Office-Based Procedures in Laryngology
Manish D. Shah
Michael M. Johns III
Laryngologic procedures were originally developed over 100 years ago to be done under local anesthetic in the office setting. Medical and surgical advances—such as general anesthesia, endotracheal intubation, and the operating microscope—led to a movement of procedures to the operating room. These advances provided surgeons with the advantages of bimanual dexterity, binocular vision, and high-power magnification and, thus, increased precision. Recently, there has been a resurgence in the popularity of awake office-based laryngeal procedures (1,2,3).
Several technologic advances have facilitated the revival of awake office-based laryngeal procedures. Distal-chip flexible endoscopes, ultrathin esophagoscopes, a variety of injection materials, and fiber-based lasers have all contributed to this trend (1,4).
Conducting laryngeal procedures in an awake patient has numerous advantages. First, awake procedures are substantially more convenient for patients when compared to procedures under general anesthesia or sedation. They may leave the hospital on their own and even return to work the same day. Patient safety is increased by avoiding the risks associated with general anesthesia, which is especially important for patients with significant medical comorbidities.
Second, there are significant advantages for the surgeon. The ability for the patient to phonate allows the surgeon to monitor voice quality before, during, and after the procedure. Furthermore, diseases that were once observed until severe enough to warrant exposing the patients to the inconveniences and risks of general anesthesia, such as glottal leukoplakia/dysplasia or papillomatosis, can be treated as frequently as indicated by clinician concern and patient symptoms.
LARYNGEAL VISUALIZATION
The development of endoscopic technology and illumination has led to improved visualization of the larynx, which is essential to the diagnosis and treatment of laryngeal pathology. Laryngeal videostroboscopy, kymography, and high-speed cinematography are all techniques that allow for detailed examination of vocal fold vibration that cannot be appreciated with standard mirror or fiberoptic laryngeal examination. These topics are covered in more detail elsewhere in this book (see Chapter 65).
For awake office-based procedures, both rigid and flexible endoscopes can be used, as is described in this chapter. Rod-lens endoscopes generally provide superior image quality when compared to flexible fiberoptic endoscopes due to larger and more stable light-carrying fibers. However, the development of flexible endoscopes with a chip-based camera at the end of the scope (“distal-chip”) has led to image quality that is near equivalent in quality to rigid rod-lens scopes (7).
PATIENT SELECTION AND PREPARATION
For the purposes of this chapter, “office-based” implies that the patient is awake, with no or minimal sedation, sitting upright, and able to provide phonatory feedback. Procedures may actually be done in a hospital-based procedure room such as an endoscopy suite, but the advantages of these procedures are realized as long as there is adherence to these principles.
The vast majority of patients will tolerate an awake laryngeal procedure; however, patient preparation is essential. The surgeon must clearly explain the procedure, including the application of topical anesthesia, and gauge the patient’s level of comfort and anxiety. It is essential to explain the abnormal sensations produced by topical
anesthesia of the pharynx and larynx as well as the mild discomfort the patient may feel during the procedure itself. Procedures should not be attempted on patients who seem too anxious to proceed; however, even very anxious patients will tolerate an awake procedure if they are adequately informed ahead of time and coached throughout.
anesthesia of the pharynx and larynx as well as the mild discomfort the patient may feel during the procedure itself. Procedures should not be attempted on patients who seem too anxious to proceed; however, even very anxious patients will tolerate an awake procedure if they are adequately informed ahead of time and coached throughout.
Patients must have a patent nasal airway for passage of a flexible laryngoscope and must be able to tolerate such an examination without an intense gag reflex. Patients who are not able to remain still for the duration of the procedure, such as patients with cervical dystonias or severe head tremor, may be difficult to treat (8). Those on anticoagulants should stop taking these medications prior to injections or biopsies. However, the experience of the authors and of others (3,8) suggests that complication rates are not higher in these patients even if they are unable to stop these medications.
