6
Risks and Complications of Tympanoplasty
The goals of tympanoplasty are to establish a safe and dry ear that is relatively trouble-free, and it is hoped, to restore middle ear function and hearing. In tympanoplasty, surgery is often necessary to deal with anatomical variations of the ear canal, ossicular chain erosion, infection, and cholesteatoma. In revision surgery, one may also have to deal with the lack of reconstructive materials, fascia, disruption of the tympanic annulus, exposure of the temporomandibular joint, and middle ear fibrosis.
■ Preoperative Evaluation, Risk Identification, and Management
The recognition of potential complications in tympanoplasty begins with the initial evaluation and plans for surgery. Table 6–1 summarizes potential problems that may arise with tympanoplasty and possible solutions. The preoperative evaluation begins with a detailed history of infections, drainage, hearing loss, vertigo, and previous surgery, as well as a careful microscopic evaluation of the ear, will identify many potential problems. With a draining ear, cultures should be obtained with consideration for antibiotic treatment.
Microscopic examination of the ear is useful to determine the extent of the perforation and the condition of the remaining drum, middle ear, and ossicular chain. It is also useful in the evaluation of squamous epithelium ingrowth into the middle ear and around the margin of the perforation, and its extent onto the medial surface of the drum. The small perforation with a large surrounding whitish area may require much more extensive surgery than suggested based on the perforation size alone. Squamous epithelium, cholesteatoma, appears as a whitish thickening of the eardrum extending from the perforation. This appears similar to tympanosclerosis but not as thick. Tympanosclerosis adjacent to a perforation may conceal cholesteatoma on the medial aspect of the drum. In addition, this avascular tissue may complicate the healing process.
The ossicular chain is also often seen through the translucent tympanic membrane. On microscopic examination it may be possible to identify remnants of the incus or stapes, which would affect middle ear reconstruction for hearing. Cerumen or crust in the ear canal may conceal a retraction pocket or cholesteatoma. The condition of the middle ear mucosa is assessed with regard to the degree of inflammation. The middle ear mucosa as well as a history of infections and examination of the opposite ear would provide some insight into the eustachian tube function.1
Preoperative treatment begins with initial consultation. Controlling middle ear infection and establishing a dry middle ear, with healthy mucosa, reduces the potential for infection, which is associated with 60% failures in tympanoplasty.2 An antibiotic pack is placed in the ear and antibiotic drops applied directly to the packing for 1 to 2 weeks, not directly to the ear or perforation. After removing the packing, the patient is asked to dry the ear using a hairdryer on a cool setting for 3 to 5 minutes twice daily; a disposable ear speculum may be used as a funnel to direct the air into the ear canal. The ear is periodically cleaned and dusted with boric acid powder once or twice a week, depending on the amount of drainage. If there is significant infection, the ear is inspected at 1- to 3-week intervals until dry, and the mucosa returns to normal, which is usually within a 4- to 6-week period. The ear can be maintained with less frequent treatments until surgery is performed.3
| Problem | Prevention/Treatment | |
|---|---|---|
| Canaloplasty | ||
| Facial nerve | Facial nerve monitoring Stimulation of all unrecognized soft tissue structures during drilling | |
| Anterior canal wall/temporomandibular joint penetration | Bipolar cautery of prolapsed fat | |
| Cartilage or bone graft of bony defect and packing of ear canal for 4-6 weeks | ||
| Exposed mastoid air cells Postoperative canal stenosis | cover the exposed air cells with bone pate, paste, fascia, and skin flaps Removal of spine of Henle Removal of anterior meatal spine Endaural relaxing incision through incisura terminalis Prolonged packing of ear canal | |
| Tympanoplasty: underlay | ||
| Middle ear cholesteatoma | Ensure the removal of all squamous epithelium from middle ear drum preparation | |
| Graft separation | Ensure good approximation between drum remnant and graft with adequate gelatin foam | |
| Graft failure in anterior drum | Prevent by considering sandwich or overlay technique Tight packing of eustachian tube with gelatin foam | |
| Tympanoplasty: Overlay | ||
| Anterior blunting | Coverage of the anterior canal bone Tight packing of anterior canal with gelatin foam | |
| Graft lateralization | Placement of graft medial to malleus handle Placement of fascia against posterior annular rim | |
| Drum cholesteatoma | Meticulous removal of all squamous epithelium on lateral tympanic membrane | |
| Sandwich | ||
| Anterior blunting | Skin coverage of the anterior canal bone Tight packing of anterior canal with gelatin foam | |
| Drum cholesteatoma | Meticulous removal of all squamous epithelium on lateral tympanic membrane |
An audiogram is obtained at the initial visit and confirmed with a second examination prior to surgery. The Weber and Rinne tests using the 512 Hz and 1024 Hz tuning forks are used to confirm a conductive hearing loss.
