Ocular Infections Associated with Human Immunodeficiency Virus Disease
Peter J. Kappel
Gary N. Holland
The most severe manifestations of HIV infection, collectively termed the acquired immunodeficiency syndrome (AIDS), were first recognized in 1981; a description of its ophthalmic manifestations followed shortly thereafter.1 Since that time, HIV infection has become a major cause of morbidity and mortality throughout the world and its associated ophthalmic infections a subject of intense study.2,3,4,5
According to the United Nations AIDS/World Health Organization, there were an estimated 39.5 million people worldwide with AIDS in 2006. The majority of these individuals live in developing countries. For updated epidemiologic data regarding AIDS, refer to the Joint United Nations Programme on HIV/AIDS Web site (www.unaids.org).
The development of secondary, opportunistic infections is a hallmark of AIDS, and the eye is a frequent site of involvement, often as the first clinically apparent site of disease. Cytomegalovirus (CMV) retinitis is the most common of the severe ocular infections to occur in HIV-infected individuals, but CMV is only one of many agents that have been reported to infect ocular tissues in the setting of HIV disease. Infections can involve the cornea, ocular surface, and adnexa; the anterior segment; or the retina, choroid, and optic nerve. This chapter reviews general concepts about opportunistic infections of the eye in HIV-infected hosts and highlights information about selected agents that are either commonly seen in people with AIDS or about which we have gained a new understanding because of the AIDS epidemic. Knowledge of the clinical characteristics, course, and disease mechanisms associated with the diseases they cause helps to manage them more effectively.
Human Immunodeficiency Virus
HIV is an RNA retrovirus, containing the enzyme reverse transcriptase, which is used to make a DNA copy of its viral RNA. The DNA copy is then incorporated permanently into the host cell genetic material. The virus infects a variety of human cells, but its effect on lymphocytes accounts for the severe immunologic abnormalities that are characteristic of AIDS.6 There is a profound reduction of the CD4+ T-lymphocyte subpopulation, although only a minority of peripheral CD4+ T lymphocytes is found to be infected. The mechanism whereby large numbers of CD4+ T lymphocytes are destroyed is not completely understood. Lymphocyte dysfunction leads to profound defects in cellular immunity, including cutaneous anergy and decreased in vitro lymphocyte proliferative responses to various mitogens and antigens. In addition, patients develop alterations in humoral immunity and in immunoregulatory mechanisms.7 Polyclonal B-cell activation results in elevated levels of immunoglobulin G (IgG) and immunoglobulin A (IgA). Circulating immune complexes are also a common finding.
AIDS is now defined by the Centers for Disease Control and Prevention (CDC) as either the occurrence of specific “index diseases,” such as Kaposi sarcoma (KS) or Pneumocystis carinii pneumonia, to which patients are susceptible because of HIV infection, or a CD4+ T-lymphocyte count <200 cells per μl of blood in an HIV-infected individual.8
HIV infection is transmitted by sexual activity (in particular, men who have sex with men or women who have sex with men at risk for HIV infection) or through receipt of infected blood or blood products. Groups at risk include intravenous drug users who share contaminated needles; hemophiliacs; recipients of whole blood transfusions; and rarely, those with accidental needle-stick injury. The disease can also be transmitted in utero to children of mothers with HIV infection.
HIV has been recovered from most ocular tissues, including the retina and cornea, and is shed in tears. It does not appear to cause clinically apparent disease in most individuals but may occasionally cause nonspecific intraocular inflammation. Occasionally, HIV-infected patients are found to have chronic iridocyclitis that cannot be attributed to any secondary intraocular infection or systemic inflammatory disease.9,10 The iridocyclitis has been reported to resolve in some patients with antiretroviral therapy (zidovudine), suggesting a direct relationship to HIV. Alternatively, inflammation might be the result of an unidentified infectious agent of low virulence that is successfully suppressed with improvement in the host’s immune function. HIV infection may also play a role in the development of chronic multifocal retinal infiltrates, which is a disorder characterized by anterior chamber and vitreous humor inflammatory cells, and multiple faint, yellow-white or translucent, discrete foci of inflammatory cells on the surface of the peripheral retina, with or without retinal vascular sheathing;11 however, the direct involvement of HIV in this uncommon disorder has never been confirmed.
