Fig. 866 The Rambo obliteration method in an endaural approach. The vertical incision extends up to the upper edge of the auricle, and the intercartilaginous incision runs medially to Shrapnell’s membrane. A lateral circumferential and a medial circumferential incision connect the intercartilaginous incision. At the 5-o’clock position, a radial incision is made. Around the annulus, the skin is incised to remove the squamous epithelium from the drum. The posterior meatal skin is removed. It will be replaced at the end of the operation
Superiorly Based Flaps
The superiorly-based flaps usually consist of the temporal muscle, elevated together with the periosteum and the temporalis muscle fascia, and they are turned down into the cavity. Such flaps are usually sufficient to obliterate the upper part of the cavity. Flaps consisting partly or mostly of retroauricular subcutaneous fibrous tissue and muscle with its periosteum can be superiorly based, and several obliteration techniques have been described in endaural and retroauricular approaches.
In the early 1930s, Mill (1931) and Kisch (1932) used a temporal muscle flap in an attempt to obliterate the mastoid cavity and retain an external auditory canal.
The Rambo Flap
Rambo (1957) described a method of covering the tympanic cavity and the medial antrum wall with a superoanteriorly-based flap of temporalis muscle. The aim of the flap was to bridge the tympanic cavity and restore hearing.
After a special endaural incision, extending posterosuperiorly to the upper edge of the auricle (Fig. 866), a large area of the temporalis muscle fascia is exposed. The conchal skin is elevated, creating an anterior and an inferior skin flap, and exposing the entire bony ear canal. The drum epithelium is removed (Fig. 867). A conservative radical cavity is created, with extensive removal of air cells (Fig. 868). A flap of the temporalis muscle with its fascia is cut, and it is turned down over the mastoid tegmen into the cavity to cover the drum remnant, the attic, and the medial wall of the aditus ad antrum (Fig. 869). A larger flap will cover the tympanic cavity, the attic, and the medial wall of the antrum (Fig. 870). The canal skin flaps are returned, and the free flap of canal skin is replaced, partly covering the muscle flap and partly covering the bone of the cavity (Fig. 871).
The major part of the cavity wall is not covered with muscle. Rambo never used the muscle to fill the cavity, but the muscle contributes with its vascularity to healing and is a vascular support for skin flaps. In subsequent years, Rambo detached the drum from the malleus handle and elevated it laterally together with the annulus and ear canal skin (Rambo 1969). The Rambo method was often used in fenestration operations, and rapid healing of the cavity was often the case (Fritz and Crawford 1960).
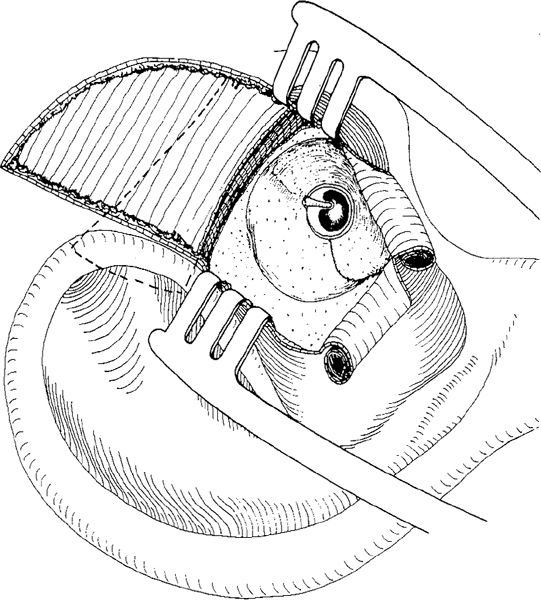
Fig. 867 The temporalis muscle fascia is exposed. The skin from the anterior and inferior parts of the ear canal is elevated as two laterally pedicled flaps. The epithelium from the drum remnant is removed. The incision in the temporalis muscle to harvest the flap is indicated by a dashed line
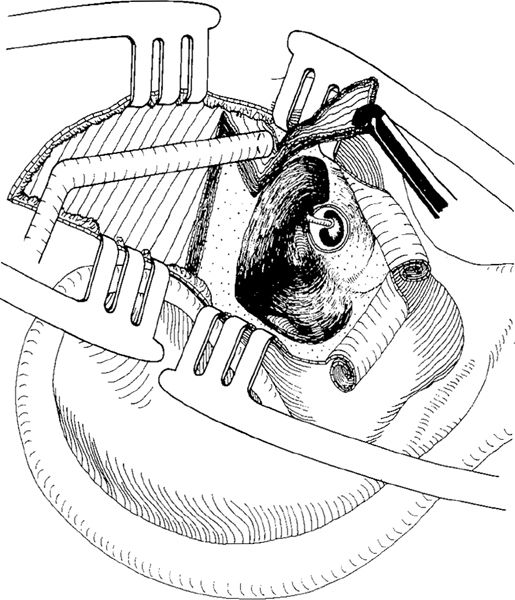
Fig. 868 A conservative radical operation with partial preservation of the bony bridge, resection of the malleus head, and extraction of the incus, is performed. An anteriorly-pedicled temporalis muscle flap is excised and pushed toward the cavity
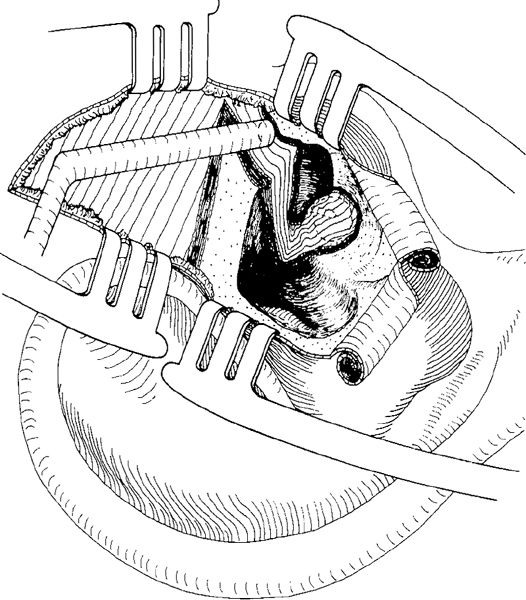
Fig. 869 The flap covers the anterior part of the mastoid tegmen, the aditus ad antrum, the attic, and the drum region
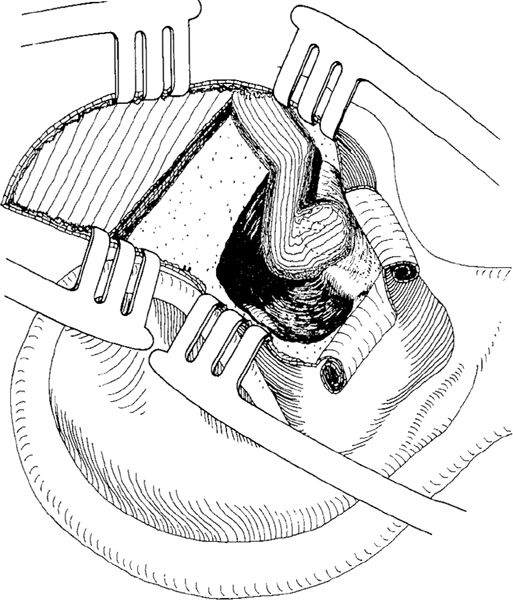
Fig. 870 A larger temporalis muscle flap is excised and placed in the antrum, aditus ad antrum, and attic, and onto the drum remnant
Thorburn (1961), on the other hand, did not cover the tympanic cavity with the muscle flap, but used it to obliterate the cavity. In an endaural approach, after elevating a large, laterally-based ear canal skin flap and after a canal wall–down mastoidectomy, Thorburn elaborated an anteriorly-based temporalis muscle flap (Fig. 872). The flap covers the superior part of the cavity (Fig. 873). The tympanic cavity is covered with a fascial prolongation placed under the skin (Fig. 874). The flaps are replaced, partly covering the muscle and partly covering the bone, and the ear canal is widened (Fig. 875).
