Ocular Histoplasmosis Syndrome
Norbert Becker
Howard H. Tessler
The ocular histoplasmosis syndrome, often termed the presumed ocular histoplasmosis syndrome (POHS), refers to a choroidopathy believed to be caused by the fungus Histoplasma capsulatum. Koch’s postulates have not proved Histoplasma to be the cause of this eye disease; instead, epidemiologic evidence has been used to implicate this fungus as the cause of the syndrome. POHS clinically presents as multiple depigmented or pigmented atrophic choroidal spots, peripapillary atrophy, subretinal hemorrhagic disciform maculopathy, and clear uninflamed media.
H. capsulatum is a dimorphic fungus that grows in nature or on Sabouraud’s agar at room temperature as a mold. It grows as small budding yeast; however, in host tissue despite its name, H. capsulatum is an unencapsulated organism. The fungus is encountered in many areas of the world but is most common in the southeastern, Middle Atlantic, and central United States. The endemic regions are probably determined by availability of the conditions necessary for the growth of the fungus. H. capsulatum is most commonly found in surface soil, particularly when enriched by the droppings of certain birds and bats. Exposure to such dust, which may occur by raking, cleaning dirt floor chicken coops, bulldozing, or spelunking, may stir up the organism and cause aerosol formation.1 Microconidia of H. capsulatum are most frequently infective by way of the respiratory route and are small enough to reach alveoli on inhalation. These microconidia are often smaller than 5 μm.
An intense granulomatous reaction may occur and may lead to caseation necrosis or calcification, which may mimic tuberculosis. The primary infection usually heals completely, but calcific granulomas may be left in the hilar nodes or lungs. Transient dissemination of the disease may lead to calcific granulomas in the spleen. In a few patients, histoplasmosis becomes a progressive and even potentially fatal disease. A patient predisposed to progressive disease usually has a history of cigarette use and associated chronic obstructive pulmonary disease.2 A rapidly fatal form of the disease exists and is usually encountered in young children and immunosuppressed individuals.3 Systemic histoplasmosis is an uncommon manifestation of AIDS.4
Most infections are either asymptomatic or very mild. They are usually manifested by cough, fever, and malaise, and chest radiograph findings show hilar adenopathy. Definitive diagnosis requires demonstration of the organism by culture or histology. Culture of H. capsulatum is difficult but is the procedure of choice with pulmonary involvement. Acute pulmonary histoplasmosis requires no therapy, but chronic fibronodular pulmonary histoplasmosis and disseminated histoplasmosis are treated with oral itraconazole or amphotericin B.5
Ocular Involvement
Three types of proven and presumed ocular involvement by H. capsulatum have been described in humans: histoplasmic endophthalmitis, solitary histoplasmic chorioretinal granuloma, and POHS. Histoplasmic endophthalmitis is usually recognized in patients with disseminated histoplasmosis.6 None of the characteristic lesions of POHS are seen in eyes with histoplasmic endophthalmitis. Ocular involvement usually begins as a peripheral focal retinitis associated with vitritis and iridocyclitis. The diagnosis is made by cultures of the aqueous and vitreous. Treatment is with systemic amphotericin B and itraconazole.7 Intravitreal injections are used in severe cases that are unresponsive to systemic treatment. Solitary histoplasmic chorioretinal granulomas (histoplasmoma) are a rare presentation of ocular involvement with the H. capsulatum organism.8 They present as a solitary granuloma and may mimic ocular toxocariasis. This type of granuloma and histoplasmic endophthalmitis is often seen in immunocompromised individuals and is becoming even more common as a result of the widespread use of chemotherapeutic agents.3,4
Historical Viewpoint
Krause and Hopkins9 in 1951 reported a case of exudative chorioretinitis that flared up after skin testing with the histoplasmin antigen. Schlaegel10 hypothesized that H. capsulatum may be a cause of choroiditis without anterior segment inflammation. In 1960, Woods and Wahlen11 described POHS in detail and postulated that histoplasmosis was the probable cause of a mild disseminated chorioretinitis and was also a cause of disciform detachment of the macula. The H. capsulatum organism has never been cultured from an individual with POHS. A report by Roth12 in 1977 showed histopathologic findings suggestive of Histoplasma organisms. Gass and Zimmerman disputed this finding.13 Khalil14 and others15,16,17 have demonstrated organisms suggestive of H. capsulatum in clinically inactive lesions in an eye that was enucleated because of melanoma.
