Ocular Allergic Disorders
Samir M. Haq
Sonali Singh
Brian J. Song
Stefan D. Trocme
The defense system of the body is designed to protect itself from infections and other harmful agents. The components of the immune system include the immunoglobulins, T and B lymphocytes, and other mediators of cell immunity. An exaggerated immune response, especially to a minor stimulation, may be of harm to the host. The unique location of the ocular surface exposes it to a variety of environmental antigens. The interaction of the environmental antigens (allergens) with the immunologically active cells and immunoglobulins of the eye leads to allergic inflammatory disorders of the eye.
History
In 1906, Von Pirquet1 used the word “allergy” to describe this state of altered reactivity. The term atopy was coined by Coca and Cooke2 to denote a wheal-and-flare skin reaction to antigen challenge in an individual with a history of allergy. Prausnitz and Kustner3 were the first to describe a wheal-and-flare reaction to an intracutaneous injection of fish extract in a person sensitive to the antigen. They also demonstrated that the reactivity may be transferred to the skin of a nonsensitized person by injection of serum from sensitized individuals (Prausnitz-Kustner reaction). The transferable serum component was called reagin. Later research revealed the component present in the serum reagin to be a new class of immunoglobulin, called immunoglobulin E (IgE) by the World Health Organization (WHO). In present day clinical practice, the term allergy refers to an acquired hypersensitivity and hyperreactivity to a foreign substance (allergen) resulting in damage to host tissues.
The symptoms that we currently attribute to ocular and nasal allergies following exposure to plant products were first described by Blackley in 1873.4 Peshkin used the allergen challenge model, also called conjunctival provocation testing (CPT), in conjunction with skin tests to diagnose ocular allergy.5 The model was also used by Abram6 and Tuft,7,8 especially in cases in which skin tests were inconclusive. In research settings, the allergen challenge test allows a reproduction of the allergic response in a controlled environment. It has been used to establish cytokine profiles at various stages in the allergic reaction9 and to evaluate the efficacy of specific therapeutic interventions.10
Incidence and Prevalence
The exact incidence and prevalence figures for allergic disorders are unknown due to considerable under-reporting. Skin test surveys suggest that as many as 40 to 50 million people in the United States suffer from allergies.11 It is estimated that up to 22% of the population suffers from allergic eye disease,12 and the percentage continues to rise.13
Economic Impact
The economic burden created by ocular allergic disorder is increasing with the increasing cost of health care. It is estimated that the medical costs are between $1.5 and $2 billion annually in the United States alone. Aside from the monetary costs, these disorders significantly affect the quality of life of the affected patients.14
Classifications of Ocular Allergic Disorders
Allergic eye diseases are generally classified into four types:
Hay fever conjunctivitis
Atopic keratoconjunctivitis
Vernal keratoconjunctivitis
Contact lens–associated giant papillary conjunctivitis
Hay Fever Conjunctivitis
Hay fever conjunctivitis is the most common ocular allergic disorder, accounting for 50% to 80% of all case of allergic conjunctivitis.15 Hay fever conjunctivitis is a manifestation of type I or immediate hypersensitivity reaction mediated by IgE. A variety of airborne antigens, such as pollen, dry grasses, weeds, spores, and dust, may trigger the allergic reaction. Based on the nature of the offending allergen, hay fever conjunctivitis may be further subdivided into seasonal (SAC) or perennial allergic conjunctivitis (PAC).
Pathogenesis
Hay fever conjunctivitis results from an immediate or type I hypersensitivity reaction. Initially, an airborne allergen dissolves in tear film and binds to the IgE antibody. This initial sensitization process is not associated with an inflammatory response. Subsequent exposure to the allergen initiates an allergic reaction, which may be divided into an early phase and a late phase.
