Ocular Abnormalities in Acquired Heart Disease
Sunir J Garg
Arunan Sivalingam
James Bolling
Richard E. Goldberg
Jocelyn Sivalingam
Larry Magargal
In contrast to congenital heart disease, in which patients have cyanotic ocular findings (dilated, tortuous veins with or without retinal edema), patients with acquired cardiac diseases usually have symptoms secondary to embolic phenomena. These symptoms vary from transient visual obscuration to complete vision loss. The major categories of acquired heart disease that have ocular findings include infective endocarditis, nonbacterial (noninfective) thrombotic endocarditis (NBTE), atrial myxoma, mitral valve prolapse, and aortic arch syndrome, including inflammatory conditions that affect the major arteries, specifically Takayasu disease and syphilis. Ocular signs of these disorders include white-centered retinal hemorrhages (Roth spots), cotton wool spots, capillary nonperfusion, branch and central retinal artery obstruction, collateral arteriovenous communications, and endogenous endophthalmitis.
INFECTIVE ENDOCARDITIS
Infective endocarditis is infection of the heart’s endothelial lining and is classically manifested by vegetations on the cardiac valve surface. The development of endocarditis depends upon several factors. Conditions such as blood turbulence, hypercoagulable states, congenital cardiac disease, rheumatic and degenerative valvular disease,1,2,3,4 intravenous drug abuse,5,6,7 prosthetic heart valves,8,9 indwelling catheters, and pacemaker wires6,7,8,9 injure the endothelial cells of the valve triggering local deposition of fibrin and platelets. This injury produces vegetations that characterize thrombotic endocarditis and are usually located along the line of closure of the valve leaflet. Infective endocarditis develops when circulating microorganisms colonize the vegetation.10 Streptococcus spp. (viridans), Staphylococcus aureus, coagulase-negative Staphylococci, and Enterococci are the most common pathogens responsible for infective endocarditis. Escherichia coli, Salmonella, Klebsiella, and fungi have also been found.11
Endocarditis may present with a myriad of nonspecific symptoms, including malaise, fevers, chills, night sweats, anorexia, and dyspnea.1 On systemic examination, patients may have a heart murmur, splenomegaly, and petechial hemorrhages in their mouth or on their skin. Larger, painless, hemorrhagic macules on the palms and soles are called Janeway lesions, and painful nodules on the fingers and toes are called Osler nodes. The laboratory findings include anemia and leukocytosis. The erythrocyte sedimentation rate and C-reactive protein levels may be elevated and urinary abnormalities, such as proteinuria and hematuria, are frequently present. Although positive blood cultures occur in more than 90% of cases, at least three sets of sterile cultures should be drawn within 24 hours in order to establish the diagnosis. Cardiac echography is helpful; transthoracic echography has excellent specificity for detecting endocarditis (98%) but variable sensitivity. If clinical suspicion is still high despite a negative transthoracic echocardiogram, transesophageal echocardiography can be performed. It has a higher sensitivity than transthoracic echocardiography, with excellent specificity.12,13 Recently, 3D-transesophageal echography has been shown to provide a mild increase in sensitivity compared with 2D echography.14
Both cardiac and extracardiac complications of endocarditis can occur. Cardiac complications vary from arrhythmia to cardiac failure.15 Extracardiac manifestations usually result from thromboembolic phenomena. Distant embolization causes arterial obstruction with resultant ischemia and tissue infarction, localized abscesses, and mycotic aneurysm formation. CNS manifestations of infectious endocarditis include stroke, transient ischemic attacks, brain abscesses, meningitis, or mycotic aneurysms.16,17,18,19,20,21
Conjunctival petechial hemorrhages, iris abcesses,22 superficial or deep retinal hemorrhages,23 focal retinal and/or choroidal abscesses, vasculitis, choroidal neovascular membrane formation, and endogenous endophthalmitis24,25 are the major ocular complications of infective endocarditis. The classic ocular sign of infective endocarditis is a Roth spot (a white-centered hemorrhage; see Fig. 22.1). The white center is believed to be either a focal microabscess caused by a septic embolus or a fibrin and platelet clot, as seen in other disorders such as leukemia and diabetic retinopathy (Fig. 22.2).26 Retinal arteriole occlusion may produce cotton wool spots and branch or central retinal artery obstruction.27,28 The inflammatory emboli can also cause a choroiditis that can lead to choroidal neovascular membrane formation.29 Endogenous endophthalmitis is the most severe ocular complication of infective endocarditis. The treatment of endogenous endophthalmitis usually involves identification of the underlying organism and aggressive systemic treatment with the appropriate antibiotics. If there is clinical evidence of virulent endophthalmitis associated with significant vitreitis or hypopyon (Fig. 22.3), the physician should also consider intravitreal antibiotics, possibly in conjunction with pars plana vitrectomy.30 Several small, retrospective, nonrandomized reports suggest that systemic treatment with vitrectomy and intravitreal antibiotics may have better visual results than systemic treatment alone.31,32 Conversely, endogenous endophthalmitis may be the initial presenting sign of infectious endocarditis in a small subset of patients. A full systemic evaluation, including cardiac ultrasonography, should be performed in all patients with suspected endogenous endophthalmitis. The overall prognosis depends upon several factors, including underlying patient comorbidities, virulence of causative organisms, as well as promptness of and responsiveness to therapy.33
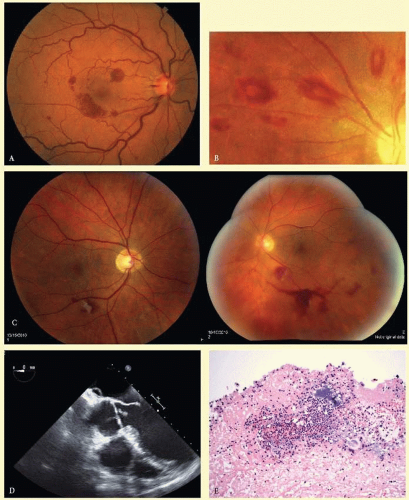 FIG. 22.1 A: Roth spot in endocarditis. Note a Roth spot (white-centered hemorrhage) superonasal to the macula. There are associated intraretinal hemorrhages as well. (Photo from Retina Service of Wills Eye Institute Photo collection.) B: More extensive and prominent Roth spots. (Photo from Retina Service of Wills Eye Institute Photo collection.) C: A 61-year-old man presented with a floater in the left eye. On examination, he had a Roth spot in each eye, with a vitreous hemorrhage in the left eye (unrelated). D: The patient had an audible aortic valve murmur. An infected valve was visible on transthoracic echography. E: Microbiology of the valve demonstrates bacteria, which were strep viridians on culture. (C-E courtesy of Alok Bansal, MD.)
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|