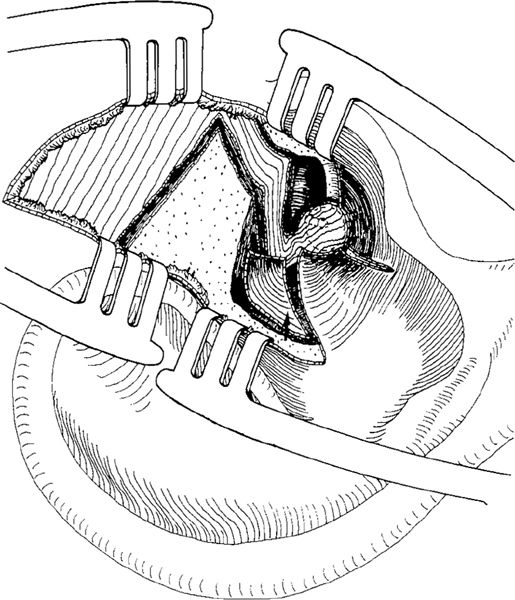
Fig. 871 The meatal skin flaps are replaced, as is the free ear canal skin flap covering part of the temporalis muscle and the cavity (arrow)
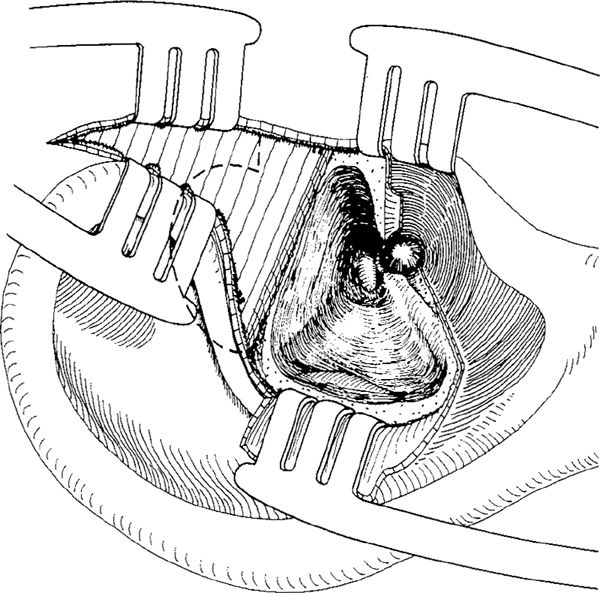
Fig. 872 The Thorburn obliteration method. An endaural approach, with a vertical incision extending to the top of the pinna and a canal wall–down mastoidectomy, is made. The ear canal skin is incised all the way around the annulus. There is no drum remnant, no malleus, and no stapes crura. The temporalis muscle fascia is exposed, and the size of the muscle flap is indicated by dashed lines
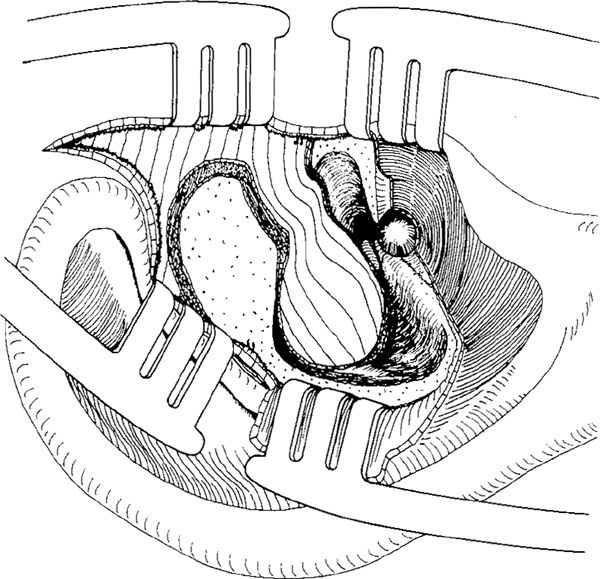
Fig. 873 A large, anteriorly-pedicled temporalis muscle flap is excised. The flap covers the superior part of the cavity, the antrum, and part of the sinodural angle
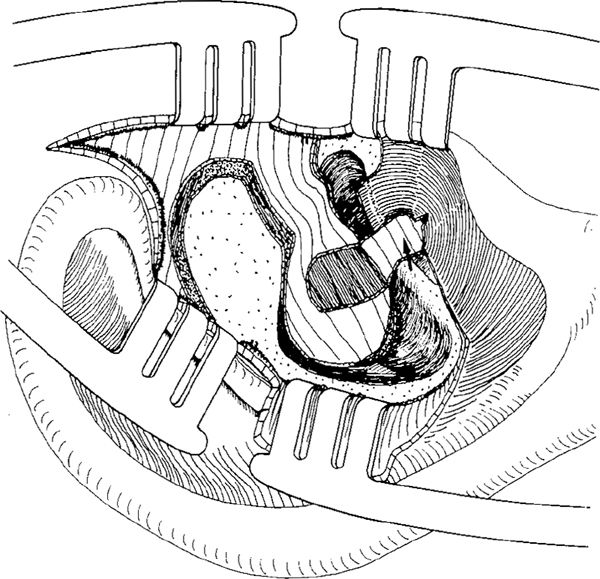
Fig. 874 From the muscle flap, a pedicled fascial graft is placed as an underlay graft under the canal skin, and the superior epithelial flap is replaced (arrow)
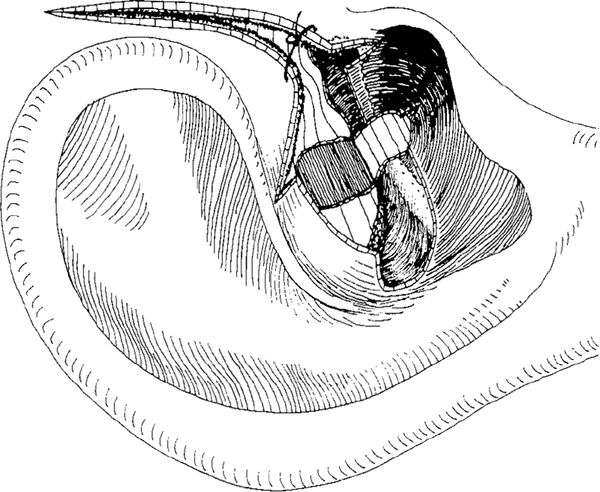
Fig. 875 The laterally-based skin flap is replaced, partly covering the muscle and partly the cavity wall. The skin incision will be sutured, maintaining a wide ear canal
The Freerichs and Williams Flap
Freerichs and Williams (1962) modified the Rambo technique in order to obliterate the mastoid cavity with temporalis muscle. After an endaural incision including a vertical extension 1 cm superior to the helix of the auricle, a laterally-based ear canal skin flap is elevated, exposing the posterior bony ear canal and the mastoid process (Fig. 876). After posterior retraction of the auricle, the temporalis muscle fascia is exposed (Fig. 877).
