Pediatric Ophthalmology
Edited by P. F. Gallin
Thieme Medical Publishers, Inc.
New York ©2000

15

Ocular Trauma
Each year an estimated 1.3 million Americans suffer eye injuries. A disproportionate share of ocular and orbital injuries occur in children.1 The population-based estimate of the incidence of ocular trauma in children is 15.2 per 100,000 per year.2 Ocular injuries in children over 10 years of age are most commonly sports related, whereas injuries in the home account for the majority of trauma in children younger than 10 years of age.3 The majority of pediatric eye injuries are preventable. Visual disability in children that is secondary to eye injuries can be greatly reduced by the implementation of well-established safety precautions and supervision.
Appropriate and timely management of eye trauma is essential to ensuring optimal outcome for the child. As many of the cases are initially managed by pediatric practitioners, the child with eye trauma should be promptly referred to an ophthalmologist. A 3-year survey conducted at the Wills Eye Hospital revealed that approximately 22% of all ocular injuries in children required hospital admissions.4 Only admissions for strabismus account for more pediatric hospitalizations than for eye injuries.
In this chapter we will discuss the standardized classification of ocular trauma and the major causes of pediatric eye trauma and its management.
 Classification of Ocular Trauma
Classification of Ocular Trauma
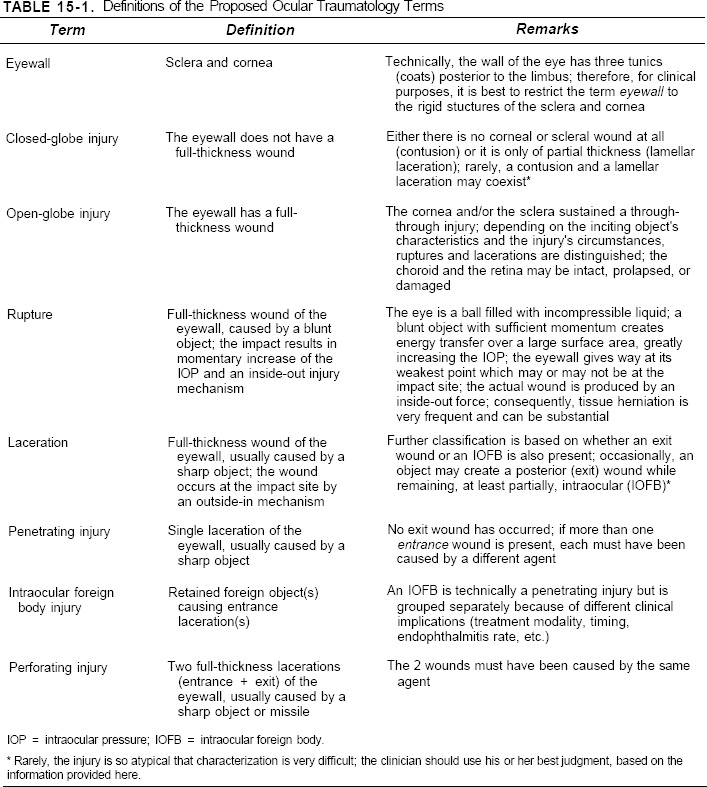
A classification of ocular trauma (Table 15-1) has been developed by Kuhn et al.5 This classification has been endorsed by the International Society of Ocular Trauma, United States Eye Injury Registry, and American Academy of Ophthalmology. At the time of initial presentation, an attempt should be made to classify the injured eye based on this classification system.
 Management of Pediatric Ocular Trauma
Management of Pediatric Ocular Trauma
The key to proper management of pediatric ocular trauma is a systematic approach including a thorough history and a methodical examination. Unfortunately, this evaluation may be hampered by inadequate instrumentation, an uncooperative patient, or fear of causing further damage to the eye.
The time of examination should be documented. An external exam should be performed first to look for eyelid lacerations. Visual function should be estimated (best corrected visual acuity, color vision, confrontation visual field, presence of relative afferent pupillary defect), followed by a slit lamp biomicroscopic exam to evaluate for signs of conjunctival tears, corneal fluorescein stain, depth of anterior chamber, anterior chamber activity, hyphema, iridodialysis, iridodonesis, and phacodonesis.