During the early phase, an antigen to binds to the sensitized IgE–mast cell complex, resulting in degranulation. This releases numerous inflammatory mediators including histamine, proteases, prostaglandins, and leukotrienes.16 The itching, redness, and tearing of the early phase may be directly attributed to histamine.17
After an asymptomatic interval, late-phase manifestations may be detectable.18 Cytokines from the early phase recruit other proinflammatory cells, such as eosinophils and neutrophils, to the conjunctiva.19,20 These cells, and the mediators they secrete, characterize the late-phase response.
The proinflammatory cytokines present in symptomatic atopic individuals may influence ocular wound healing. Communication between proinflammatory cytokines and the cornea has the potential for visual morbidity. Untreated atopic individuals undergoing laser in situ keratomileusis (LASIK) are at an increased risk for postoperative complications, such as diffuse lamellar keratitis (DLK). Boorstein and colleagues demonstrated that the use of appropriate allergy medication may greatly mitigate this risk.21 Table 30.1 summarizes the changes in cytokine levels in SAC and PAC.
TABLE 30.1. Changes in levels of tear and tissue cytokines during seasonal allergic conjunctivitis (SAC) and perennial allergic conjunctivitis (PAC). | ||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||
Symptoms
Patients present with ocular itching, burning, redness, and excess tearing. SAC and PAC frequently are associated with symptoms of allergic rhinitis and sinusitis. Affected individuals frequently provide a personal or family history of atopic phenomena such as eczema, asthma, or seasonal rhinitis. SAC presents seasonally with an abrupt onset of symptoms related to the specific pollens. Individuals with allergies to grass pollen are symptomatic in the months of May and June, whereas those with ragweed allergies manifest their symptoms in August and September. PAC presents with similar but year-round symptoms. It is triggered by year-round allergens, such as cat dander and house dust mites.22 The symptoms of PAC also tend to be milder. The age group is similar in both SAC and PAC. PAC is associated much more frequently with allergic rhinitis than is SAC. Seventy-nine percent of patients with PAC have seasonal exacerbation.23
Physical Examination
Examination of the eye in SAC reveals marked injection of the conjunctiva and episcleral vessels bilaterally (Fig. 30.1). Mild chemosis and edema of the eye lid may be present. The discharge is mostly watery but sometimes may be mucopurulent. The cornea remains unaffected. The ocular signs may be minimal, and only a careful examination would reveal dilation of the conjunctival vessels near the perilimbal area. The eye is frequently normal appearing, and it is only the presence of symptoms that suggests diagnosis. The clinical signs of PAC are usually minimal and, in fact, this normal appearance in the presence of year-round itching and tearing makes the diagnosis obvious.24
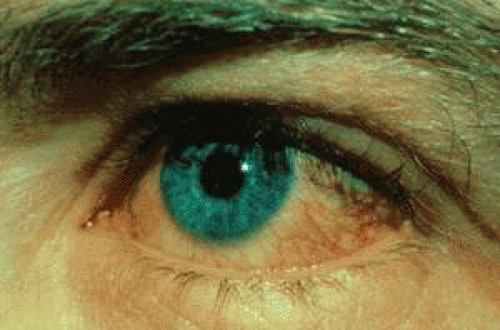 Figure 30.1. Mild hay fever conjunctivitis with conjunctival injection. |
Diagnosis
The diagnosis is made on the basis of history and clinical examination. The presence of eosinophils in conjunctival scrapings aids the diagnosis, but their absence does not exclude it. Tear tryptase, a protease released primarily from activated mast cells, may serve as an objective parameter of disease activity.25
Treatment
In the management of hay fever conjunctivitis, the primary treatment consists of separation from the causal allergen, cold compresses, and the use of topical ophthalmic lubricants. Immunotherapy, although not primary treatment, may have some efficacy.26
Topical Vasoconstrictors
Phenylephrine and naphazoline are topical vasoconstrictors used in the treatment of mild cases of allergic conjunctivitis. These medications act on sympathetic receptors to constrict conjunctival blood vessels. The use of topical vasoconstrictors is limited due to a rebound phenomena observed on discontinuation.