If only an atticotomy or a small atticoantrotomy is performed, a small muscle flap is used (Fig. 878) to cover the bony defect (Fig. 879). The perforation is closed with a free fascial graft, and the ear canal flap is returned.
If a canal wall–down mastoidectomy has been performed, then a large temporalis muscle flap with the fascia and the periosteum is elevated. The flap has a broad base anteriorly (Fig. 880). It is placed in the cavity with a broad pedicle along the mastoid tegmen.
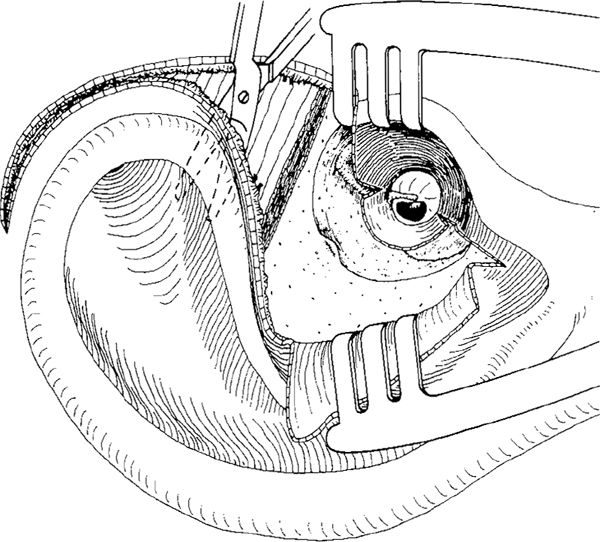
Fig. 876 The Freerichs and Williams obliteration method. An endaural approach is made, with a vertical incision extending 1 cm superior to the helix. The posterior ear canal skin is elevated laterally, making a laterally-based flap that is held aside by a selfretaining retractor The mastoid process is exposed. A medial radial incision at the 12-o’clock position, and a similar incision at the 5-o’clock position, are performed. With a pair of scissors, the auricle is elevated from the temporalis muscle fascia
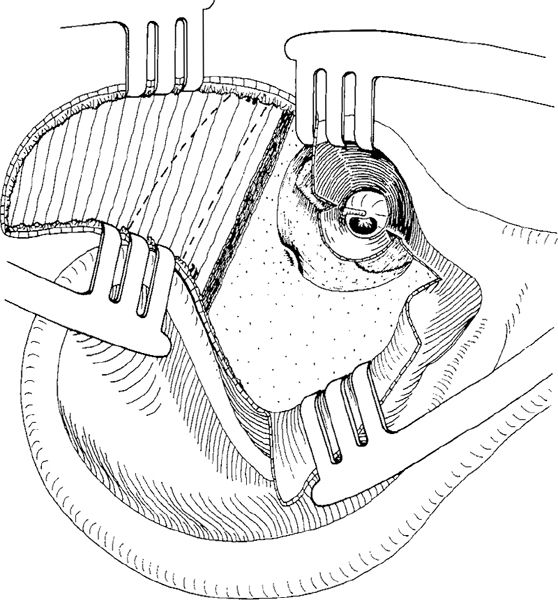
Fig. 877 The temporalis muscle fascia is exposed. A small and a large temporalis muscle flap are indicated by dashed lines
Using this type of flap, it is extremely difficult to reach the mastoid tip. Even the largest temporalis muscle flap will not reach (Fig. 881).
Another problem of large, anteriorly based temporalis muscle flaps is that their pedicles may occupy too much space in the anterior part of the mastoid tegmen, and may contribute to narrowing of the ear canal.