A dilated fundus exam also should be performed. Retinal pathology should be carefully drawn. The initial exam may well be the only opportunity to visualize the retina. If there is a vitreous hemorrhage, the retinal view may be lost during subsequent exams.
Ultrasound biomicroscopy should be performed carefully without applying undue manipulation of and pressure on the globe. It is a safe and effective adjunctive tool for the clinical assessment and management of ocular trauma, especially when visualization is limited and multiple traumatic injuries are involved. Eyes with angle recession, iridodialysis, cyclodialysis, hyphema, intraocular foreign body, scleral laceration, and subluxed crystalline lens have been imaged without complication. Ultrasound biomicroscopy aids in the diagnosis when visualization is limited by media opacities or distorted anterior segment anatomy.
Plain radiographs of the orbit help to localize metallic foreign bodies. Caldwell view, Water’s view, and lateral views should be requested to identify orbital foreign bodies and orbital bony fractures.
Computed tomography scans are extremely helpful in identifying retrobulbar hemorrhage, differentiating between intraocular and orbital foreign bodies, and identifying orbital bony fractures and extraocular muscle entrapment.
Intravenous antibiotics and tetanus toxoid injection should be administered when open globe injury is suspected. Treatment of corneal abrasions, hyphema, traumatic optic neuropathy, and other sequelae of closed globe injuries is according to the standard of care.
Surgical Intervention and Exploration under General Anesthesia
If an open globe injury is suspected, only minimal ocular examination and manipulations should be performed. After radiological investigations to rule out an intraocular foreign body, surgical intervention should be urgently performed under general anesthesia to repair or explore the globe. The threshold for exploration should be low whenever a penetrating or perforating injury or rupture of the globe is suspected. In addition, the globe should be explored under general anesthesia if an examination is not possible because the child is combative.
Examination under anesthesia often allows for careful indirect ophthalmoscopy if no intraocular hemorrhage is present. If the view of the fundus is unobscured, a subsequent surgical exploration may not be necessary. On the other hand, the optic disc and the macula can be carefully assessed for prognostication and medical/legal sequelae.
An adequate view of the fundus might not be possible due to corneal laceration, hyphema, cataract, or vitreous hemorrhage. If a laceration of the cornea is present this should be closed, approximating the limbus first. The conjunctiva should be incised to expose the course of the laceration. As the laceration is seen, it should be closed step by step. The laceration should be closed anteriorly prior to further posterior exploration to prevent extrusion of intraocular tissues.
Lacerations can be found anywhere on the globe. Ruptures are often at the limbus and at the muscle insertions. If the penetrating injury crosses the muscle insertion, the vitreous base may be involved. The suture material is then changed to absorbable suture material to allow for placement of a scleral buckle. The wound at, and posterior to, the muscle insertion is closed and placed on a radial or circumferential buckle.
If vitreous hemorrhage is present, a foreign body may be present. The foreign body is removed using an external or internal magnet according to the principles of foreign body vitreous surgery. If vitreous hemorrhage is present without a foreign body, it should be observed for infection and clearing. Ultrasound is used to monitor the eye. If vitreous hemorrhage does not clear, and amblyopia is a concern, vitreous surgery is undertaken to clear and remove the blood and reattach the retina as indicated.
 Major Causes of Pediatric Ocular Trauma
Major Causes of Pediatric Ocular Trauma
Child Abuse (See also Chapter 7, Child Maltreatment.)
There are an estimated 2 million victims of child abuse in the United States per year. Physical abuse is the leading cause of serious head injury in infants. Although physical abuse has in the past been a diagnosis of exclusion, data regarding the nature and frequency of head trauma consistently support a medical presumption of child abuse when a child younger than 1 year of age has intracranial injury.6 Any physician who suspects child abuse is required by U.S. law to report the incident to a designated governmental agency for appropriate investigation.
