23
Rarer Tumors of the Middle Ear and Temporal Bone
The temporal bone is a structure with intricate anatomy and important function. Within it lie the mechanical and neurological mechanisms of hearing, balance, facial sensation and movement, swallowing, and speech. The temporal bone can be divided into anatomical regions of the middle ear, mastoid, external auditory canal (EAC), otic capsule, petrous apex, jugular fossa, and internal auditory canal (IAC). Tumors of the temporal bone are uncommon. They manifest in several ways, depending on the location and involvement with neurovascular structures. A discussion of temporal bone tumors can be made specific to the region of involvement because each region has unique tumor types, clinical presentations, exam findings, and surgical approaches (Fig. 23)On the other hand, it is common for tumor to involve overlapping anatomical regions, so that no area can be considered in isolation, and a broad understanding of the temporal bone and all of its intricacies is vital.
■ Anatomy and Pattern of Spread
One might assume that tumor extension within the temporal bone would be difficult to predict, given the complex structure of the temporal bone with bony framework, preformed pathways, and soft tissue structures that extend across anatomical boundaries. However, armed with an understanding of the anatomy of the ear and tumor behavior, pathways of tumor extension are predictable. Skin and cartilage of the EAC offer little resistance to spread of tumors originating in the EAC or from the skin of the auricle. In the EAC, Santorini’s fissures, Huschke’s foramen, and the bony-cartilaginous junction provide direct access to the periparotid tissues and temporomandibular joint (TMJ). The bony canal is resistant to tumor extension, but erosion of the canal wall provides communication between the EAC and the mastoid cavity. Erosive extension through the tympanic ring allows tumor to spread between the middle ear and EAC. In the middle ear, the hard bone of the otic capsule blocks medial tumor extension; however, the eustachian tube, round and oval windows, neurovascular structures, and mastoid cavity are preformed pathways for tumor growth. From the middle ear, tumor can spread anteriorly along the eustachian tube to the nasopharynx and infratemporal fossa or along the promontory or caroticotympanic nerve to the carotid artery. Posteriorly, middle ear tumors extend directly or along the facial nerve into the mastoid. Aggressive mastoid tumors can erode into the middle or posterior fossa and involve the sigmoid sinus and dura. The dura is somewhat resistant to invasion, but eventual intracranial involvement ensues. The facial nerve, trigeminal nerve, greater superficial petrosal nerve, and carotid artery are common routes for direct tumor extension throughout the temporal bone and into surrounding anatomical areas, including the intradural space, cavernous sinus, jugular bulb, infratemporal fossa, periparotid tissues, and neck.
■ Warning Signs
When evaluating patients in an otologic clinic, a complete history and physical includes evaluation of the ear, head and neck, and cranial nerves. Tumors of the ear and temporal bone are uncommon, but vigilance for detecting them should always be high. These warning signs should lead to a careful consideration of the possibility of temporal bone lesions (Table 23–1). Table 23–2 presents some points of consideration when faced with a temporal bone lesion.
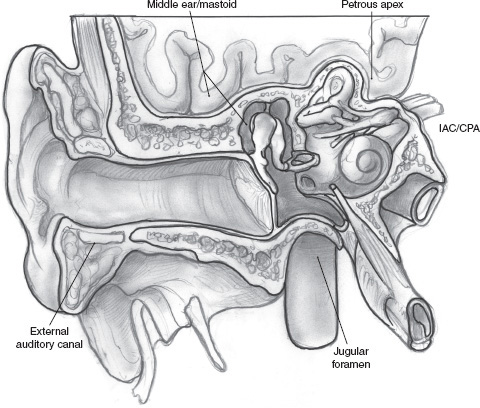
FIGURE 23-1 Anatomy of the ear and temporal bone. CPA, cerebellopontine angle; IAC, internal auditory canal.
■ Radiographic Evaluation
Any warning sign warrants further evaluation with radiographic imaging. Computed tomography (CT) and magnetic resonance imaging (MRI) offer distinct advantages over one another; both may be needed to make a diagnosis and plan intervention. The history and physical can be a guide in choosing the optimal initial study. For instance, if symptoms and physical findings suggest a lesion of the middle ear or mastoid, petrous apex, jugular bulb, or EAC, a high-resolution CT scan with 1 mm sections in the axial and direct coronal planes offers advantages of showing bone erosion and extent of soft tissue disease. In many cases of middle ear and EAC lesions, a CT is the only examination required for diagnosis and surgical planning. A CT scan is performed preoperatively even if a middle ear mass is small and its borders are visualized completely; it is important to document an intact bony cover over the carotid artery and jugular bulb, thereby ruling out a carotid anomaly and a glomus jugulare.
MRI is helpful when the extent of tumor or the type of tumor is not clear based on CT, such as larger tumors of the middle ear, petrous apex, or jugular bulb. MRI provides additional information on subtle extension of tumor along tissue planes and helps differentiate soft tissue from fluid within the middle ear and mastoid.1 MRI can also demonstrate dural and intradural involvement.
