithelial disease and the prior surgically induced soft-tissue changes can be adequately assessed. The KTP laser has proven its utility in ablating disease with maximum preservation of the underlying SLP, and this laser is used in almost every patient with dysplasia or papilloma. Fig. 9.3 shows a patient with recurrent laryngeal papilloma (Fig. 9.3A) who presents for office-based pulsed KTP laser photoangiolysis (Fig. 9.3B) after previously undergoing surgery in the operating room under general anesthesia. Subsequent treatments are done in the office depending on patient tolerance and preference, extent of disease, and location of the disease. Office-based KTP laser use for dysplasia and papilloma is primarily for disease on the superior and medial glottic surfaces as well as in the supraglottis. Disease on the inferior surface of the vocal folds and subglottis is harder to treat in the office setting. These patients require extended follow-up to detect recurrent disease. Even though office-based pulsed KTP laser ablation is sometimes less effective than similar photoangiolytic treatment in the operating room, due to time constraints associated with topical anesthesia, posttreatment dysphonia is often diminished as well. Although this treatment strategy often results in more frequent procedures (and therefore more total cases) due to limitations of the therapeutic window provided by topical anesthesia, patients are able to avoid the risks of multiple general anesthetics. Figure 9.3 (A) Transnasal distal-chip scope endoscopy of a patient with diffuse vocal fold and supraglottic recurrent papilloma. (B) This same patient is undergoing office-based pulsed potassium-titanyl-phosphate laser photoangiolysis of papilloma. Note the characteristic white blanching of the disease that has already been treated. The laser fiber (right side of image) is being withdrawn after treating supraglottic papilloma. Recently, a 2013-nm continuous-wave laser was developed to simulate the cutting properties of the carbon dioxide laser.3 The RevoLix laser (LISA Laser Products, KatlenburgLindau, Germany) is a diode-pumped solid-state laser that has a thulium-doped yttrium-aluminum-garnet laser rod that produces a continuous-wave beam with a wavelength of 2013 nm. This wavelength has a target chromophore of water, making it an effective laser for hemostatic cutting. A distinct advantage of the thulium laser is its glass fiber delivery system, which allows for tangential endoscopic dissection as well as office-based use through a flexible fiberoptic laryngoscope. Our preliminary use with the thulium laser during endoscopic partial laryngectomy procedures in both the glottis and the supraglottis3,24 revealed that this laser created effective hemostasis with increased thermal damage on the soft tissues at the margin of the cancerous section as compared with the carbon dioxide laser, although this degree of thermal damage did not seem excessive. While there is not a significant need for nonselective ablation of laryngeal lesions in the office-based setting, there are occasional indications where patients would benefit from this technique. We have used the thulium laser through the flexible laryngoscope to perform ablation of diffuse recurrent respiratory papillomatosis and lesions of the larynx apart from the phonatory membranes.3 Often these are patients who require multiple procedures for severe, extensive disease or who are poor candidates for general anesthesia and require ablation of a lesion where precise preservation of the vocal fold layered microstructure is not of major concern. Patients undergoing office-based laryngeal laser surgery require optimal anesthesia of the entire upper aerodigestive tract. Timing is important during delivery of topical anesthesia to ensure that treatment commences shortly after maximum anesthesia is achieved. There is generally a small therapeutic time period during which patients can be treated before they start to react to the lasering with increased secretions and discomfort. In some cases, it is helpful to have patients take Valium (diazepam, 5 mg, taken orally 30 minutes before the procedure) or the equivalent antianxiolytic before beginning office-based surgery. Most patients tolerate office-based laryngeal laser surgery quite well, and it is unusual to have the patient undergo general anesthesia solely on the basis of tolerance of the procedure.25 The nasal passage is decongested and anesthetized by spraying a mixture of Neo-Synephrine (phenylephrine) and Topicaine (lidocaine) transnasally. Butamben (cetacaine) spray is judiciously applied to the tongue base and soft palate. Patients are then asked to inhale an atomized solution of 4% lidocaine to begin to directly numb the glottis. Final anesthesia at the target treatment site or sites within the larynx is achieved by directly dripping up to an additional 4 mL (in adult patients) of 4% lidocaine onto the treatment site under direct visualization of the transnasal scope. Treatment should begin within 5 to 10 minutes of application of the topical anesthetic to ensure a maximum period of time for lasering before secretions accumulate and patients’ tolerance for the procedure diminishes. For office-based surgery, a flexible laryngoscope with suction and a side-port working channel is necessary to deliver the laser fiber to the target tissue. A small fiber size is desirable because the fiber lies within the suction port, and large fibers can make suctioning of thick secretions difficult (Fig. 9.4A, B). Basic surgical principles are the maximum reduction of disease with preservation of the vocal fold with little or no scarring. In adults, surgical intervention is often done solely for voice-related symptoms, unlike the concern for airway obstruction that is the predominate reason for surgical management of pediatric patients. Fig. 9.1 depicts the typical office-based setup for the treatment of laryngeal papilloma in an awakened patient with topical anesthesia. 1.Patients are seated in a standard otolaryngologic examination chair and the optimal height is adjusted for the operating surgeon. It is helpful to place a pillow behind the patient’s back to provide comfortable padding against which they may brace themselves. 2.After adequate topical anesthesia is achieved, transnasal flexible laryngoscopy is performed with a scope that contains both suction and a side-port working channel. 3.The laser fiber is delivered through the side-port working channel of the flexible scope and used to treat the disease in both contact and noncontact modes. Treating laryngeal papilloma in an awakened patient is less precise than when the patient is under general anesthesia due to the patient’s respiration and occasional swallowing. However, when using the KTP laser, the selectivity of this laser to be preferentially absorbed by the more vascular papilloma ensures optimal treatment of disease. 4.Disease is treated to the endpoint of white blanching (indicating that the intralesional vasculature has been coagulated). Bulky exophytic disease can be suctioned away. The base of the treatment site can then be treated again with laser energy. 5.Lasering continues until all visible disease has been adequately treated or until patients’ tolerance and increased secretions prohibit further lasering. Figure 9.4 (A) The distal flexible laryngoscope revealing the 2-mm working channel with laser fibers and sheaths. Note that the 0.4-mm potassium-titanyl-phosphate laser fiber (left) with its sheath allows for substantially more area to suction secretions and blood than the larger (0.6-mm) pulsed-dye laser fiber (right) with sheath. (B) The image shows a typical flexible laryngoscope with suction attached (white tubing) and laser fiber being inserted into the side-port working channel.

Selective Photoangiolysis and the 532-nm KTP Laser
Ablation and the 2013-nm Continuous-Wave Thulium Laser
Anesthetic Considerations
Surgical Steps
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