There have been other HIV-infected individuals without evidence of secondary intraocular infections who have decreased vision, constricted visual fields, and reduced or extinguished electroretinograms. It has been suggested that these findings might represent other manifestations of direct infection with HIV; alternatively, they may be indirect effects of HIV infection, resulting from the retinal microvasculopathy that is a universal finding in HIV-infected individuals.2,3,4,12,13
The mechanism by which HIV disease causes the retinal microvasculopathy (manifested clinically by cotton-wool spots and retinal hemorrhages) is unknown. HIV infection of the endothelial cells with subsequent vascular occlusion does not fully explain all findings of the condition, nor does it account for the marked similarity between HIV-associated retinal microvasculopathy and retinal microvasculopathy seen in diabetes mellitus or some connective tissue disorders, such as systemic lupus erythematosus. Also, infection of endothelial cells is not a consistent finding in patients with retinal microvasculopathy.14 Alternative hypotheses suggest that vascular damage results from immune complex deposition or hemorheologic abnormalities.13,15,16,17,18
HIV also appears to serve directly as a contributing factor in the pathogenesis of some opportunistic infections, as described later for CMV retinitis.
Numerous antiretroviral drugs have been developed to treat HIV infection.19 Treatment that includes specific combinations of antiretroviral drugs has come to be known as highly active antiretroviral therapy (HAART). Successful HAART results in an elevation of CD4+ T-lymphocyte counts and a drop in HIV levels in the blood. These changes reflect restoration of immune function that markedly reduces the incidence of opportunistic infections, including those involving the eye, and increases survival.20,21,22
Opportunistic Infections of the Retina and Choroid
Infections of the eye (Table 1) are among the most feared complications of HIV infection, although ocular infections occur less commonly than nonocular infections with the same agent3 (Table 2). Those involving the retina and choroid tend to be severe and are associated with a high rate of vision loss.
Table 1. Infectious Agents That Cause Ophthalmic Disease in Human Immunodeficiency Virus–infected Individualsa | |||
|---|---|---|---|
|
Table 2. Autopsy Findings in 35 Patients with Acquired Immunodeficiency Syndrome | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||
CMV retinitis is an AIDS-defining illness.8 Varicella-zoster virus (VZV) retinopathy and toxoplasmic retinochoroiditis are the only other retinal infections that are seen with any regularity, but they were still far less common than CMV retinitis during the era before the availability of HAART. The remaining retinal infections associated with AIDS are uncommon. Endogenous bacterial infections of the retina, for example, have been reported only rarely.23,24 Choroidal infections are less common than retinal infections, but the spectrum of reported causes is larger; infecting agents include both Mycobacterium tuberculosis and nontuberculous mycobacteria and a variety of fungi, including P. carinii.25 The characteristic spectrum of opportunistic infections that occurs in AIDS is undoubtedly a reflection of the specific immunologic defects of the disease. The systemic and local factors that protect against a higher incidence of these infections in the eye remain to be elucidated.
Retinal and choroidal involvement is a manifestation of disseminated infections, in which the massive proliferation of organisms may overwhelm the patient’s limited immune defenses. They are usually seen late in the course of the syndrome; thus, they may actually signal further waning of immune defenses. Patients with intraocular infections should be suspected of having tissue-invasive infections involving other internal organs. When they do occur, intraocular infections are frequently extensive and severe. Concurrent infections with multiple organisms have been reported.
