Ocular Protection from Solar Radiation
Jonathan C. Javitt
Hugh R. Taylor
Each of us is exposed to some amount of sunlight. The extent of exposure can vary greatly depending on a person’s occupation and recreational activities. As a visual organ, the eye is very much affected by light. Visual pigments in photoreceptor outer segments are constantly bleached, shed, and rapidly regenerated. With ordinary exposure, these light-induced changes. are short-lived and rapidly reversed. However, intense exposure to either the broad band of visible light or to narrower specific bands in the visible spectrum, such as those produced by a laser, can cause permanent ocular damage. For example, the occurrence of retinal burns in eclipse blindness is well known,1 and initial experiments in retinal photocoagulation were performed with highly focused solar energy.2
Not all bands of electromagnetic radiation emanating from the sun are in the visible spectrum, and many of the nonvisible bands can have a serious impact on biologic function. Although most harmful solar radiation is filtered out by the atmosphere, the sunlight that does reach the earth’s surface contains sufficient amounts of ultraviolet radiation (UVR) to cause sunburn3 and various skin cancers.4,5 The changing life-style of persons in developed countries is causing a rapid increase in exposure to sunlight and consequently to UVR. The dermatologic and epidemiologic literature, as well as the lay press, documents a sudden rise in the rate of skin cancers.5 Just as topical sun-blocking agents are prudent measures in protecting the skin from harmful solar radiation, simple practical measures such as wearing appropriate spectacles or a hat can effectively protect the eyes from exposure to UVR type B (UV-B).
DESCRIPTION OF ULTRAVIOLET RADIATION
PHYSICAL DEFINITION OF UVR
The spectrum of nonionizing radiation ranges from short-wavelength UVR (wavelength 100 nm) to far-infrared radiation (1 mm or 100,000 nm) (Fig. 1). The visible spectrum lies between 400 nm (indigo) to 760 nm (red). Beyond the visible spectrum is infrared radiation, and below the visible spectrum are the shorter wavelengths of nonionizing radiation called ultraviolet radiation (UVR). Although UVR is only 5% of the sun’s energy, it is the most hazardous portion encountered by humans. The physical spectrum of UVR ranges from 100 to 400 nm. However, much of the nonionizing radiation is absorbed by the earth’s atmosphere. Wavelengths less than 290 nm are totally absorbed by the ozone layer in the stratosphere, and longer wavelengths are absorbed to a lesser extent. Thus, in nature, UVR less than 290 nm does not reach the earth’s surface and is not encountered.6
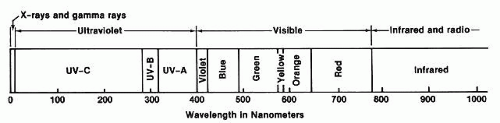 Fig. 1. The spectrum of ultraviolet and visible light. |
Based on the biologic effects of the different wavelengths or bands, UVR has been subdivided into three bands: UV-A (400 to 320 nm), UV-B (320 to 290 nm), and UV-C (290 to 100 nm).7 UV-A, or near UVR, produces tanning (the browning of the skin due to an increase in the skin content of melanin) and photosensitivity reactions. UV-A is emitted by so-called black lights, which are often used to make objects fluoresce and are also used in tanning salons. UV-B causes sunburn (painful erythema and blistering), and increased exposure to UV-B is associated with an increased rate of skin cancer.6,7,8,9 UV-C, which is germicidal and may also cause skin cancer, is not normally encountered on the earth’s surface and comes entirely from artificial sources such as germicidal ultraviolet lamps or arc welding.