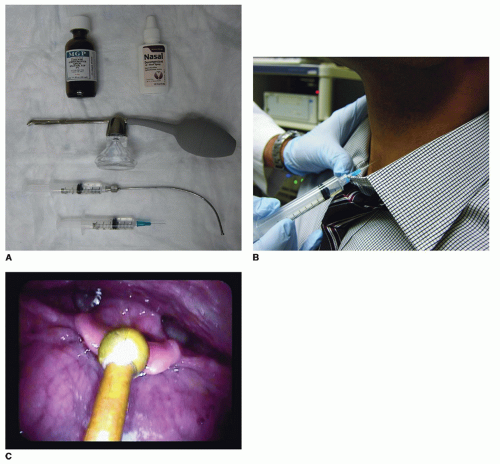 Figure 73.1 A: Equipment and medications required for laryngopharyngeal topical anesthesia. Shown in the photograph are topical 4% lidocaine solution, oxymetazoline, spray bottle to aerosolize medications for nasal anesthesia, Abraham cannula, and syringe with needle for transtracheal injection of anesthetic. B: Transtracheal injection of anesthetic for topical laryngotracheal anesthesia. C: An Abraham cannula is used to drip topical anesthetic onto the larynx. |
ANESTHESIA
Adequate anesthesia of the laryngopharynx is of utmost importance to the success of any awake laryngeal procedure. This can be achieved by either topical application of anesthetic medication or superior laryngeal nerve (SLN) blocks (Fig. 73.1A). Almost always, the former will suffice; however, the latter can be useful in certain patients. Whichever method is used, patients must be instructed to remain NPO for 30 to 45 minutes after the procedure due to the risk of aspiration secondary to laryngopharyngeal anesthesia.
Topical
The nasal cavity should be anesthetized and decongested if a flexible scope is to be used for the procedure. Our preference is to use oxymetazoline and 4% topical lidocaine. The laryngopharynx can then be anesthetized by one of four methods:
Transtracheal injection of 2 to 4 mL of 4% lidocaine into the lumen of the trachea (Fig. 73.1B). This will elicit a strong cough reflex, delivering the lidocaine to the subglottic, glottic, and supraglottic levels. The airway should be entered below the cricoid cartilage as opposed to through the cricothyroid membrane. This avoids the plexus of blood vessels found at the cricothyroid membrane and minimizes bleeding in the larynx, which can obscure structures during the procedure itself. If the patient has a tracheostomy, instillation of the anesthetic through the tracheostomy tube with subsequent occlusion of the tube during the cough will produce a similar effect.
With a flexible or rigid scope used to visualize the larynx, an Abraham cannula (Pilling; Teleflex Medical, Research Triangle Park, NC) can be used to deliver 2 to 4 mL of 4% lidocaine to the base of tongue, epiglottis, and larynx (Fig. 73.1C). A “laryngeal gargle” is performed by having the patient phonate during the delivery of the anesthesia in order to maximize contact time with the laryngeal mucosa (9).
The anesthetic can be delivered via a syringe attached to the working channel of a flexible laryngoscope. As above, a “laryngeal gargle” will maximize effectiveness of anesthesia.
Lidocaine will result in 45 to 60 minutes of anesthesia within 90 seconds of application. However, most patients will only tolerate the procedure for approximately 20 to 30 minutes (1,8). Various topical anesthetic medications may be used as long as the maximum dose guidelines are strictly followed (1,8).
Superior Laryngeal Nerve Block
The site of injection for an SLN block is halfway between the hyoid bone superiorly and the superior border of the thyroid cartilage inferiorly, and halfway between the anterior midline and the superior cornu of the hyoid bone (10). This corresponds to the point where the internal branch of the SLN pierces the thyrohyoid membrane to enter the larynx. One to two milliliters of anesthetic is injected in this area, superficial to the thyrohyoid membrane, to provide a nerve block. The duration of anesthesia will depend upon the agent(s) used. The procedure should be done on both sides of the larynx.
Complications of Topical Anesthesia
Significant complications of topical anesthesia are very infrequent (10). Vasovagal reactions can rarely occur (10), but actual syncope can often be prevented if the prodromal symptoms are recognized. The procedure should be aborted and the patient placed in a reclined position.