HIV infection and its sequelae have been studied in a variety of animal models. Rhesus monkeys infected with simian immunodeficiency virus (SIV) develop an AIDS-like illness. In this model, the monkeys develop a variety of ophthalmic lesions, including CMV infections of the retina.26
Cytomegalovirus
CMV is a ubiquitous, enveloped DNA virus of the herpes group. Up to 50% of adults in many populations have been infected with CMV, but in most cases, it does not cause any clinically apparent disease; however, the virus remains in the body as a latent infection. Two viral genes (UL97 and UL54) have been given special attention because of their role in development of resistance to anti-CMV drugs.27,28,29,30,31 UL97 encodes a phosphotransferase that is required for an initial phosphorylation of the anti-CMV drug ganciclovir. Mutations of UL97 therefore limit the conversion of ganciclovir to its active form. UL54 encodes DNA polymerase; mutations confer resistance not only to ganciclovir but also to the anti-CMV drugs foscarnet and cidofovir as well. Drug resistance generally develops during therapy, as mutant strains emerge in response to drug exposure.31
In patients with AIDS, CMV can cause life-threatening infections involving many tissues, including the brain, lungs, and gastrointestinal tract. CMV causes a necrotizing retinitis that can result in severe vision loss.32,33,34 Prior to the introduction of HAART, the reported prevalence of CMV retinitis varied from 4% of ambulatory patients (primarily intravenous drug abusers)35 to 34% of eyes in an autopsy series of male homosexuals.3 This discrepancy may reflect the fact that CMV retinitis occurs late in the course of AIDS. The introduction of HAART has reduced the incidence of AIDS-related CMV retinitis but has not eliminated it altogether.32,34
The major risk factor for CMV retinitis is severe immunodeficiency. Prior to the introduction of HAART, the infection almost always occurred in patients with CD4+ T-lymphocyte counts <50 cells per μl.36,37 Among patients who develop CMV retinitis while on HAART, the majority also have low CD4+ T-lymphocyte counts, indicating failure of treatment to effect or maintain immune reconstitution.34 There is no obvious correlation between the development of CMV retinitis and levels of CMV antibodies. CMV retinitis has been reported without detectable anti-CMV antibodies in the blood.38
CMV retinitis is more common among patients with AIDS than among other severely immunosuppressed individuals infected with CMV. The frequent development of CMV retinitis may be related in part to the retinal microvasculopathy that is common to HIV-infected individuals. Ultrastructural studies of retinal capillaries have demonstrated basal lamina thickening, swelling of endothelial cells, narrowing and occlusion of vascular lumina, and loss of pericytes.3 This microvascular disease may allow access of virus to retinal tissue through damaged vessel walls. Alterations of blood flow through the retinal circulation may also contribute to infection by increasing the contact time between circulating infected cells and the retina.13,15,16,17 Furthermore, HIV may act as a cofactor in development of CMV retinitis. Both viruses have been found in the same retinal cells at autopsy.39 Interactions between the two viruses, which are known to occur in vitro,40,41 may enhance the activity of CMV in coinfected cells. Among HIV-infected individuals, CMV retinitis is more common in men who have sex with men than in other risk groups, probably because of greater exposure to CMV.4,42
A great deal has been learned about the natural history of CMV retinitis during the course of the AIDS epidemic. Hematogenous spread of virus to the eye is supported by laboratory, clinical, and histopathologic findings. There is a relationship between levels of CMV in the blood and development of CMV retinitis in patients with AIDS.43,44 CMV-like virus particles have been observed within macrophages in the choroidal circulation of a patient with AIDS and viremia.45 CMV retinitis frequently begins adjacent to retinal vessels in the posterior pole33 (Fig. 1). In patients without AIDS, the spread of disease along vessels has been attributed to infection of vascular endothelial cells, which break free and travel through the retinal circulation.46 In support of this hypothesis, inclusion bodies have been identified in retinal endothelial cells of organ transplant patients with CMV retinitis. Endothelial cell inclusions have been reported rarely in choroidal tissue of AIDS patients.47,48 In autopsy studies,2,3 no CMV antigen has been identified in retinal endothelial cells by immunochemical techniques, even in vessels that traveled through areas of retinitis. Thus, endothelial cell infection may not play a major role in the spread of CMV retinitis in all patients. In contrast, Rao and associates49 studied eyes of patients with AIDS and perivascular CMV retinitis lesions and found a lack of endothelial cells in the adjacent vessels, suggesting that they may have been infected and destroyed early in the infection.
