18
Obliteration Operations
Mastoid obliteration has evolved throughout a century of surgical development. Various materials and techniques have been described. Without methods used today, a packed mastoid wound would take 3 weeks to several months to heal. This was then followed by the chronic, troublesome, open mastoid cavity.
Ideally, a postoperative mastoidectomy will undergo prompt, complete coverage with a continuous sheet of healthy keratinized squamous epithelium. Factors that prevent this from occurring include creation of a large mastoid cavity, small sclerotic cavities, small meatuses, postoperative infection, inadequate lowering of the posterior buttress, and inadequate clearance of disease.1, 2 Attempts to control these factors by changing operative technique still fail to fully eradicate the troublesome open cavity. Ten to 60% of patients undergoing a mastoidectomy continue to experience chronic irritation.3–5
The troublesome open cavity can be managed by conservative toilet, revision open surgery, or a mastoid elimination procedure. There are three forms of mastoid elimination: ablation, obliteration, and staged reconstruction. The technique chosen depends on the patient’s symptoms, the pathology present, the patient’s hearing status, and patient compliance.
■ Indications for Mastoid Obliteration
The open mastoid cavity can cause chronic irritation for the patient. The result of open technique surgery (no preservation of the posterior canal wall) can result in a non-self-cleaning and nonwaterpro of cavity. The patient may experience one or more of the D’s: dizziness, deafness, discharge, debris, discomfort (need to maintain a dry ear), dependency on the otologist to clean the cavity, and desperation to be free of the problem.6Secondary to this, the patient is forced to curtail more pleasurable physical or social activities, such as swimming. In such conditions, there is ample indication for surgically addressing the patient’s mastoid.
■ Contraindications to Mastoid Elimination
Contraindications to a mastoid elimination procedure include an unreliable patient, general debility of the patient, it being the only hearing ear, and residual disease such as inaccessible cholesteatoma, malignancy, and infection. Appropriate management for these patients includes revision mastoidectomy or conservative toilet.
■ Principles of Elimination Procedures
Elimination procedures employ one of three philosophies (Fig. 18–1A–C). Obliteration involves a filling in of the cavity with one of three methods: (1) a pedicled flap, (2) free grafts or alloplastic materials, or (3) free grafts or alloplastic materials that are covered with a flap or graft. External canal wall reconstruction/staged reconstruction entails reconstruction of the tympanic membrane, external canal, and ossicular chain. Complete middle ear ablation, with closure of the external auditory canal (EAC), is the most radical of the three elimination procedures.
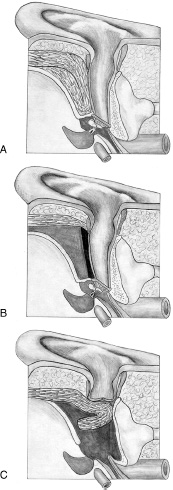
FIGURE 18–1 Three methods of obliteration. (A) Obliteration, or filling the mastoid cavity. (B) Reconstruction of the external canal wall. (C) Ablation of the middle ear and closure of the external auditory canal.
■ Technique Selection
There are multiple options for management of the troublesome open cavity. Conservative toilet is unlikely to cure the problem permanently but should be used in patients who cannot undergo surgery for various reasons. Revision open surgery should be reserved for patients in whom elimination surgery is contra-indicated.
Ablation is indicated when the affected ear has no sensorineural reserves. The contralateral ear should be disease free and have better hearing. It may also be indicated for patients unable to cooperate with postoperative care (e.g., severe mental retardation). Other indications include desire to optimize healing as in cases of exposure to postoperative irradiation or cochlear implantation. When prior procedures have been unsuccessful and the patient continues to demonstrate severe middle ear disease and an associated dermatitis of the ear canal and auricle, ablation may be entertained. The opposite ear must have normal hearing in this case. Should hearing loss in the better-hearing ear occur, a bone conduction hearing aid can then be used in the ablated ear. All ablation cases should be reexplored 12 months later to exclude residual cholesteatoma.