The presenting sign of child abuse involves the eye in 5% of cases. Forty percent of physically abused children will present with ocular and periocular findings. Blunt trauma inflicted with fingers, fist, belts, or straps is the usual mechanism of injury. Typical anterior segment findings include periorbital ecchymosis, subconjunctival hemorrhage, hyphema, and subluxated lenses. Posterior segment findings include retinal hemorrhages, retinal tears, and rhegmatogenous retinal detachments. The optic nerve can show papilledema or atrophy (see Chapter 21).
Certain diagnostic findings are also highly suggestive of child abuse such as the pattern of two or three parallel bruises on the face as in a slap, the paired semicircular bruises of the human bite, or bruises on the thorax or upper arm.16 Furthermore, some general findings that lead to suspicion include several sites of soft tissue or bony injuries that are in different stages of healing, when multiple hospital admissions to different hospitals are reported in the history, when the guardian’s report regarding the injury does not match the extent or location of findings, or when the reported events are inconsistent with the child’s likely behavior at that age.
Conceptually, alcohol and drug abuse during pregnancy may be considered a form of “child abuse” as the effects last through childhood and beyond. The ophthalmic findings of fetal-alcohol syndrome have been well described and include craniofacial abnormalities, lid shortening, cataract, increased tortuosity of the retinal vessels, optic nerve hypoplasia, and learning disabilities.7 Although clinical and experimental evidence of retinal vascular abnormalities with retinal hemorrhages has been reported from maternal use of cocaine,8 not all studies have confirmed the clinical significance of this abuse.9 More work in this area is needed to fully elucidate the relationship between drug abuse and congenital ocular disease.
Accidental Injury
There are reports of association of ocular injury with infant walker use.10 Penetrating ocular injury has been reported after a minor fall with some designs of rigid infant pacifiers.11 Corneal abrasion secondary to accidental trauma should be considered in an inconsolably crying otherwise asymptomatic infant.12
Accidental Blows and Falls
The most common cause of pediatric ocular trauma is accidental blows and falls.2 Injuries include orbital contusions and hematomas, facial hypesthesia, eyelid lacerations, subconjunctival hemorrhages, corneal edema and abrasion, hyphemas, traumatic iritis, iris sphincter ruptures, iris atrophy, angle recession, iridodialyses, traumatic cataract, vitreous hemorrhages, retinal hemorrhages, macular hole formation, optic atrophy, and bony orbital wall fractures.
Bungee cords,13 merchandise display hooks,14 and water balloon slingshots15 have also been associated with accidental ocular trauma.
In accidental trauma the most frequent sites of injury include the forehead, anterior tibia, and other bony protuberances such as the chin. Injury to the face, trunk, buttocks, and genital area may suggest deliberate or malicious injury.
Sports and Recreational Activities
Sports trauma is a leading cause of permanent vision loss in the United States irrespective of age. The type of sport and the mechanism most frequently responsible for injuries are, respectively, outdoor and indoor soccer and ball trauma.17 Basketball, baseball, and the racquet sports are other leading causes of ocular trauma.18 Common injuries include corneal abrasion, traumatic iritis, lid or orbital contusions, and conjunctival hemorrhages. The great majority of injuries could have been prevented if adequate protective eyewear had been worn. Eye care practitioners should advocate the use of protective eyewear for patients who participate in sports activities (see position paper by American Academy of Ophthalmology and Pediatrics).
Bungee jumping is a recreational sport that has gained worldwide popularity. The injuries and deaths that have occurred have made safety an integral issue in the practice of the sport. Although early reports of significant injuries are infrequent, more recent investigations have indicated severe sequelae, including ocular hemorrhage.19
Pets
Tarantulas have become increasingly popular pets.20 Typically, owners are unaware of the potential risk of ocular injury from the barbed urticating hairs found on the dorsal aspect of a tarantula’s abdomen. Patients who manifest red eye and pain after handling a tarantula should be examined to determine if offending barbed hairs are present in the cornea and conjunctiva.