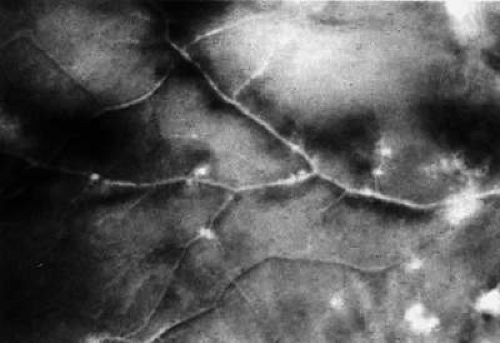 Figure 1. Gross autopsy specimen. Early foci of CMV retinitis are seen as white, granular patches adjacent to retinal vessels (original magnification 12×, printed with permission from Pepose JS, Holland GN, Nestor MS et al: Acquired immune deficiency syndrome: Pathogenic mechanisms of ocular disease. Ophthalmology 92:472, 1985.) |
Usually, infection begins with an isolated focus of disease; rarely are there more than two or three discrete areas of infection within the eye.33 These lesions invariably enlarge to involve additional retinal tissue; new lesions develop less frequently. The enlargement of lesions does not progress at the same rate from all lesion borders.50 Border advancement is faster in an anterior direction, toward the ora serrata, than in a posterior direction, toward the fovea. In some cases, the disease appears to move circumferentially around the fovea (Fig. 2). Historically, CMV retinitis was considered a “foveal-sparing” disease; in a series of organ transplant patients with CMV retinitis reported by Egbert and associates51 prior to the AIDS epidemic, only 3 of 21 eyes had macular involvement; however, studies of patients with AIDS show that infection can begin at or near the fovea.33 Advancement of lesion borders will halt at the ora serrata.3 Following total retinal necrosis, it is replaced by a thin gliotic membrane.45 No virus can be identified in ocular tissue at this late stage.
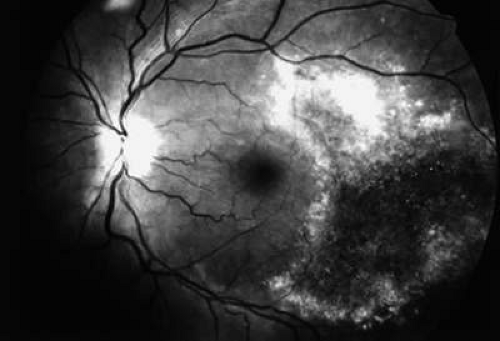 Figure 2. CMV retinitis in the left eye of a patient with AIDS. Disease has reactivated at lesion borders, and the posterior border is advancing in a circumferential manner around the fovea. |
Retinal necrosis can result in numerous retinal holes, which in turn place patients at risk for retinal detachment, estimated to occur in 38% of patients at 1 year after diagnosis of CMV retintis.52 Large lesions52,53 and lesions that extend to the vitreous base54,55 are associated with an increased risk of retinal detachment.
Without anti-CMV therapy, the progression of CMV retinitis in severely immunodeficient patients is a slow but relentless process, with total destruction of the retina occurring over a period of months.45 In contrast, with the immune reconstitution associated with HAART, CMV retinitis may eventually become inactive, even without treatment, as immune function improves.56 In most patients who respond to HAART, specific anti-CMV drug therapy can therefore be discontinued without disease reactivation; however, progression of CMV retinitis does occur in a few patients despite laboratory evidence of immune reconstitution,57 possibly because of persistent defects in specific immunity against CMV in those patients, and despite improvements in nonspecific laboratory measures of immune function such as CD4+ T-lymphocyte count.58,59
The histopathologic characteristics of AIDS-related CMV retinitis in one autopsy study are listed in Table 3.3 Such studies demonstrate the tissue necrosis and cytomegalic cells characteristic of all CMV infections2,3 (Fig. 3). Electron microscopic and immunohistochemical studies have identified CMV viral particles and antigen in a patchy distribution throughout all layers of the retina and occasionally in contiguous retinal pigment epithelial cells.3 Viral antigens are only rarely identified in the choroid.3,48 Viral antigen in the choroid has been found in association with vessels and is not always adjacent to areas of retinitis, suggesting that the virus reaches the choroid through independent hematogenous spread rather than by extension of infection from the retina.
