Chapter 16 Ocular manifestations of HIV/AIDS in children
HIV/AIDS-related illnesses are among the leading causes of morbidity and mortality worldwide.1 Each day, over 7000 persons become infected with HIV and 5000 persons die from complications related to their infection. Roughly 2.5 million children 15 years of age or less currently have HIV/AIDS. This number increased by approximately 370 000 in 2009, representing over 1000 newly infected children per day. Ocular complications occur in 70% or more of adults and up to 50% of children with HIV/AIDS if not treated with antiretroviral therapy.1,2
The introduction of multidrug combination therapy changed the face of HIV/AIDS-related eye disease. Termed Highly Active AntiRetroviral Therapy (HAART), this regimen uses a combination of potent antiretrovirals to inhibit replication of HIV. Patients on HAART experience a dramatic improvement in helper CD4+ T cell populations and a marked decline in viral titers, resulting in fewer opportunistic infections, reduced morbidity and mortality, and improved quality of life. Despite the decline in the incidence of ocular complications in patients taking HAART, they continue to occur and remain an important cause of disability in HIV-infected patients. This is particularly true in the developing world, where access to HAART varies considerably from country to country.2
HIV/AIDS: global and regional epidemiology
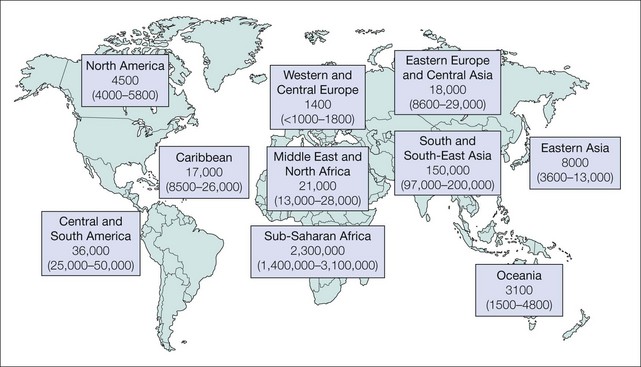
The 2010 report from The Joint United Nations Program on HIV/AIDS (UNAIDS) and the World Health Organization (WHO) on the global HIV/AIDS epidemic estimated that 33.3 million (31.4–35.3 million) people were living with HIV in 2009, 90% of whom were unaware of their infection. Roughly 15.9 million (14.8–17.2 million) were women and 2.5 million (1.6–3.4 million) were children under 15 years of age (Table 16.1). The prevalence of HIV infection in children varies, with over 90% of all children with HIV/AIDS living in Africa (Fig. 16.1). It has been estimated that 16.6 million (14.4–18.8 million) children under the age of 18 have lost one or both parents to HIV/AIDS, and of the 1.8 million (1.6–2.1 million) people who died of HIV/AIDS-related illnesses in 2009, 260 000 (150 000–360 000) were children under 15 years of age.1
Table 16.1 Global summary of HIV/AIDS as of 2009
| Number of people living with HIV/AIDS in 2009 | |
| Total | 33.3 million (31.4−35.3 million) |
| Adults | 30.8 million (29.2−32.6 million) |
| Women | 15.9 million (14.8−17.2 million) |
| Children under 15 years of age | 2.5 million (1.6−3.4 million) |
| Number of people newly infected with HIV in 2009 | |
| Total | 2.6 million (2.3−2.8 million) |
| Adults | 2.2 million (2.0−2.4 million) |
| Children under 15 years of age | 370 000 (230 000−510 000) |
| Number of HIV/AIDS-related deaths in 2009 | |
| Total | 1.8 million (1.6−2.1 million) |
| Adults | 1.6 million (1.4−1.8 million) |
| Children under 15 years of age | 260 000 (150 000−360 000) |
The numbers in parentheses represent confidence intervals based on the best available information.
From UNAIDS, Report on the global AIDS epidemic, 2010. http://www.unaids.org/globalreport/Global_report.htm.
Transmission of HIV in children
While high-risk behaviors such as injection drug use, unprotected commercial sex, and unprotected sex between men contributes to HIV transmission, most HIV infections in adults occur during unprotected heterosexual intercourse.2 Most HIV-positive children acquired their infection in utero, at delivery, or while breast feeding – so-called Mother To Child Transmission (MTCT). Prior to the advent of obstetric and antiretroviral interventions, up to 40% of infants born to infected mothers contracted HIV infection. This included 20% to 25% of infections that occurred in utero, 35% to 50% that occurred during delivery, and 25% to 35% who were HIV negative at birth, and within the first 6 weeks of delivery, but who became infected later, presumably as a result of transmission through breast milk.3 These rates have since declined dramatically in North America, Western Europe, and other resource-rich regions, where current total perinatal transmission rates vary from 1% to 3%. The incidence of MTCT in many resource-poor regions remains high due to the high prevalence of HIV in women of child-bearing age, a lack of access to antiretroviral prophylaxis, and few feasible alternatives to breastfeeding. Sub-Saharan Africa has the highest burden of HIV disease overall, accounting for 80% to 90% of perinatal infections and children infected by HIV.1
Diagnosis of HIV/AIDS in children
The Centers for Disease Control and Prevention (CDC) case definition4 of HIV infection among children aged less than 18 months recognizes four categories:
The presence of maternal antibodies can make diagnostic laboratory testing for HIV infection among children aged less than 18 months unreliable; these children with perinatal HIV exposure who develop an AIDS-defining illness (Box 16.1) are considered presumptively HIV-infected.
Box 16.1
AIDS-defining conditions for children less than 13 years of age, adolescents, and adults
• Bacterial infections, multiple or recurrenta
• Candidiasis of bronchi, trachea, or lungs
• Coccidioidomycosis, disseminated or extrapulmonary
• Cryptococcosis, extrapulmonary
• Cryptosporidiosis, chronic intestinal (greater than 1 month’s duration)
• Cytomegalovirus disease (other than liver, spleen, or nodes), onset at age >1 month
• Cytomegalovirus retinitis (with loss of vision)b
• Herpes simplex: chronic ulcers (greater than 1 month’s duration) or bronchitis, pneumonitis, or esophagitis (onset at age greater than 1 month)
• Histoplasmosis, disseminated or extrapulmonary
• Isosporiasis, chronic intestinal (greater than 1 month’s duration)
• Lymphoid interstitial pneumonia or pulmonary lymphoid hyperplasia complexa,b
• Lymphoma, Burkitt’s (or equivalent term)
• Lymphoma, immunoblastic (or equivalent term)
• Mycobacterium avium complex or Mycobacterium kansasii, disseminated or extrapulmonaryb
• Mycobacterium tuberculosis of any site, pulmonary,b,c disseminated,b or extrapulmonaryb
• Mycobacterium, other species or unidentified species, disseminatedb or extrapulmonaryb
• Pneumocystis jirovecii pneumoniab
• Progressive multifocal leukoencephalopathy
• Salmonella septicemia, recurrent
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