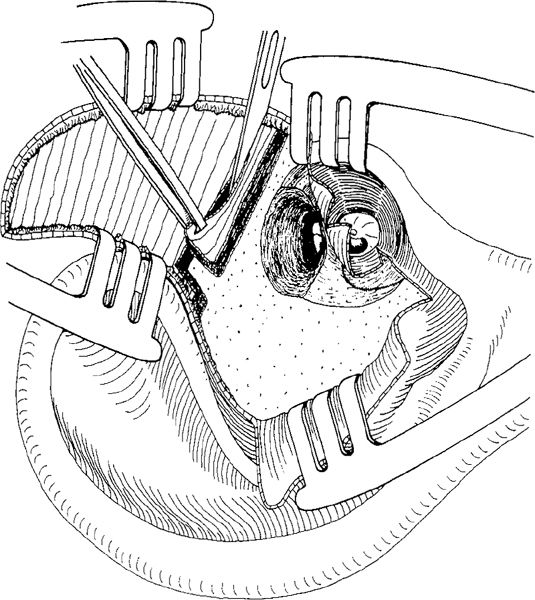
Fig. 878 An atticotomy is performed. A small, anteriorly-pedicled flap is cut from the inferior edge of the temporalis muscle
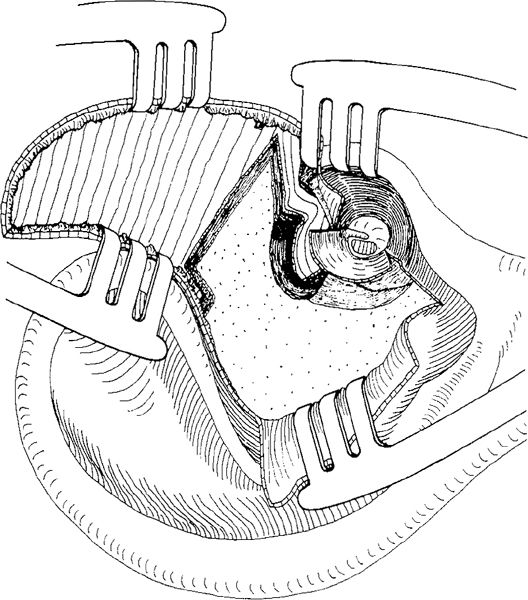
Fig. 879 The flap covers the atticotomy, and the tympanomeatal flap is replaced
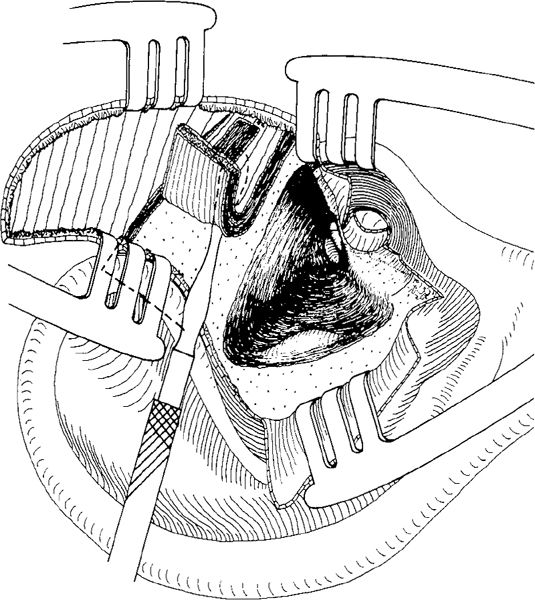
Fig. 880 A large, anteriorly-pedicled temporalis muscle flap is cut and elevated in a case of canal wall–down mastoidectomy with a preserved bridge, intact ossicular chain, and posterior perforation
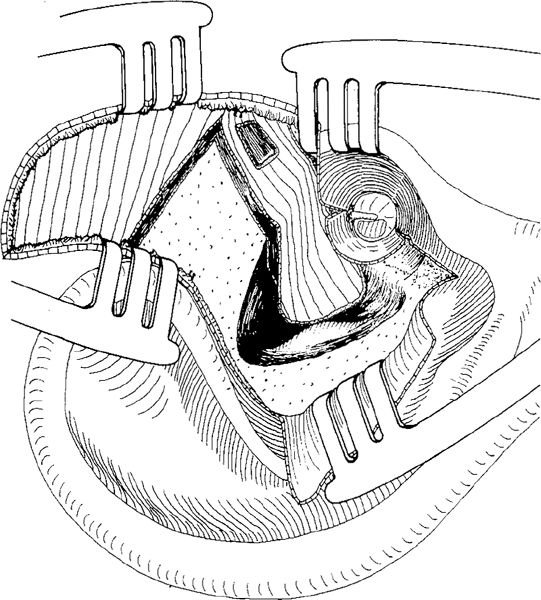
Fig. 881 The posterior perforation is closed with an underlay fascial graft taken from the temporalis muscle. A large, anteriorly-pedicled temporalis muscle flap covers the aditus ad antrum and the medial part of the cavity. The ear canal skin flaps are replaced
The Tos Bipartite Flap
Since 1962, the present author, when performing mastoid obliteration using temporalis muscle, and recognizing the difficulties of using the Rambo or Freerich flaps to reconstruct the ear canal wall or to cover both the antrum and the mastoid tip, has used a bipartite flap — one part obliterating the mastoid tip, and other the antrum (Tos 1969). The flap includes retroauricular tissue and the temporalis muscle.
A retroauricular skin incision is made 1 cm behind the retroauricular fold. The skin is elevated, and a curved incision is made through the subcutis, the posterior auricular muscle, and the periosteum, running along the entrance of the ear canal and extending toward the mastoid tip (Fig. 882). The fibrous tissue and periosteum are elevated and retracted posteriorly. This tissue will be included in the flap (Fig. 883). After the canal wall–down mastoidectomy (Fig. 884), dissection of the musculoperiosteal flap is started at the mastoid tip, including as much muscle as possible. If necessary, the attachment of the sternocleidoid muscle — but always parts of the splenius capitis muscle, transversus nuchae muscle, and longissimus capitis muscle — is included in the inferior part of the flap, which is thicker than the upper part (Fig. 885). The flap is cut and elevated in a superior direction. The retractor has to be repositioned and the skin retracted maximally in order to elevate and dissect the upper part of the flap (Fig. 886). Using a pair of scissors, the flap is cut posteriorly (Fig. 887) and as far as possible superiorly and anteriorly (Fig. 888). Finally, the base of the flap is placed in the cavity in such a way that it forms a firm “wall” in the region of the removed posterior bony ear canal wall. The inferior end of the flap is placed in the mastoid tip. In the posterosuperior part of the flap, a vertical incision is made, thus creating the posterior part of the flap (Fig. 889). This flap is turned down into the antrum and sinodural angle (Fig. 890).