Preoperative visits are also used to answer the patient’s questions about surgery, risks of surgery, including graft failure, recurrent perforation, hearing results, vertigo, facial paralysis, and infection. In addition, other potential problems and risk factors such as smoking, nasal and allergic problems, medical disorders, and use of anticoagulants and other medications, are discussed with the patient.4 Preferably those medications that may contribute to bleeding are stopped at least 2 weeks prior to surgery to reduce intraoperative bleeding, which may adversely affect exposure, graft placement, or ossicular chain reconstruction.
■ Intraoperative Risk Prevention and Management
Adequate exposure is essential for precise reconstruction of the drum and ossicular chain. The surgeon should be able to visualize the margins of the perforation at the time of reconstruction.
The most common approach in tympanoplasty is using the postauricular incision, which allows better exposure of the anterior annulus and middle ear. The postauricular incision is preferred for anterior and total perforations. Using the postauricular incision, areolar or true fascia is harvested from the posterior temporalis muscle. In revision surgery, it may be necessary to harvest fascia from the anterior temporalis muscle or from the occipital cortex. After multiple procedures, temporalis fascia may not be available and it becomes necessary to harvest pericranium from the medial aspect of the temporalis muscle or fascia from the opposite ear.5
Small central perforations with clear margins without squamous epithelial ingrowth can be managed using a transmeatal approach with an ear speculum. However, it may not be possible to obtain sufficient exposure for repair of large perforations through an ear speculum. Use caution with a small posterior perforation. Cholesteatoma, which appears white through the drum may extend anterior on the medial surface of the drum as far as the eustachian tube. This frequently requires reconstruction of the entire tympanic membrane.
With the endaural incision, the pinna is retracted posteriorly, which permits better exposure of the posterior middle ear and ossicular chain. In revision surgery, the endaural incision allows better exposure of the anterior temporalis muscle fascia.3
Canaloplasty
Canaloplasty with enlarging and straightening of the bony ear canal permits exposure of the entire drum surface. Straightening the anterior canal wall and floor of the external auditory canal reduces the potential of blunting in the anterior tympanomeatal angle by shifting the angle away from the tympanic annulus. Removal of the posterior annular rim facilitates exposure of the posterior middle ear and ossicular chain. It also reduces the potential for fixation of the ossicular prosthesis to the canal wall (Fig. 6–1A–D).5, 6
One of the biggest dangers during canaloplasty is the loss of canal skin or the tympanomeatal flap, which may inadvertently become wrapped around the drill bur. This problem can be reduced by removing the tympanomeatal flap and epithelium from the lateral drum surface prior to performing the canaloplasty. The canal skin can be replaced as a free skin graft after placement of the fascia graft. The risk of a torn flap is greater when it is pedicled at the annulus. A small square of instrument wipe sponge or a strip of aluminum from a suture pack will help protect the canal skin flaps, drum, and ossicular chain from the drill. A laterally based anterior canal wall flap is less susceptible to being avulsed by the drill if protected by the retractor blade. However, a laterally based flap may retract leaving the anterior tympanomeatal angle bare, which can lead to blunting of the angle. Covering the angle with skin after reconstruction of the drum will reduce blunting. This can be accomplished by advancing a free canal skin graft covering the drum several millimeters up the canal wall, or the anterior canal skin several millimeters onto the drum surface.7, 8