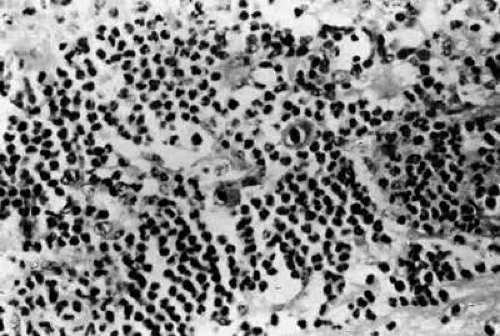 Figure 3. CMV retinitis, with neutrophilic infiltration in an area of necrotic retina. Cytomegalic cells with intranuclear inclusions are present in the center of the field (hematoxylin-eosin; original magnification 600×, printed with permission from Pepose JS, Holland GN, Nestor MS et al: Acquired immune deficiency syndrome: Pathogenic mechanisms of ocular disease. Ophthalmology 92:472, 1985.) |
Table 3. Autopsy Findings in Acquired Immunodeficiency Syndrome Patients: Characteristics of Cytomegalovirus Retinitis | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||
Autopsy studies have also shown that the retinal whitening of CMV retinitis (in patients with AIDS as well as in those who are immunodeficient for other reasons) is attributable to retinal necrosis and edema; there is usually only a sparse lymphocytic infiltrate. Autopsy studies have also shown that 22% to 50% of patients with AIDS-related CMV retinitis will have focal neutrophilic infiltrates in retinal tissue,3,45 which is atypical when compared with CMV retinitis in patients without AIDS. The difference has been attributed to intact granulocyte function and chemotaxis in patients with AIDS, in contrast to infants, organ transplant recipients, and patients with malignancies who can have more severe quantitative or qualitative granulocyte dysfunction.3 Acute inflammatory cells may extend into the subjacent choroid despite the absence of identifiable viral antigens.3 A variety of stimuli (CMV antigen, immune complex deposition, tissue necrosis) may be responsible for the production of chemotactic factors leading to neutrophilic infiltration. Immunohistochemical studies have revealed deposition of IgG, IgA, and, to a lesser extent, immunoglobulin M (IgM) and C3c in retinal tissue and within retinal arteriolar walls.3 Many IgA-bearing plasma cells were present in one case.2 Perivascular infiltration of neutrophils occurs, consistent with immune complex–mediated vasculitis,2,3 but there is poor correlation between the distribution of tissue-bound immunoglobulins, acute inflammatory cells, and CMV antigens.3 Thus, it is also possible that concurrent retinal infection with other unidentified pathogens is responsible for the acute inflammatory reaction seen in these eyes. Inflammatory cell products do not appear to play an important role in the extensive tissue destruction common to all cases of CMV retinitis.
The anterior chamber reaction associated with CMV retinitis is typically mild and does not result in complications, such as elevated intraocular pressure or posterior synechiae. Corneal endothelial deposits are a frequent manifestation of the reaction;60,61,62 these keratic precipitates are fine, stellate or reticular flecks distributed diffusely on the endothelial surface. Histologically, they have been found to be macrophages and fibrinous material without lymphocytes or evidence of CMV infection of endothelial cells. The vitreous humor usually remains remarkably free of inflammatory material despite the presence of virus in the vitreous cavity.47
Patients with AIDS-related CMV retinitis who begin HAART may develop immune recovery uveitis (IRU) as a result of their improved abilities to mount immunologic reactions against intraocular CMV.63,64,65,66,67,68,69,70,71,72 It is analogous to the marked intraocular inflammatory reactions that have been noted in patients on immunosuppressive drugs who have CMV retinitis when those drugs are withdrawn.51 Inflammation associated with IRU is most prominent in the vitreous cavity but can also involve the anterior segment. Complications of IRU include optic disc edema, cystoid macular edema, epiretinal membrane formation, vitreomacular traction syndrome, retinal neovascularization, posterior synechiae, and cataract. Vision can be lost if complications of inflammation occur.