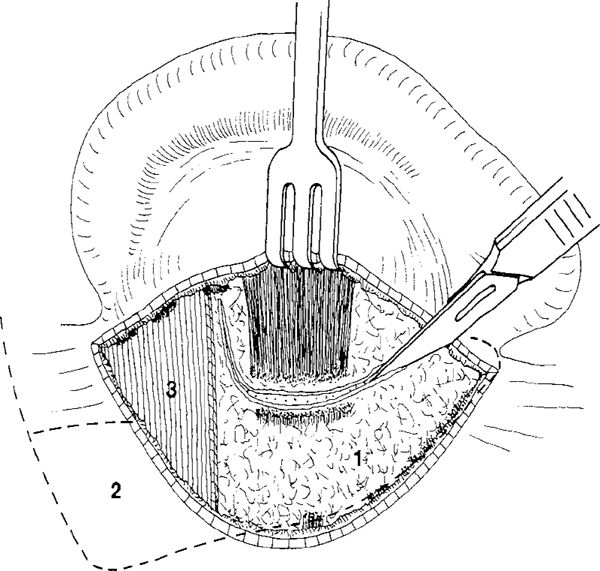
Fig. 882 The Tos obliteration method with a bipartite flap. After a retroauricular skin incision 1 cm behind the retroauricular fold, the skin is elevated. An incision through the subcutis–periosteum tissue and the posterior auricular muscle runs along the entrance of the ear canal and extends toward the mastoid tip. The size of the bipartite flap is indicated by dashed lines. (1) the inferior flap, (2) the posterior flap, (3) the base of the flap
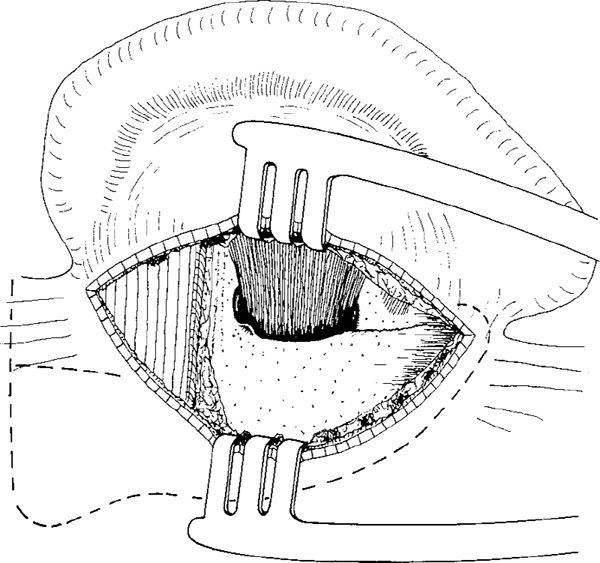
Fig. 883 The retroauricular tissue is elevated with the periosteum and retracted posteriorly, exposing the mastoid plane and the entrance of the ear canal
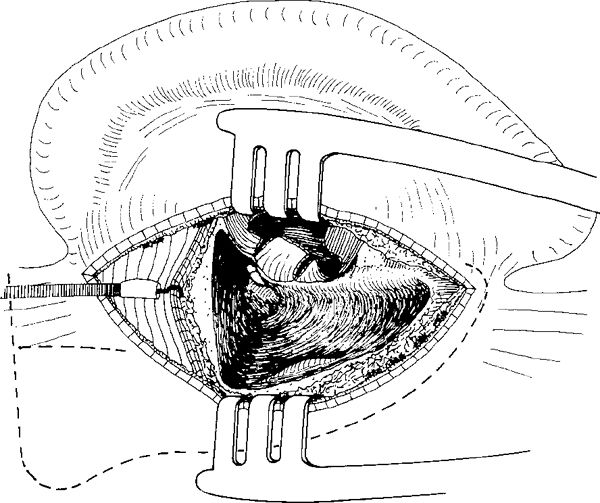
Fig. 884 The ear canal skin flaps are elevated. A canal wall–down mastoidectomy with preserved bridge is performed
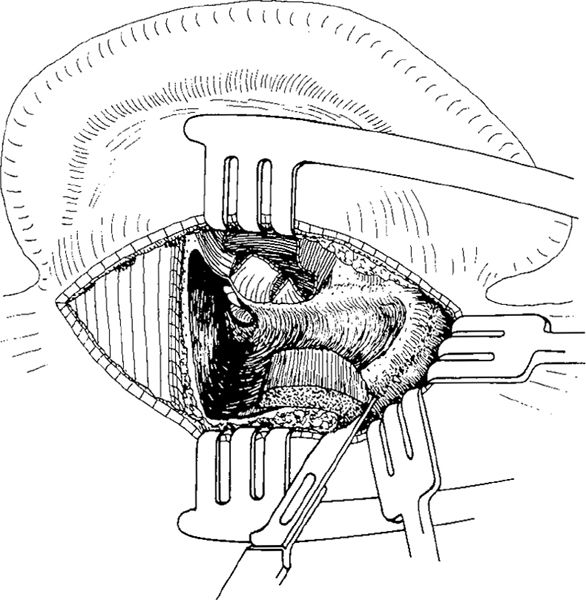
Fig. 885 Dissection of the muscle flap is started inferiorly, beyond the mastoid tip. After further retraction of the skin, the fibers of the sternocleidomastoid muscle, the splenius capitis muscle, and the transversus nuchae muscle attached to the posterior aspect of the mastoid tip are cut with a knife
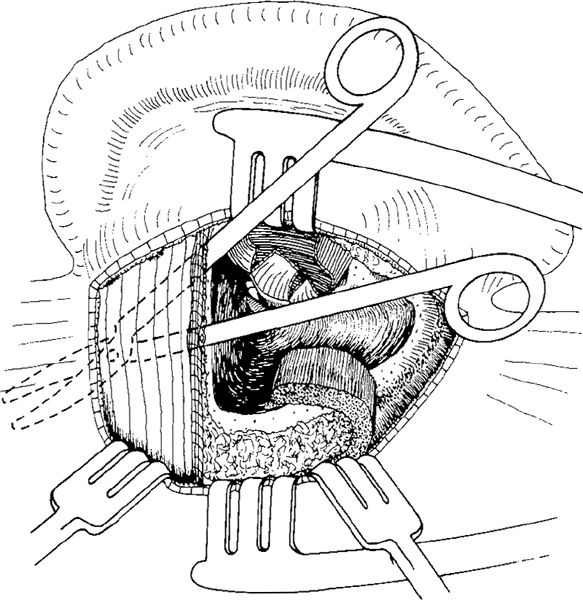
Fig. 886 After further retraction of the skin posteriorly, the fibrous tissue posterior to the cavity is exposed and, together with the temporalis muscle, detached from the bone
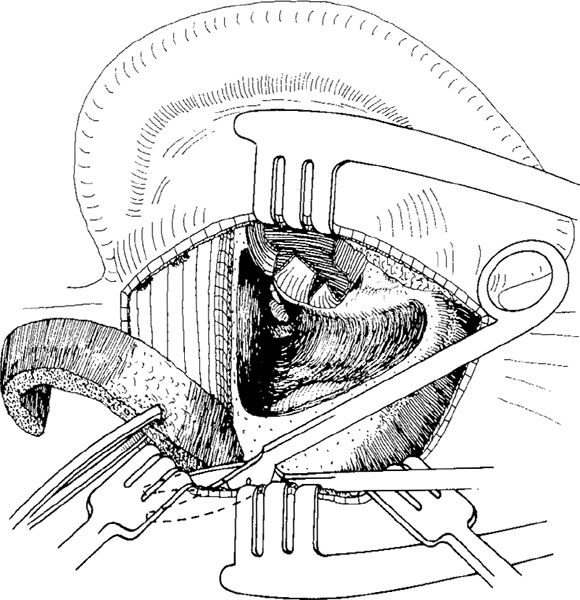
Fig. 887 The subcutis–periosteum flap and the temporalis muscle are cut posteriorly with a pair of scissors after maximal retraction of the skin
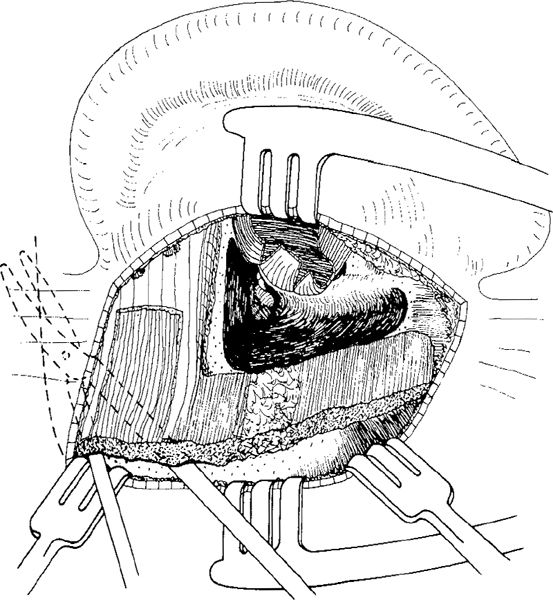
Fig. 888 Further cutting of the muscle in an anterior direction along the horizontal dashed line is partly performed blindly. A large flap is now mobilized. A large piece of temporalis muscle fascia is harvested, and the muscle flap can be cut along the vertical line