Systemic toxicity may result from inappropriately high doses of topical anesthetic agents. Early symptoms can include perioral and tongue paresthesias, visual disturbance, lightheadedness, dysarthria, muscle twitching, and tinnitus. These symptoms must be recognized very early as cardiovascular collapse, convulsions, and cardiorespiratory arrest are possible. This highlights the importance of strict adherence to recommended maximum doses for each anesthetic agent. Dose adjustments may be required in patients with hepatic compromise, renal insufficiency, or heart block.
Allergic reactions are also possible but are usually mild, and anaphylaxis is rare (8). Even more rare is methemoglobinemia, which results in impaired oxygen delivery to tissues and is most commonly seen with the use of benzocaine or prilocaine. Early signs include “chocolate cyanosis”—a brown or gray discoloration of the lips and mucous membranes. It can progress to involve dysrhythmias, seizures, myocardial infarction, coma, and death.
MONITORING DURING AWAKE LARYNGEAL PROCEDURES
Patients do experience significant changes in hemodynamic parameters during awake laryngeal procedures. In a study of 31 patients who had monitoring of their vital signs during their procedure, 23% of patients developed severe hypertension and 29% significant tachycardia (11). Furthermore, none of these patients reported or showed signs of abnormal amounts of discomfort (11). Despite the fact that others have found that the vast majority of patients tolerate procedures and report minimal pain or discomfort (12,13), these findings suggest that patients are experiencing significant hemodynamic changes that do not correlate to subjective comfort levels. Given the low complication rates of awake procedures, these changes likely do not pose a significant danger to patients. Thus, in general, it is the opinion of the authors that monitoring is not indicated in patients who do not receive sedation. However, patients with significant comorbidity such a severe cardiac or pulmonary disease may benefit from pulse oximetry and/or blood pressure monitoring.
AIRWAY EVALUATION AND ASSESSMENT
With adequate anesthesia, the airway can be examined fully in the office. It allows for evaluation of both dynamic and fixed obstruction, which cannot be done under general
anesthesia with rigid endoscopy. This can yield important information to help plan and guide any potential operative intervention, as well as to monitor operative results during follow-up. Concern of laryngospasm and lack of patient tolerance often prevent clinicians from employing these techniques. However, it is a very safe technique (9) that can provide immediate and valuable information.
anesthesia with rigid endoscopy. This can yield important information to help plan and guide any potential operative intervention, as well as to monitor operative results during follow-up. Concern of laryngospasm and lack of patient tolerance often prevent clinicians from employing these techniques. However, it is a very safe technique (9) that can provide immediate and valuable information.
Cricoarytenoid Joint Fixation and Posterior Glottic Stenosis
When a patient presents with an immobile vocal fold, one must distinguish between cricoarytenoid (CA) joint fixation and nerve paresis or paralysis if their history is suggestive of the former as a potential etiology. This determination is important to guide therapy and determine prognosis. CA joint mobility can be assessed by looking for the “jostle sign.” An immobile arytenoid due to nerve paresis or paralysis will be “jostled” by the mobile arytenoid with phonation, whereas the arytenoid of a fixed CA will not jostle. However, this can be a very subtle sign to diagnose.
CA joint mobility can be more reliably assessed via palpation, which has classically been done via direct laryngoscopy under general anesthetic. Palpation can, however, be done awake if the larynx has been adequately anesthetized (14,15). A flexible or rigid endoscope is used to visualize the larynx while the surgeon or patient holds the tongue, and a curved forceps or Abraham cannula can be used to provide gentle pressure at the vocal process of the arytenoid cartilage in a lateral and posterior direction.
Similarly, it is often important to distinguish between bilateral vocal fold immobility due to a neurologic cause and posterior glottic stenosis. A similar maneuver to that described above can be done with two instruments simultaneously to assess for CA joint mobility as well as posterior glottic stenosis (15).