Obliteration is reserved for patients with hearing but who are not suitable for staged reconstruction. More recently, partial obliteration has been encouraged, with a reexploration at a second stage for residual disease. In a series of 55 obliterations, Black found a residual cholesteatoma rate of 15%.6
Staged reconstruction should be utilized in patients who are able to hear. Reconstruction can be completed in one-or two-stage procedures, pending the findings at the first stage. These patients must be reliable for two-stage procedures.
■ Surgical Techniques
Table 18–1 considers conditions that accompany a troublesome open mastoid cavity. It also addresses each technique to address the troublesome open cavity and includes points that maximize the success of these procedures.
Problem |
| Prevention/Treatment |
|---|---|---|
Persistent mastoid cavity drainage and profuse debris | Mastoid elimination | |
Recurrent cholesteatoma | Reexploration or follow-up radiographic studies 1 year after mastoid obliteration; a 15% rate of residual cholesteatoma exists | |
Mastoid obliteration | Use of hydroxyapatite filler combined with a pedicled vascular flap is advocated Use of free soft tissue is unpredictable, with varying rates of resorption and risk of infection | |
Ear canal reconstruction | Use of a hydroxyapatite prosthesis and a pedicled medial temporalis flap is advocated Vigilance must be maintained to protect against neo-external auditory canal stenosis | |
Mastoid ablation | Must be reexplored to guard against residual cholesteatoma |
Obliteration
Cavity obliteration was the first elimination procedure to appear. Two forms of obliteration exist: the flap and the filler method. The methods can be combined.
Flaps
Flaps entail the rotation of a vascularized local soft tissue flap into the open cavity defect. They require an axial blood supply and minimal muscle (risk of atrophy). A variety of muscle mesodermal tissue flaps have been developed since the early 1900s.2,7–13 The flaps most popularized are the Popper (1935) and Palva (1957) flaps.3,14,15
The Popper flap is a periosteal flap based on the pinna that extends posteriorly over the mastoid. It is rotated medially to obliterate much of the mastoid tip and cavity bowel. The Palva flap modified the Popper flap by incorporating more postaural subcutaneous tissue for better obliteration (Fig. 18–2A–C). A wing flap, developed by Black (1998), has proven successful by providing a more precise cover for the elimination site.6,–16 It is an anteroinferiorly based flap that is turned medially into the cavity. Its vascular supply is from the postauricular and middle temporal arteries. Bulk may be supplied by the posterior temporalis muscle and its overlying fascia.
Palva et al noted 50% resorption of the flap when used alone for obliteration in a series of 189 operations followed postoperatively for 4 to 7 years.17 The authors found cholesteatoma in 4% of these ears. Epithelial debris and cerumen easily cured with cleaning of the canal was found in 12%. These findings are supported by other authors.2,18–22 Flaps used alone for obliteration techniques decreased in popularity in the 1960s secondary to shrinkage and debris accumulation.
Fillers
Fillers should be durable, biocompatible, infection resistant, readily available, simple to use, and without cross-infection risk. Free grafts and other materials have been studied since the late nineteenth century for obliteration purposes.
Soft tissue, including blood clot,23–26 fat,27–29 and muscle,11,24,30–32 was proven inadequate as a filler. Blood as a filler was prone to leave residual air cells as fibrotic changes occurred. Free fat grafts require a clean cavity; if infection occurs, the fat is extruded and subsequently replaced by fibrous tissue small in bulk. Muscle has a tendency to undergo avascular necrosis or atrophy and later resorption resulting in a large cavity defect. Hohmann’s histologic studies on muscle and fat graft obliteration in mastoid cavities in the primate supported these findings.33 Muscle in the long term atrophied, producing cystic spaces. Fat was absorbed or liquefied by fat necrosis, not replaced by fibrous tissue. Its survival was unpredictable, and Hohmann states that a second surgical procedure to obtain a free fat graft is not justified.