Automobile Accidents
The effectiveness of air bags as a safety device in decreasing fatalities and reducing morbidity in frontal impact motor vehicle accidents has been well established. However, ocular injuries can occur due to air bag inflation, particularly when seatbelts are not worn properly.21 Hyphema and corneal abrasions are the most common injuries related to air bag inflation. Several serious cases of vision-threatening injuries, including retinal detachment, retinal dialysis, scleral rupture, and dislocated lens, have also been reported. Eyeglass wear presents an additional risk factor for serious and permanent ocular damage.
Thermal and Chemical Burns
Eye injuries caused by fireworks are often severe and can cause permanently reduced visual acuity or blindness. Approximately 12,000 persons are treated each year in U.S. emergency departments because of fireworks-related injuries; of these, an estimated 20% are eye injuries.22 In one study 95% of children treated for injuries associated with fireworks were reported to be injured during the 3-week period of June 22 to July 14.23 Firecrackers are associated with the majority of injuries, followed by bottle rockets, Roman candles, sparklers, fountains, and jumping jacks. Permanent sequelae are more common for eye injuries caused by rockets than eye injuries caused by other types of fireworks. Children and their families should be encouraged to enjoy fireworks at public fireworks displays conducted by professionals.
The most common type of thermal burn to the ocular surface in children is due to contact with the tip of a cigarette. This type of injury typically occurs in children 2 to 4 years of age. It should be noted that these injuries occur frequently. At this age, toddlers frequently run into cigarettes inadvertendy held by an adult at the child’s eye level. When the cigarette burn is accidental, the corneal abrasion is usually in conjunction with a lid burn as well; the child’s lids began to close from the blink reflex. When the injury is purposeful and is child abuse, the lids have been forcibly held open and there is a discrete corneal burn only.
Chemical burns in children are often due to household products kept on low shelves. These include various organic solvents, soaps, drain cleaners, and household cleaning agents. They are some of the strongest acidic and alkaline substances known to cause ocular injury.
A high index of suspicion is in order when a child presents for evaluation of a red eye with a corneal or conjunctival abrasion. Very often in the pediatric age group, the traumatic event is not witnessed, and the parent may not be aware of the fact that the eye has been exposed to a caustic agent. A piece of pH paper briefly inserted into the inferior conjunctival fornix may provide an indication of the acidic or alkaline nature of the offending agent and serve to help guide further management. As in adults, acid burns may initially cause severe damage upon contact; however this is usually self-limited due to the rapid production of a coagulum that limits further damage. Alternatively, alkali burns may reveal a less impressive initial presentation. However, due to the fact that alkaline substances result in the saponification of fatty acids in the cornea, alkali burns may actually “melt” the cornea and gain access to the internal structures of the eye with disastrous consequences. When it comes to management, copious irrigation is the rule, irrespective of the nature of the offending agent. This often involves several liters of normal saline and should be continued for at least 30 minutes. The pH should then be checked again to ensure neutrality. Irrigation should be followed by the meticulous removal of any particulate matter with specific attention paid to the upper and lower conjunctival fornices. Particulate matter often contains small amounts of the culpable agent in addition to necrotic debris. Limbal vasculature blanching, also known as marblization, is a warning sign of ocular ischemia, and therefore its presence is a poor prognostic indicator.
Although almost all chemical injuries will reveal significant loss of corneal and conjunctival epithelium, if the limbal stem cell population has not been damaged, these injuries typically heal well with a topical antibiotic, cycloplegic, and lubricant. In the setting of an alkaline burn, a topical steroid may be added during the initial portion of therapy. For burns of the ocular surface recalcitrant to conventional therapeutic modalities, newer therapies have yielded promising results, such as limbal autograft transplantation. In this procedure, portions of the limbus and adjacent conjunctival tissue are harvested from the healthy fellow eye and transplanted to the injured eye, thus repopulating the injured eye with the limbal stem cells needed for wound repair. Results of this technique have been encouraging.
Overall, children should be re-evaluated frequently to confirm compliance with the prescribed regimen, an often difficult prospect for both the child and the parent. Furthermore, frequent re-examination is necessary to monitor for failure to heal. It should be noted that, in addition to observing the cornea and conjunctiva for healing, specific attention should be paid to the conjunctival fornices, often the site of insidiously developing symblepharon.