ENVIRONMENTAL, TEMPORAL, AND GEOGRAPHIC VARIATIONS IN ULTRAVIOLET RADIATION
UVR is scattered across the whole sky by the Rayleigh effect, just as blue light is scattered.8 Light or broken clouds do not significantly reduce the level of UVR, although levels are reduced by heavy cloud cover.8 A sky with a clear horizon for 360° provides for maximal exposure; when hills, trees, or buildings obstruct part or all of the horizon, the UVR exposure is reduced proportionally.10 UVR can also be reflected by the ground, the amount dependent greatly on the type of surface (Fig. 2). Grass and soil reflect only 1% to 5% of UV-B, water 3% to 13%, sand and concrete about 7% to 18%, and fresh snow up to 88%.10
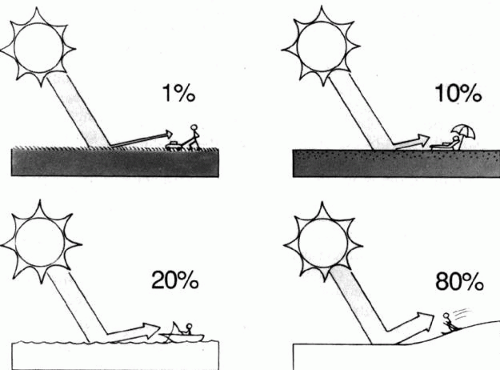 Fig. 2. There is substantial variation in the amount of UVR reflected by different surfaces. The extremely high reflectivity of snow and ice accounts for the risk of snow blindness (photokeratitis) encountered during spring skiing at high altitudes. (Javitt JC, Taylor HR: Focal Points: Clinical Modules for Ophthalmologists 9(3). Reprinted with permission from the American Academy of Ophthalmology, 1991) |
As the sun makes its daily transit, the spectral content of sunlight changes substantially (Fig. 3). At low incident angles, nearly all visible and ultraviolet energy is reflected or absorbed by the atmosphere, giving the familiar reddish hue to early morning and late evening sunlight. The UV-A and UV-B content of sunlight increases as the sun reaches its zenith and progressively decreases during the afternoon. Similarly, the farther from the equator, the more oblique is the angle of sunlight incidence and the lower the UVR level on the ground. Many people have learned the hard way that an hour’s exposure to tropical sunlight imparts a far greater dose of UV-B than does an hour on the beach in New England or the Pacific Northwest. As the Earth tilts to produce changing seasons, so too does the angle of sunlight incidence and the resulting UVR content of sunlight, with summer sunlight imparting far greater doses of UV-B than sunlight of other seasons.
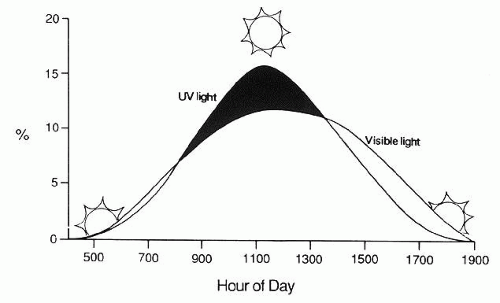 Fig. 3. Percent of total energy by hour of day. The relative UVR content of sunlight varies during the day and reaches its peak at noon. (Javitt JC, Taylor HR: Focal Points: Clinical Modules for Ophthalmologists 9(3). Reprinted with permission from the American Academy of Ophthalmology, 1991) |
The ambient dose of UVR also increases somewhat at higher altitudes, because there is less atmosphere to filter the sun’s energy. UV-B exposure increases approximately 20% per 10,000 feet. Climbers have frequently discovered that they are vulnerable to sunburn even when the sun seems to exert little warming effect. Persons climbing and skiing on snow-covered peaks are at particular risk because of the extremely high ultraviolet reflectivity of snow and ice.