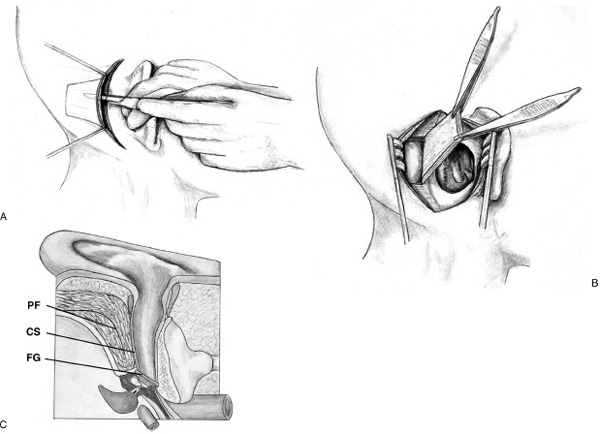
FIGURE 18-2 The Palva flap. A musculoperiosteal flap based on the pinna that extends posteriorly over the mastoid. (A) Extended elevation of the posticular flap. (B) Rotation of flap into the mastoid cavity. (C) Rotation of the flap medially to obliterate the mastoid tip and cavity bowl. CS, canal skin; FG, fascial graft; PF, Palva flap.
Fascia and periosteum soft tissue grafts remain frequently used to promote reepithelialization by lining the open cavity or covering other forms of filler used for obliteration.
Homograft and heterograft bone have been utilized as filler for mastoid obliteration. Sources include despeciated calf bone paste,1 calf bone,34 and cortical
and cancellous femoral head bone.35, 36 Heterogeneous bone (calf) only worked satisfactorily in covering small surfaces because it absorbs and is replaced by the body in a short time. Calf bone paste demonstrated early absorption as well. Merifield’s studies of homograft and heterograft bone in animals demonstrated greater than 30% absorption.29 Hohmann’s studies of heterogeneous bone as a filler in the mastoid cortex demonstrated that it became easily infected and subsequently extruded from the cavity. Foreign body and local allergic reactions were observed as well.33 Shea et al, using cancellous femoral bone chips combined with autogenous bone paste for smoothing the contour of the ear canal, demonstrated a low rate of extrusion and an ability to reduce the cavity size 60 to 100%. One year from surgery, the average increase in cavity size was 6.5%.36
Results have tended to fare better with autogenous bone. Guilford et al abandoned use of autogenous bone chips from the mastoid cortex after noting foreign body behavior and inert, nonincorporated bone in second-stage procedures.1, 11 Schiller’s “mastoid osteoplasty” utilized iliac crest autogenous cancellous bone strips for extensive obliteration of the mastoid cavity.37 Contrary to Guilford et al, Schiller noted replacement of bone grafts by new bone, provided placement in a vascularized bed. Among 40 patients followed for 9 months postoperatively, five demonstrated irregularity and enlargement of the ear canal, one demonstrated incomplete obliteration, one became infected, and one showed sequestration and subsequent avascular necrosis of the grafts. Iliac crest harvesting also results in additional donor site pain. More recently, autograft bone pate has been widely used, often in varying combinations with other fillers.35,36,38,39 It is produced in more adequate amounts and performs better than nonautologous bone. Black has demonstrated, however, that bone pate, carries with it a high rate of postoperative infections (15%), localized resorption (17%), and pocket formation (25%).6
Autologous cartilage has proven successful as a filler.40–42 It can be difficult to obtain in adequate amounts, however, without causing significant donor site morbidity (e.g., obtaining costal cartilage). Homo-graft and heterograft cartilage has shown unpredictable resorption if not supported by well-vascularized surrounding or overlying soft tissues.29 Variations of homograft and heterograft cartilage have included diced bovine cartilage filler,11 homograft chips,9 sheets of homograft cartilage,42 and crushed cartilage.43
Historically, synthetic agents such as cements to include methyl methacrylate44, 45 and ionomer cement,6, 46 silicone,47 and Proplast (Vitek, Houston, Texas)48, 49
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