Failure to maintain adequate epithelial coverage of the ear canal increases the potential for postoperative canal stenosis and fibrosis of the medial canal and drum. Thin split-thickness skin grafts can be used to provide epithelial coverage of the eardrum and canal. Small grafts (0.5 xl 1 cm) can be obtained for the posterior surface of the pinna. A larger split-thickness skin graft (STSG) to resurface the ear canal and drum can be obtained from the high or lower abdomen. Although some surgeons may prefer to obtain a graft from the arm, it has been my experience that this is more irritating than other sites. Packing the ear canal following surgery for several weeks will help ensure an adequate meatus and reduce secondary canal stenosis.9
When approaching the level of the annulus, the surgeon should be aware of soft tissue in the posterior wall and floor of the canal, which could be the vertical facial nerve. Identification of the chordae tympani nerve, which can be followed to the vertical facial nerve, is often helpful.5 In congenital ear surgery, the facial nerve may cross the floor of the external auditory canal lateral to the annulus or it may form the annular rim. In children, the vertical facial nerve may be lateral to the plane of the tympanic annulus, whereas in adults, it is generally 2 to 6 mm medial to the plane of the tympanic annulus.10–14
Facial nerve monitoring is not required for tympanoplasty except in special circumstances, such as a congenital ear. However, the patient should not be given paralytic agents by anesthesia. One must remain oriented when working in the ear canal and middle ear with regard to the normal location of the facial nerve. If there is question about an unusual soft tissue structure, it is better to test for facial stimulation. If evoked electromyographic monitoring of the patient’s facial nerve is not available, a hand gently resting on the nonparalyzed patient’s cheek is equally as sensitive to facial movement as electrical monitoring.
Penetration into the temporomandibular joint during canaloplasty can cause intraoperative and postoperative problems, particularly if the periosteum is violated. If the periosteum is violated, fat prolapsing into the external auditory canal may impair exposure of the anterior drum. A bipolar cautery may be used to transect the fat, causing the fat to retract into the temporomandibular joint (Fig. 6–1E). In most cases, packing of the ear canal for 4 to 6 weeks postoperatively, until fibrosis and epithelialization are complete, will prevent significant soft tissue prolapse from developing. If a large defect is created, a thin layer of bone or cartilage placed anterior to the canal wall and covered with fascia will reduce problems with prolapse of the soft tissue into the canal (Fig. 6–1F). In severe cases of prolapse of the temporomandibular joint, the patient may develop fullness in the ear, cerumen impaction medial to the prolapsed tissue, and occasionally temporomandibular joint pain.
In block resection of the external auditory canal for carcinoma, the anterior canal wall is commonly resected with no significant postoperative problems. In congenital ear surgery, the periosteum of the temporomandibular joint is frequently “skeletonized” without problems. Postoperative packing of the external auditory canal for 6 to 8 weeks in both cases reduces potential stenosis of the canal.16
Exposure of mastoid air cells during canaloplasty may result in mucosa developing within the external auditory canal leading to a moist ear, infection, the accumulation of squamous debris, and cholesteatoma formation. Covering exposed air cells with bone pate (paste), fascia, and skin flaps will frequently prevent these problems from developing (Fig. 6–1F).16
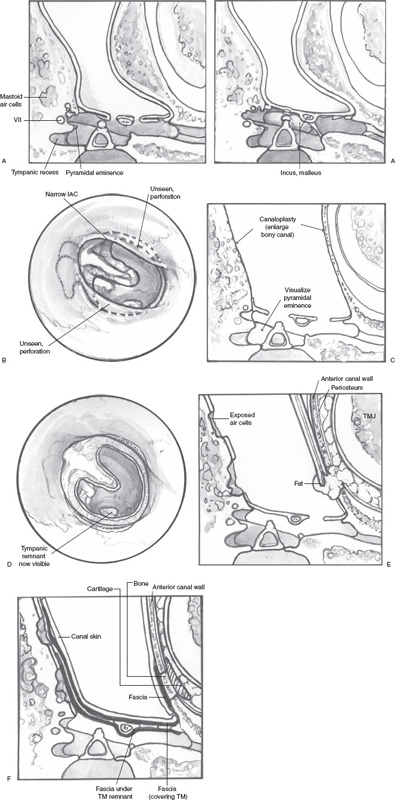
FIGURE 6–1 (A) Canaloplasty. A narrowed ear canal can be caused by a prominent bulge in the anterior canal wall or floor of the external canal, and may limit exposure of tympanic membrane perforation and annular rim. (This would include specific causes, such as exostosis.) (B
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