Before the muscle flap is placed, a piece of fascia is harvested from the temporalis muscle (Fig. 888). The fascia closes the ear drum perforation and covers the posterior ear canal skin, separating the skin from the muscle (Fig. 889). The canal skin flaps are returned, allowing rapid epithelialization of the enlarged ear canal over the fascia. The cavity is firmly obliterated, since the flaps are not under tension and are reasonably vascularized (Fig. 890).
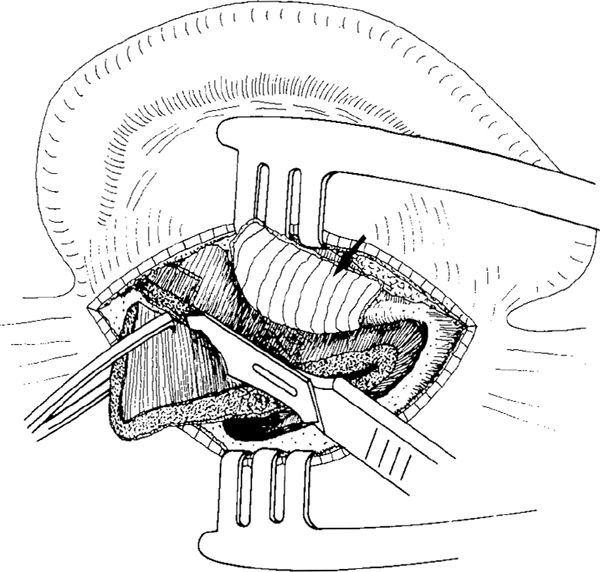
Fig. 889 The fascial graft is placed in the tympanic cavity. After the ear canal skin flaps have been replaced, the temporalis muscle fascia covers the posterior aspect of the ear canal (arrow). The inferior part of the subcutis–muscle flap fills the mastoid tip, and the middle part forms the ear canal. In the posterosuperior part of the temporalis muscle, a vertical incision is completed, making a posterior flap obliterating the antrum and sinodural angle
If the fascia is not large enough to cover the ear canal, a small, anteriorly-based pedicled Palva flap can be made from the anterior subcutis periosteum flap, including the postauricular muscle (Fig. 882) attached to the posterior aspect of the conchal eminence. The flap is pulled posteriorly to cover the fascia (Figs. 891 and 892).
Before obliteration, the ear canal is widened with incisions at the 12-o’clock and 6-o’clock positions running through the external auditory meatus. The ear canal is packed with Gelfoam balls immediately after the fascia is placed and after, the canal skin flaps have been replaced. Finally, a 1–cm strip of gauze moistened with oxytetracycline and hydrocortisone ointment (Terra-Cortril) is placed in the widened ear canal (Fig. 892). The pack is removed after three weeks. A further piece of gauze is placed in the ear canal for at least a further two weeks in order to keep it widened.