Topical Antihistamines
Topical antihistamines have demonstrated efficacy in the treatment of allergic conjunctivitis by competitively blocking histamine receptors. These drugs exhibit selectivity for H1 receptors and thus have great efficacy in the reduction of itching. Second-generation H1-receptor antagonists include levocabastine and emedastine. Levocabastine has demonstrated a rapid onset and a relatively prolonged activity.27,28,29 Emedastine exhibits selective H1 antagonism and has no apparent effect on adrenergic, dopaminergic, or serotonin receptors.30 The activity of topical antihistamines declines after 3 to 4 hours, and as such, frequent dosing is recommended. The addition of a topical vasoconstrictor may provide additional efficacy.
Mast-Cell Secretion Inhibitors
Cromolyn, lodoxamide, and perimolast are mast-cell secretion inhibitors commonly used in the treatment of allergic conjunctivitis. Cromolyn induces the phosphorylation of a mast-cell protein termed MACEDONIA (mast-cell degranulation inhibitory agent). It is postulated that MACEDONIA blocks mast-cell secretion through interactions with the cell cytoskeleton.31 Lodoxamide has demonstrated a potency of approximately 2,500 times that of cromolyn.32,33 Perimolast is under development in the United States and Europe for the treatment of allergic conjunctivitis. Its efficacy has been shown to be similar to cromolyn, but with a superior patient comfort profile.34 Mast-cell stabilizers may prevent symptoms, but they are not suitable for the treatment of acute symptoms.
Multimodal Medications
Bimodal medications act as both mast-cells stabilizers and antihistaminics.
Nonsteroidal Anti-Inflammatories
Nonsteroidal anti-inflammatories (NSAIDs) inhibit cyclooxygenase, resulting in a reduction of prostaglandin and thromboxane levels. NSAIDs have efficacy in the mitigation of itching and conjunctival hyperemia associated with SAC.37 NSAIDs are not associated with the negative complications of corticosteroids, such as ocular infections, increased intraocular pressure, or contribution to cataract formation.38 Ketorolac, diclofenac, and flurbiprofen presently are available for ocular use; however, only ketorolac is currently approved for treatment of SAC. Diclofenac appears to have similar efficacy to ketorolac in the treatment of SAC.39 The efficacy of flurbiprofen in the treatment of vernal keratoconjunctivitis (VKC) is documented, but further research is needed to warrant its use in allergic conjunctivitis.40
Soft Topical Steroids
Topical steroids have great potency when compared to other treatment options. They work by intervening at multiple pathways in the inflammatory cascade, thus making them extremely effective. However, these drugs typically are reserved for severe cases because of their potential side effects. A short-term use of topical steroids should be used concurrently with other allergy medications, which may be continued after steroid use is stopped.41 Soft steroids have been introduced as a safer alternative to traditional steroids. Loteprednol represent this class of drugs (42). Table 30.2 summarizes the treatment options for SAC and PAC.
TABLE 30.2. Treatment options for ocular allergy. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Atopic Keratoconjunctivitis
Atopic keratoconjunctivitis (AKC) is a chronic inflammatory condition of the eye occurring in patients with a history of atopic dermatitis. It involves predominantly the lower tarsal conjunctiva. The symptoms frequently are disabling, and corneal involvement may lead to blindness. Ninety-five percent of the patients have a personal or family history of atopic disorders such as dermatitis, eczema, or asthma. However, only 25% to 42% of patients with atopic dermatitis develop ocular disorders.12,43 In 1953, Hogan was the first to recognize the association of atopic dermatitis and ocular surface disorders.44 The common ectodermal origin of the skin and ocular structure and their close proximity explain this association.
AKC usually presents from the late teens to the second decade, many years after the initial presentation of atopic symptoms. In many patients, the manifestations of disease improve with age and may completely disappear. Severe cases, however, do persist in to later life. Older patients tend to have the more severe form of the disease, which has its peak incidence in the 30-to 50-year-old age group. Males are affected more often than are females.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