Clinical Manifestations
In the United States, POHS is an important cause of loss of central acuity.18 This syndrome affects patients during their most productive years, in the third, fourth, and fifth decades of life.19 POHS is characterized by four clinical manifestations: a disseminated choroiditis producing the so-called histo spots; subretinal choroidal neovascularization, usually in or adjacent to the macula; peripapillary chorioretinal atrophy; and clear ocular media.
Histo Spots
Histo spots (Fig. 48.1) represent a multifocal or a disseminated choroiditis characterized by atrophic or yellowish white scars in the posterior pole and the periphery. In 1972, Smith et al.19 showed the number of disseminated scars to range from 0 to 102. They occurred bilaterally in 62% of the patients, with the majority of the scars found posterior to the equator. The spots have sharp borders and frequently are partially pigmented. They do not appear to be active areas of choroiditis with swelling and cellular exudation. The random distribution of the scars throughout the midperipheral areas and posterior pole of the fundus suggests a hematogenous dissemination of H. capsulatum to the eye. Histo spots seem to have a predilection for areas of greater blood supply. Skin testing in 59% of the general population in an endemic area was positive for the histoplasmin antigen; however, only 4.4% of this group was found to have histo scars on clinical examination.20
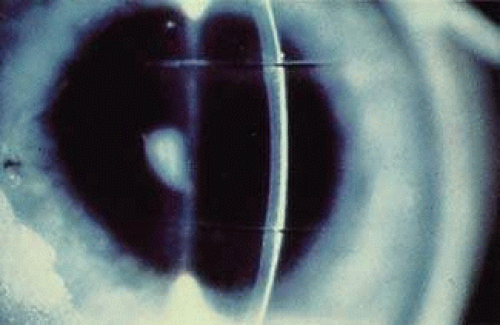 FIGURE 48.1 Histo spots. Note the punched-out appearance. Some spots contain pigment and others are depigmented. Choroidal vessels often can be seen, indicating these scars are old and not actively inflamed. |
About 5% of patients with POHS demonstrate what have been called peripheral streak lesions of the fundus. These streaks are of variable length and pigmentation (Fig. 48.2).21 The streak lesions are most likely to be the result of a linear aggregation of histo spots. The histo spots are normally stable but may undergo changes in shape, size, and intensity. They have been shown to become larger over the course of time. The mechanism of change in size and shape of these lesions is unknown. Long-term follow-up has shown that 9% to 16% of patients will develop new histo spots.22,23,24 It has also been shown that 50% of eyes will have changes in atrophic scarring manifested by increased size or by formation of new scars in the peripapillary, macular, and peripheral regions. In 1969, Krill and associates25 described the evolution of these choroidal infiltrates as being hypofluorescent in the early stages of the disease. During the course of time, they assume a hyperfluorescent appearance, which is more characteristic of the mature lesions. Therefore, the late atrophic histo spot has the fluorescein angiographic picture of a pigment epithelial window defect.
 FIGURE 48.2 Linear streaks are sometimes seen in ocular histoplasmosis. These streaks may represent coalescent histo spots. There are some nearby typical histo spots. |
Peripapillary Atrophy
A ring of peripapillary atrophy (Fig. 48.3) occurs in the majority of cases of POHS. This ring is characteristic, with a narrow inner pigment zone adjacent to the disc edge and a white depigmented zone away from the disc. It is hypothesized that a circle of granulomas forms during the active infective stage of the disease and that these granulomas atrophy, leaving the ring of peripapillary atrophy. Neovascular membranes can occur in these rings of atrophy and sometimes involve the macula.26
 FIGURE 48.3 Peripapillary atrophy. Note the characteristic ring of pigment adjacent to the disc, with the depigmented ring more distal. |
Macular Lesions
It is the macular lesions that bring patients to an ophthalmologist with symptoms of metamorphopsia. Subsequently, patients may develop profound loss of central visual acuity.