The reported incidence of IRU among people with AIDS-related CMV retinitis who receive HAART has varied from 0.109 cases per person-year to 0.83 cases per person-year.66,69 In a large multicenter study, 17.6% of patients with AIDS-related CMV retinitis who met criteria for immune reconstitution had IRU.72 The reason that not all patients develop IRU is unknown; however, there may be qualitative differences in the immune response between immune reconstituted patients with and those without IRU.73 Also, studies have identified a number of risk factors for IRU. People with larger CMV retinitis lesions are at increased risk for IRU, presumably because there is more viral antigen in the eye.70,72 A history of the treatment with the antiviral agent cidofovir is also a risk factor,71,72 presumably because the drug itself can cause uveitis.74 A history of more intense anti-CMV treatment possibly reduces the risk of IRU by limiting the amount of viral antigen,68 but continued treatment of healed CMV retinitis after immune reconstitution does not appear to prevent IRU.71
Initial vitreous inflammatory reactions may improve over a period of 6 weeks, whether or not anti-inflammatory therapy is administered,64 but tissue damage, if it occurs, and anterior segment inflammation may persist.63,66,67 Macular edema, in particular, tends to be a persistent problem that is refractory to treatment.
Human CMV is highly species specific, making the study of human CMV infections in animal models difficult. Attention has therefore been focused on murine CMV infections in mice as a possible model for the study of human CMV retinitis. Holland and associates75 showed that murine CMV was capable of causing retinal necrosis in immunosuppressed mice. Other investigators have subsequently studied the role of immune defenses against murine CMV retinitis;76,77 however, there are many differences between murine and human CMV infections of the eye, and extrapolations about disease mechanisms to human CMV retinitis should be made with caution. For example, murine CMV seems to have a propensity for uveal tissue, unlike its human counterpart. Also, susceptibility of murine and human CMV isolates to various antiviral agents is very different, making these models of little use for the investigation of new antiviral agents. A rabbit model of disease using human CMV has also been reported.78 Chorioretinal inflammation and destruction were seen, but this model has not subsequently been used for clinical studies of human retinal infection.
Varicella-zoster Virus
VZV can also cause a severe necrotizing retinopathy in HIV-infected patients79,80,81,82,83 (Fig. 4). It may present as an isolated infection or may occur concurrently with or after cutaneous herpes zoster in any dermatomal distribution. It has also been associated with VZV encephalitis.83 In most HIV-infected patients, VZV retinopathy presents as a distinctive clinical disorder known as the progressive outer retinal necrosis (PORN) syndrome.81 It is characterized by multifocal, deep, opaque retinal lesions (believed to be retinal edema) that rapidly extends to full-thickness necrosis, with coalescence of lesions. The retina can be completely involved over a period of a few days to a couple of weeks. There is little or no vitreous or anterior chamber inflammatory reaction. Occlusive vasculitis is not a primary feature of the disease, although patients are ultimately left with severe vascular attenuation. The optic nerve may be hyperemic, and optic atrophy is a sequela of the infection.
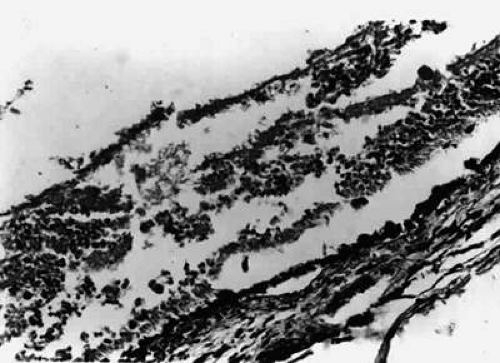 Figure 4. VZV retinitis with full-thickness retinal necrosis. There is little associated inflammation (hematoxylin-eosin; original magnification 280×, photograph courtesy of Todd P. Margolis, M.D., Ph.D.) |
Histopathologic examination of two cases showed viral antigens and viral particles in the outer retinal layers, consistent with the appearance of deep retinal lesions.80 There were variable amounts of inflammation in the retinas and scattered areas of choroidal inflammation, although there was no evidence of choroidal infection by the virus. Histopathologic examination of two additional cases showed VZV infection of the retinal pigment epithelium (RPE) and greater involvement of the outer than inner retinal layers, consistent with the clinical appearance of lesions.83
The infection responds poorly to antiviral therapy.81 Even among patients with response to therapy, recurrence of disease is common.79,81 At the time of disease recurrence, the development of new lesions, including involvement of the second eye in unilateral cases, is more common than reactivation of preexisting lesions.79,81 These new lesions may therefore be the result of repeated episodes of viremia, or they may have arisen from clinically inapparent virus in the retina.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