The late results one to six years after surgery on 103 patients were good (Tos 1969). Eighty percent remained completely dry with no postoperative aural complaints, and 11% had intermittent discharge during the first six to 12 months postoperatively, but thereafter it ceased and at further follow-up checks, the ears were dry and the cavity was epithelialized. The majority of patients developed some residual cavity, but the cavity lining was intact and the migration properties of the epithelium were good, with the cavities generally being selfcleaning.
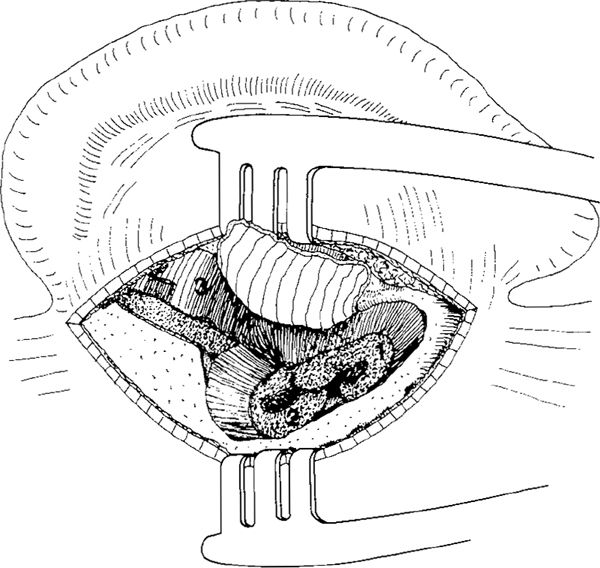
Fig. 890 The bipartite flap is now in place. One end fills the inferior part of the cavity (1), and the other the antrum and the sinodural angle (2). The base of the flap (3) covers the superior wall of the cavity and forms the ear canal wall, behind the temporalis fascia graft
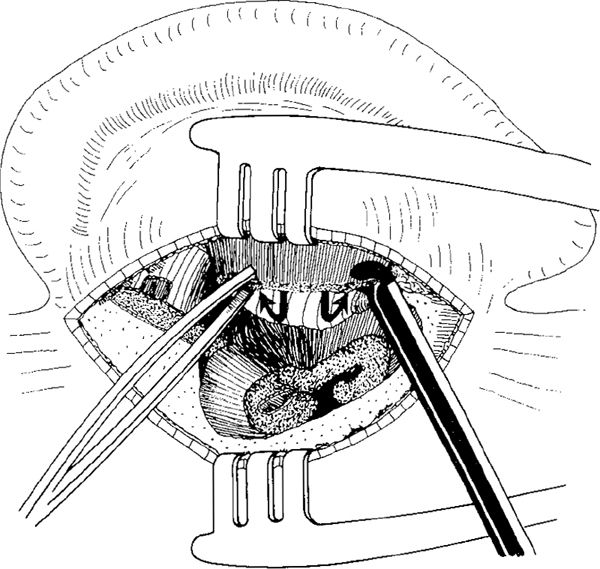
Fig. 891 From the fibrous tissue and the remnant of the postauricular muscle, a small anterior pedicled flap is elaborated and pulled behind the fascia (arrows)
This method allows obliteration of large cavities, because a large part of the temporalis muscle, as well as the retroauricular fibrous tissue and the mastoid tip muscles, are included in the flap. The retroauricular incision is, however, essential for this flap.
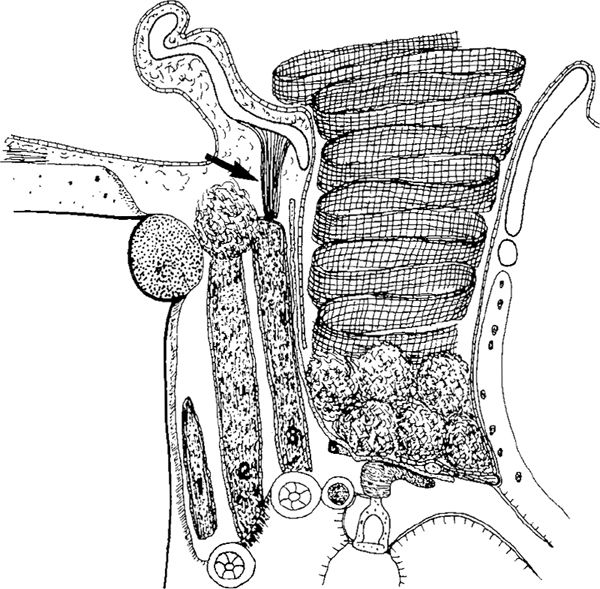
Fig. 892 The Tos bipartite flap, seen in a side view. A large piece of fascia covers the ear drum perforation as an underlay graft. It is attached to the preserved bridge, and continues laterally under the laterally-based canal skin graft, forming the ear canal. The relatively solid muscle flaps are obliterating the cavity, the inferior part (1), the posterior part (2), and the anterior part (3), forming the ear canal wall. From the concha, a small pedicled flap, consisting mainly of postauricular muscle, covers the fascia (arrow). The ear canal is widened and packed with Gelfoam balls and a gauze moistened with oxytetracycline and hydrocortisone (Terra-Cortril) ointment
The Guilford Superior Pedicled Flap
The Guilford (1961) flap is used in an endaural approach and the flap is harvested using a retroauricular incision (Fig. 893). The base is located anterosuperiorly at the junction of the temporalis muscle with the postauricular muscle. The flap contains the subcutaneous and fibrous tissue, the postauricular muscle, and the periosteum. After a retroauricular incision, the subcutis muscle flap is elevated (Fig. 894). The flap covers the mastoid tegmen, the sinodural angle, and the medial wall of the cavity (Fig. 895).