Histo spots located in the macular area tend to develop choroidal neovascular membranes (CNVMs; Fig. 48.4). These CNVMs are similar to those seen with age-related macular degeneration, angioid streaks, and choroidal ruptures.27 Histologically, there is an egress of capillaries from the choroid to the subretinal space between Bruch’s membrane and the neurosensory retina.
 FIGURE 48.4 Signet ring (gray-green lesion) in macula indicating a probable subretinal neovascular net. There is characteristic peripapillary atrophy of presumed ocular histoplasmosis syndrome. |
The reason for the formation of CNVMs in the macular area in POHS, as in age-related macular degeneration, is not understood. Some investigators have postulated that an immune reaction against H. capsulatum may play a part. Others believe that the CNVMs are just a deterioration that accompanies any break in Bruch’s membrane.27 Ophthalmoscopically, CNVMs may first appear as dirty gray-green subretinal lesions. This formation has been likened to a signet ring. The initial lesions may progress to actual subretinal hemorrhage. Deposition of lipid and serous elevation of the retina may also occur as a result of increased permeability in the CNVMs. In time, this condition progresses to an atrophic or gliotic scar, which may assume various forms. Most of the scars are white because of fibrous tissue that develops secondary to the hemorrhage. Microcystic degeneration of the sensory retina may also occur as a result of chronic serous detachment of the neurosensory retina. The visual acuity in patients who have had CNVMs is seldom better than 20/200, unless the location of the scars is eccentric to the fovea. In one retrospective study, only 14% of untreated eyes with subfoveal neovascular networks ended with a 20/40 acuity.28 If the scar is greater than several disc diameters, the vision may fall to the counting fingers level. Just as in age-related macular degeneration, choroidal neovascular membranes may progress to massive vitreous hemorrhage. This infrequent circumstance is due to an actual hemorrhage through a break in the neurosensory retina.29,30
Ocular Media
The ocular media in patients with POHS are absolutely clear of cells. No inflammatory cells can be found in either the aqueous or vitreous. Part of the reason for this lack of cells may be because the inflammatory stage has ended by the time patients are seen clinically. Another possibility is that inflammatory cells deep in the choroid have difficulty penetrating into the vitreous. This finding is in contrast to toxoplasmosis, a retinochoroiditis, in which the primary inflammation lies in the retina. Subsequently, in toxoplasmosis, cells spill over into the vitreous and aqueous. Patients who have vitreous or aqueous cells and present with peripheral punched-out lesions, peripapillary atrophy, and macular CNVMs should be diagnosed as having multifocal choroiditis (also called pseudohistoplasmosis).31,32 The cause of the pseudohistoplasmosis syndrome has been described to include presumed sarcoidosis, possibly tuberculosis or syphilis. In about 30% of patients, no cause of multifocal choroiditis can be determined.
Exacerbation and Recurrences
A significant reduction in central visual acuity is caused by POHS in at least 2,000 young and middle-age adults every year in the United States. About 0.5% of cases of legal blindness in Tennessee are due to histoplasmosis.8 Most exacerbations occur at the site of previous histo scars. The chance of macular involvement primarily depends on whether histo spots are present in the macula at the time of the recurrence. Lewis et al.33 noted a 23% risk of developing asymptomatic macular lesions in a contralateral eye with asymptomatic macular scars. Their finding agrees with the 20% rate of onset in the second eye in 3 years reported by Elliot and Jackson34 and by Sawelson et al.35 Lewis et al. found that 58% of untreated eyes with macular CNVMs eventually deteriorate to a visual acuity of 20/200 or worse.
In a study by Watzke and Claussen,29 16.6% of eyes developed new infiltrates in the choroid and retina in areas that were clinically and angiographically normal 10 years previously. The basic lesion was found to be a nodular choroidal infiltrate that evolved clinically and angiographically from normal retina. Angiographically, the lesion was initially hypofluorescent with the later hyperfluorescence of a choroidal scar.
Geographic Distribution and Epidemiology
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