Self-Mutilation
Self-inflicted injury to the eyes is an extremely uncommon form of behavior. Intentional, severe, self-inflicted eye injuries may be seen in patients with organic disabilities, either autism, dementia, or severe mental retardation, where a lack of impulse control and preexisting eye irritation or surgical operation may contribute to the act.24 Severe ocular injuries due to self-mutilation include retinal detachment resulting in visual loss and self-enucleation.25 Active vigilance from caretakers and psychiatrists is essential as the majority of the patients are confined at the time of the act. Trichitellemania is an entity whereby children, usually adolescents, pull out their lashes continually until none remain. This is treated with counseling and antidepressive agents; however, it is quite difficult to cure.
 Types of Ocular Trauma
Types of Ocular Trauma
Birth Trauma
Trauma secondary to childbirth is usually due to traumatic vaginal delivery or application of obstetric forceps. The frequency of sight threatening complications in instrumental deliveries is, however, low. The injuries are generally superficial, and include periorbital ecchymosis and lid edema, conjunctival chemosis, subconjunctival hemorrhage, corneal abrasion or corneal edema, and obliquely oriented Descemet’s tears.
Scrolls of Descemet’s membrane are usually present at each margin of the break. Obstetric forceps pressure strong enough to cause corneal injury usually leaves an occipital depression from the opposite forceps blade26 (Fig. 15-1).
Posterior segment findings are usually limited to flame-shaped retinal hemorrhages. The anatomic location and appearance of retinal hemorrhages in infants provide important clues in the diagnosis of underlying disorders. Although neonatal retinal hemorrhages related to birth trauma are common, benign, and self-limited, retinal hemorrhages may also be caused by a variety of ocular (e.g., PHPV, ROP) or systemic diseases (e.g., hematological or cardiovascular disorders and infections).27 Prompt diagnosis of retinal hemorrhages in infants is crucial because treatment may be required to prevent amblyopia and blindness. Birth weight is likewise a factor as fetal macrosomia has been associated with increased risk of birth trauma in vaginal deliveries.28 However, low birth weight is also a factor predisposing to some types of injuries. Hypoxia, coagulation dysfunction, and neonatal vascular fragility are mentioned as mechanisms in these instances.29
Orbital Fracture
Blunt impact in the region of the eye may produce orbital bone fractures. Fractures of the orbital floor or “blowout fractures are common in children when objects larger than the orbital rim strike the eye. In children, these commonly include projectile injuries such as those due to balls and rocks. Examination often reveals limitation of ocular motility frequently associated with restriction of ocular motility on attempted upgaze, although downgaze may be affected as well. These restrictions may be manifest only as diplopia on extreme upgaze or downgaze. Restrictions in other fields of muscular action may occur as well. Other signs of orbital floor fracture include orbital emphysema, subconjunctival emphysema, epistaxis, and hypesthesia of the ipsilateral cheek and upper lip. Management considerations of orbital floor fractures are similar to those for adults and are beyond the scope of this text.

FIGURE 15-1. (A) Neonate with evidence of forceps-related birth trauma on forehead and eyelid of left eye. (B) Same child with corneal edema secondary to rupture of Descemet’s membrane.
Fracture of the medial wall of the orbit may occur via the same forces that produce orbital floor fracture and the two are often seen simultaneously. Signs of medial wall fracture include orbital emphysema, epistaxis, and enophthalmos. Medial canthal tendon injury may be associated with a medial wall fracture and often results in an increased intercanthal tendon distance. Furthermore, the nasolacrimal drainage apparatus may be damaged, resulting in a variety of complications including epiphora.
Although rare in adults, isolated fracture of the orbital roof is the most common type of fracture of the orbit encountered in early childhood.30 It is thought that differences in early anatomy may help to explain this discrepancy. In adults, the relatively thicker superior orbital rim and the fully developed frontal sinus might limit deflection of the orbital roof and prevent fracture. However, in young children, the superior orbital rim is considerably less well developed, and the lack of frontalsinus pneumatization potentially allows for momentary deflections of the orbital roof large enough to rupture adjacent blood vessels and fracture bone.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