The eyes are normally protected and shielded from UVR by a number of factors11,12a and only receive a small fraction of ambient UV-B under normal circumstances. The normal horizontal alignment of the eyes and the orbits significantly reduces ocular exposure to whole-sky irradiation. Further anatomical protection is provided by the brows, the nose, and the cheeks.13 The eyelids provide protection that is further enhanced by squinting, a common reflex in bright sunlight. The eyes are relatively unprotected laterally, although the transmission of UVR by internal reflection in the cornea may lead to a concentration of ultraviolet irradiation at the nasal limbus.14 Other personal factors that can decrease ocular UVR exposure in a given environment include wearing a hat and protective eyeglasses.11,12 Taken together, these different factors result in an ocular exposure that is between 7% and 17% less than the ambient UVR level.12
OCULAR TRANSMISSION OF ULTRAVIOLET RADIATION
Only a fraction of the UVR entering the eyes reaches the retina-a fact with important photobiologic implications (Fig. 4). The amount of radiation that is absorbed determines the potential for damage to the absorbing tissue. Energy from the dissipation of the absorbed radiation results in tissue damage. Radiation that is not absorbed by a superficial tissue will be transmitted and can affect deeper tissues.
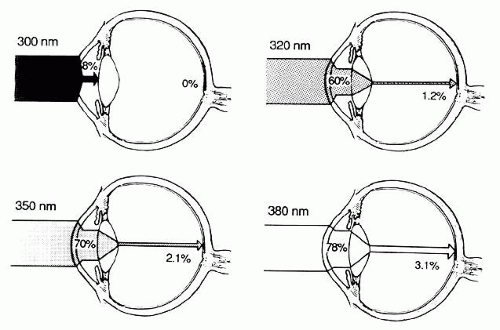 Fig. 4. Absorption of light by ocular structures varies with its wavelength. (Javitt JC, Taylor HR: Focal Points: Clinical Modules for Ophthalmologists 9(3). Reprinted with permission from the American Academy of Ophthalmology, 1991) |
The cornea absorbs almost 100% of UV-C radiation (below 290 nm), but transmission rapidly increases for longer wavelengths, so that, for instance, 60% of radiation at 320 nm is transmitted by the cornea.15,16,17,18 A normal young human lens absorbs most UVR below 370 nm. As the human lens yellows with age, it absorbs even more UV-A and also shorter blue wavelengths.18,19 In adults, less than 1% of radiation between 320 and 340 nm and only 2% of radiation of 360 nm reaches the retina.20 The lens is exposed to and absorbs most of the UV-B entering the eye.
MECHANISMS OF PHOTOTOXICITY
The energy carried by a photon is directly proportional to its frequency; thus, the shorter the wavelength, the higher the energy. A photon’s energy is absorbed by the atom or molecule with which it collides. Low-energy infrared photons carry enough energy to affect the rotational or vibrational state of an atom or a molecule and produce warming. Higher-energy UVR photons can alter the energy state of the electrons, making the atom or molecule relatively unstable, leading to oxidative reactions including cross-linking and denaturation of proteins and free-radical formation. Higher-energy photons such as gamma rays cause an electron to be removed entirely from the molecule, thereby causing ionization.
The capacity of a given atom or molecule to absorb radiant energy is dependent on its physicochemical properties, and the characteristics of a tissue are in turn dependent on the properties of its constituents. The lens proteins are rich in the amino acid residues of tryptophan, tyrosine, and phenylalanine, which absorb most of the radiant energy below 300 nm. Cross-linking of these proteins is implicated in the pathogenesis of cataract. Other chromophores and pigments in the lens appear to absorb most of the energy in the 300 to 400 nm range.21
EFFECT OF ULTRAVIOLET RADIATION ON OCULAR TISSUES
CORNEA
Photokeratitis from Acute Exposure
Exposure to UV-B and UV-C may cause a superficial punctate keratopathy that appears up to 6 hours after exposure. This is the ocular analogue of acute blistering sunburn. The condition is most frequently encountered as “welder’s flash,” caused by even momentary exposure to UV-C during arc welding. Clusters of photokeratitis have been reported in association with defective glass envelopes surrounding mercury vapor lamps, most frequently in school gymnasiums. Naturally occurring UV-B in sufficient doses also causes photokeratitis. This condition, often termed snow blindness, is usually encountered when the UVR reflectivity of the environment is extremely high, such as during spring skiing. Snow blindness is of historical interest and importance in the annals of arctic and Antarctic explorers. Like welder’s flash, snow blindness is a self-healing epithelial injury that resolves in 8 to 12 hours. Photokeratitis can occur in more hospitable environments as well. Near-threshold exposures of UV-B can be received during the summer on beaches in the southern United States.