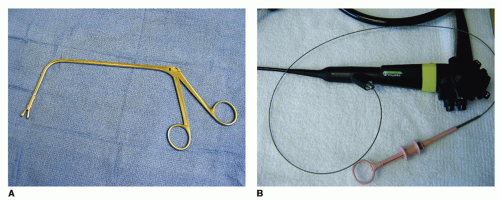 Figure 73.2 A: Curved biopsy forceps for peroral laryngeal biopsies. B: Flexible biopsy forceps passing through working channel of flexible endoscope. |
Subglottic and Tracheal Stenosis
The complete tracheobronchial tree can be evaluated with adequate topical anesthesia. With the anesthesia techniques described above, examination to the level of the carina is possible. Further examination of the bronchi usually requires application of topical anesthesia to the bronchi via the working channel of the scope. A flexible endoscope can easily be passed distal to the vocal folds with no significant risk of laryngospasm and is well tolerated by the majority of patients (9). Subglottic and tracheal stenosis, laryngeal and upper airway tumors, and tracheomalacia can be evaluated closely. The latter is easier to examine awake as opposed to under general anesthesia due to its dynamic nature. The length and degree of stenosis can be assessed, although length may be difficult or impossible to assess in severe stenoses if the scope will not pass through easily or if the patient has the sensation of airway obstruction.
LARYNGOPHARYNGEAL BIOPSY, PANENDOSCOPY, AND TUMOR STAGING
Biopsies may be done peroral with a rigid scope and a long curved biopsy forceps (Fig. 73.2A) after appropriate topical anesthesia of the larynx. The patient holds on to their tongue while the surgeon holds the scope and directs the biopsy forceps. However, this technique can be difficult to perform and is not well tolerated by all patients. The development of flexible endoscopes with working channels that pass easily through the nasal cavity has facilitated biopsies to be done in this manner. Generally, this technique is better tolerated by most patients. The scope is advanced to a position with the lesion of interest in view, and a 1.8-mm flexible cup biopsy forceps (Fig. 73.2B and C) is passed through
the working channel by an assistant until visible beyond the tip of the scope. The forceps are then opened and the scope is advanced until the forceps come into contact with the lesion (Fig. 73.2D). The forceps are then closed and removed from the scope. The scope can be left in place and multiple biopsies can be taken, which is advisable as the small size of the biopsy forceps can result in false-negative results.
the working channel by an assistant until visible beyond the tip of the scope. The forceps are then opened and the scope is advanced until the forceps come into contact with the lesion (Fig. 73.2D). The forceps are then closed and removed from the scope. The scope can be left in place and multiple biopsies can be taken, which is advisable as the small size of the biopsy forceps can result in false-negative results.
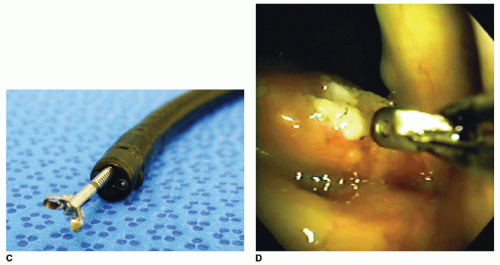 Figure 73.2 (Continued) C: Biopsy forceps tips visible beyond the end of a flexible endoscope. D: Biopsy of vocal fold lesion using a flexible 1.8-mm biopsy forceps. |
The ability to conduct biopsies, along with transnasal esophagoscopy (TNE) and awake bronchoscopy, allows for awake panendoscopy and tumor staging to be done in the office setting. This has been demonstrated to be as effective as operative staging under general anesthesia (16).
VOCAL FOLD INJECTION
Like many procedures in laryngology, vocal fold injection began as an office-based procedure but became a well-established technique under general anesthesia. Awake injections are certainly more convenient for patients and also avoid the risks of general anesthesia. This is significant for patients with significant medical comorbidity or who are recovering from a recent operation. The latter situation can pose a dilemma in patients with operative injury causing vocal fold immobility (17), and an awake injection offers a safe alternative.
The majority of awake office-based vocal fold injections are done for injection laryngoplasty. Indications for injection augmentation include vocal fold paralysis or paresis, vocal fold atrophy, scar, sulcus vocalis, and postsurgical defects. This chapter focuses on these indications. Other indications for injection include more superficial injection of steroid, cidofovir, or bevacizumab (1,18,19).
Numerous studies have shown awake injection laryngoplasty to provide excellent results in treating glottal insufficiency (17,20), even when compared to traditional injection laryngoplasty done under general anesthetic (5,21). Furthermore, there is a substantial cost savings associated with awake injection over traditional injection under general anesthetic (5).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