Findings suggestive of a lesion in the cerebellopontine angle (CPA) or IAC and isolated facial nerve paresis are best evaluated first with gadolinium-enhanced MRI. To evaluate the facial nerve, MRI includes the CPA, brainstem, skull base, and parotid, to detail the entire course of the facial nerve from its nucleus to its entry into the parotid gland. Bone algorithm CT scan demonstrates the bony detail of the geniculate, labyrinthine, tympanic, and mastoid segments of the facial nerve, as well as the stylomastoid foramen.
Angiography is needed for large vascular tumors prior to surgery to assess carotid involvement and document collateral flow. Occlusion studies such as single photon emission computed tomography (SPECT) scan are done when there is a chance of carotid sacrifice. We do not recommend carotid sacrifice for benign disease because the risk of stroke is 10% even in cases with favorable occlusion studies. Larger glomus tumors are embolized prior to surgery to reduce intraoperative blood loss.
Radiographic evaluation must be done with optimal technique. For CT, axial and coronal thin cut sections 1 or 1.5 mm are obligatory. Reconstructed coronal images are inadequate to detail the diameter or erosion of the geniculate ganglion or the tympanic portion of the facial nerve, and direct coronal images should be obtained. When evaluating the ear, MRI scans limited to the brain or done without contrast are inadequate. The MRI includes coronal and axial, T1- and T2-weighted images, gadolinium, and fat suppression. Other techniques are introduced as appropriate by the radiologist. The surgeon must always examine the studies personally for technique and findings.
Facial paresis |
Recurrent ipsilateral facial paralysis—In Mark May’s1A series of 1862 patients with Bell’s palsy, facial paralysis recurred in 13%, with 38% of those ipsilateral, accounting for 5% of the total group; in 197 patients with facial nerve tumors, the incidence of recurrent paralysis was 10% |
Slowly progressive facial paralysis (over weeks to months) |
A Bell’s palsy that does not begin recovery within 6 months |
Facial paralysis accompanied by twitching or hemifacial spasm |
Involvement of single or multiple facial nerve branches with sparing of others |
ENoG of > 95% degeneration within the first 5 days of facial paralysis |
Prolonged latency as well as decreased amplitude on ENoG (Bell’s palsy will have decreased amplitude but normal latency) |
On EMG, fibrillations and polyphasic potentials indicate simultaneous degeneration and regeneration, suggestive of a tumor |
A lesion in the IAC associated with facial paralysis is probably not a vestibular schwannoma and is more likely a hemangioma or neuroma |
Chronic otorrhea (duration in the order of years) |
Bleeding from the ear |
A polyp in the EAC or middle ear, especially if hemorrhagic or necrotic |
Middle ear mass not consistent with cholesteatoma, such as fleshy, gray, or purple color, or granular consistency |
Otalgia—persistent or out of proportion to physical findings |
Parotid mass |
Facial numbness or pain |
History of skin cancer of the face, ear, or scalp |
History of malignancy (breast, colon, prostate, parotid, lung) |
Multiple cranial nerve deficits |
ENoG, electroneuronography; EAC, external auditory canal; EMG, electromyography; IAC, internal auditory canal
■ Other Considerations
When encountering unusual tumors of the temporal bone, a team approach is critical. Consultation with a radiologist, pathologist, neurosurgeon, and reconstructive surgeon experienced in disorders of the temporal bone improves quality of care. We regularly present unusual or complicated cases to a tumor board, which includes discussion with a radiologist, pathologist, radiation oncologist, and medical oncologist, in addition to input from the medical staff of the hospital.
Intraoperative neurophysiological monitoring of cranial nerves VII, VIII, IX, and X can decrease postoperative neural deficits. Operating room personnel and the surgeon must be experienced in the setup, interpretation, and trouble shooting of the tests. Muscle relaxants are avoided during monitoring of motor nerves. The equipment should be high quality and reliable and placed distant to sources of electrical interference.
■ Middle Ear/Mastoid
Tumors of the middle ear and mastoid are uncommon. The middle ear and mastoid contain embryological derivatives of ectoderm, mesoderm, and endoderm and therefore hold the risk of developing a variety of tumors, including epithelial, vascular, bone, cartilaginous, and neural tumors. By far the most common tumors are paraganglioma (glomus tumors). Facial nerve neuroma is probably the second most common in frequency, but is rare. Other rare benign tumors of the middle ear include adenoma, schwannoma, hemangioma, meningioma, dermoid, teratoma, lipoma, osteoma, and papilloma. Malignant tumors include squamous cell carcinoma, ceruminous adenocarcinoma, adenocarcinoma, rhabdomyosarcoma (Fig. 23–2A), osteosarcoma, lymphoma, chondrosarcoma, carcinoid-tumor, hemangiopericytoma, and melanoma. Tumor-like lesions include heterotopic salivary gland (choristoma), encephalocele, and granulomatous disease. A high dehiscent jugular bulb or an aberrant carotid artery may give a false impression of a middle ear mass. Primary tumors of the mastoid are rare. One that deserves special mention is the endolymphatic sac tumor, which occurs sporadically or associated with von Hippel-Lindau disease (Fig. 23–2B).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