The corneal epithelium can tolerate only a certain dose of UV-B before breakdown occurs. Although this threshold may be nearly reached during a full day of winter skiing, skiers may notice only irritation during the evening, and epithelial repair will occur during sleep. With the increased UV-B content in spring sunlight, this threshold can be exceeded in 1.5 to 2 hours of noontime skiing, especially at higher altitudes. Thus, by evening, spring skiers may have painful photokeratitis and a matching sunburn.
Photokeratitis accounts for 59% of all injuries associated with tanning booths.22 It can occur if the protective goggles are defective or removed even briefly or if the glass envelope of the lamp is defective and allows UV-C to escape.
Pinguecula and Pterygium from Chronic Exposure
Pingueculae are localized yellowish-gray fleshy lesions that appear close to the limbus on the nasal or temporal interpalpebral bulbar conjunctiva. Pterygia are somewhat similar in appearance but involve the peripheral cornea as well. Histologically, both lesions contain deposits of degenerating collagen fibers, elastoid fibers, and an increased population of metabolically active stromal fibrocytes. Similar histologic changes are found in the dermis of sun-exposed skin.
Pterygium occurs more commonly in tropical or sunny areas than in more temperate regions and has been clearly associated with exposure to UVR.23,24 Although geographic and ecological differences in pterygium rates have been postulated to result from non-UVR factors, such as corneal drying or microtrauma caused by smoke, sand, and dust particles, studies have confirmed the importance of UVR exposure.
A study of 838 men who work on Chesapeake Bay showed that the risk of pinguecula and pterygium was significantly associated with increased levels of UV-A and UV-B.25 For those in the highest quartile of annual UV-B or UV-A exposure, the odds ratio for the development of pterygium was 3.06.
Climatic Droplet Keratopathy
Climatic droplet keratopathy (CDK), which has also been called Labrador keratopathy, chronic actinic keratopathy, proteinaceous degeneration, and keratinoid degeneration, is a spheroidal degeneration of the superficial corneal stroma. The condition is characterized by yellow, oily-appearing subepithelial droplets replacing Bowman’s layer or lying in the superficial stroma. In general, their distribution is similar to that of band keratopathy, but with a clear zone of separation from the limbus and corneal vessels. The changes are thought to be caused by degeneration of serum proteins that normally diffuse through the cornea.
In the study of Chesapeake Bay watermen, CDK was even more strongly associated with UV-B exposure than was pterygium.25 The odds ratio for average annual UV-B exposure in the upper quartile was 6.36 for CDK, as compared with the lower quartile. Similar ratios were shown for exposure to UV-A.
ASSOCIATION BETWEEN ULTRAVIOLET RADIATION AND CATARACT
Experimental Basis for an Association Between UVR and Cataract
A number of experiments have shown that UVR exposure causes cataracts in animals, particularly cortical and posterior subcapsular Cataracts. Both guinea pigs and rabbits acutely exposed to UVR (293 to 303 nm) develop clouding of the anterior cortex.26 Subcapsular and punctate conical opacities develop in albino mice chronically exposed to broadband UVR from 40-watt blacklight lamps (300 to 400 nm).26 Posterior migration of undifferentiated lens epithelium (posterior subcapsular cataract) in response to UVR has also been noted.27,28
The Epidemiologic Basis for an Association Between UVR and Cataract
Epidemiologic and clinical observations also suggest a link between sunlight exposure and cataract formation. Cataracts occur more commonly in tropical areas with higher sunlight exposures than in more temperate regions.29,30,31,32 People undergoing cataract surgery are more likely to have brunescent cataracts if they live closer to the equator or work outdoors.33 People in the United States who live more than half their lives in areas with high sunlight or UVR levels have a greater risk of cortical cataract.34,35,36 This association does not hold for nuclear cataract.36
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