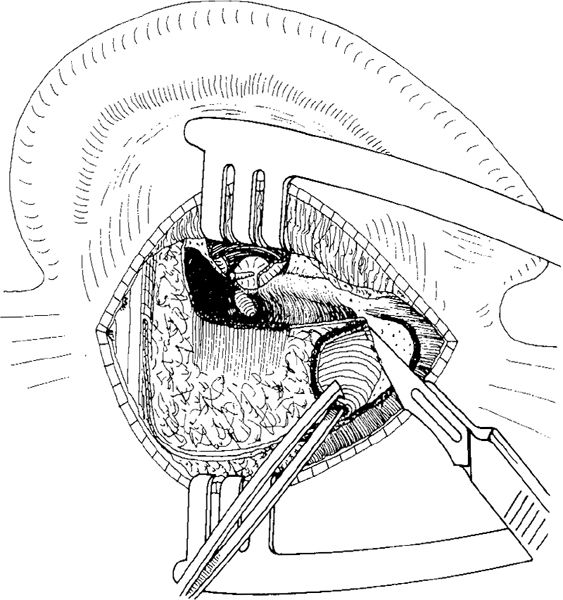
Fig. 893 The Guilford superior pedicled flap. After a canal wall–down mastoidectomy performed in an endaural approach, a retroauricular incision is made and the skin is elevated. The subcutis and periosteum is incised, starting at the inferior border of the temporalis muscle and continuing posteriorly and inferiorly. At the mastoid tip, the fibers of the sternocleidomastoid muscle are cut, and dissection of the flap is started. A canal wall–down mastoidectomy cavity is visible. The bridge is removed, and the malleus head is resected
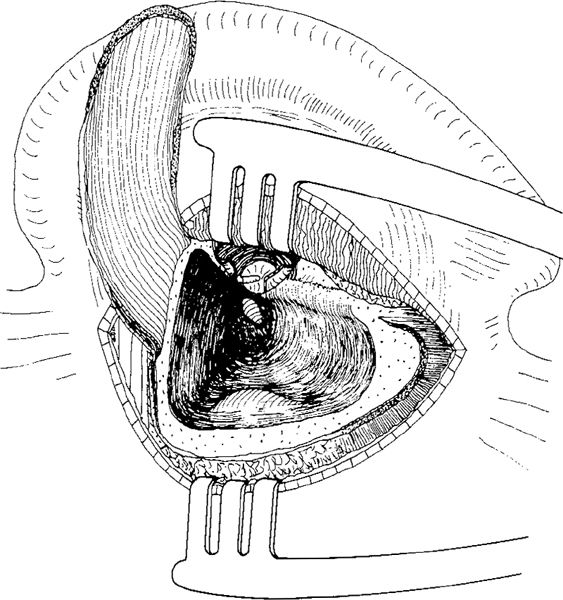
Fig. 894 The flap is elevated. It is pedicled antrosuperiorly. The periosteum is attached to the flap, and inferiorly the flap contains some muscle fibers
The Elbrønd Flap
The Elbrønd superiorly-based subcutis–periosteal flap (Elbrønd 1963) is a modification of Guilford’s method (1960). The method is based on two approaches. First, the canal wall–down mastoidectomy is performed using an endaural approach. A retroauricular incision is then made (Fig. 896) to harvest the subcutis–muscle–periosteum flap, which includes the superficial fibers of the sternocleidomastoid muscle, the splenius capitis muscle, the transversus capitis muscle, and the longissimus capitis muscle, as well as the fibrous tissue and the periosteum posterior to the cavity. After elevation of the skin with two additional retractors, the muscle fibers are cut with a scalpel directed tangentially toward the mastoid tip (Fig. 897). All the fibers from the mastoid tip and the muscle fibers behind the mastoid tip are elevated and divided from their bony attachment. The flap is elevated in a superior direction, as far as the inferior border of the temporalis muscle (Fig. 898), and placed in the cavity (Fig. 899). It predominantly covers the posterior walls of the cavity, the sinodural angle, and the mastoid tip, but it does not reach the aditus ad antrum, the attic, or the lateral semicircular canal (Fig. 896). Compared to the Guilford flap, the Elbrønd flap is larger, and its pedicle is placed further posteriorly.
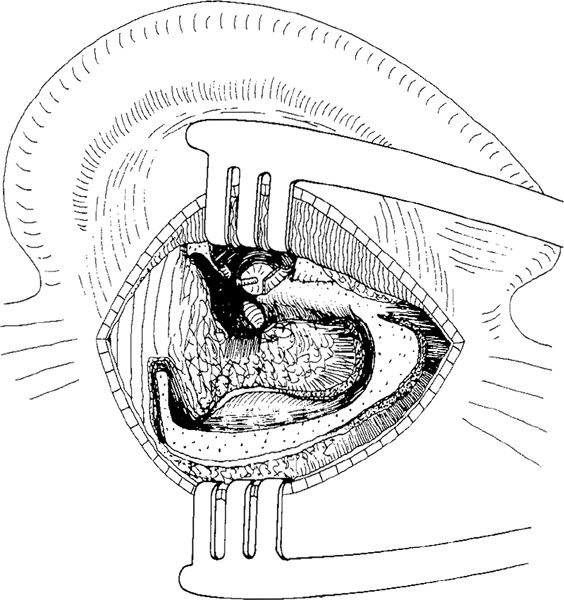
Fig. 895 The flap is placed in the cavity. It covers the mastoid tegmen and the medial aspect of the cavity, but in cannot totally obliterate the cavity
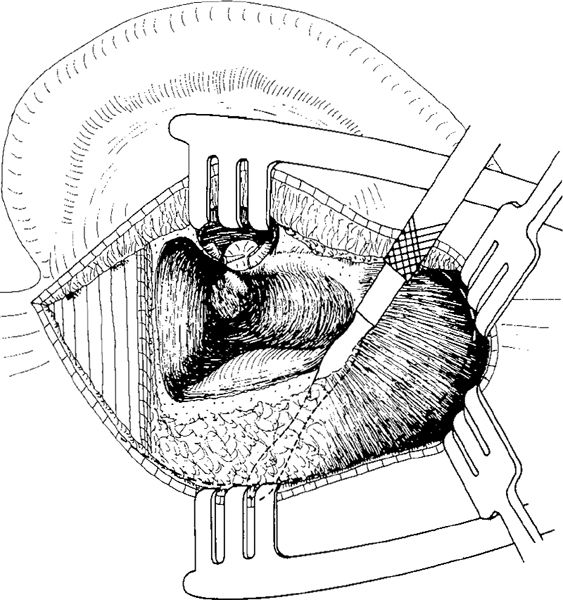
Fig. 896 The Elbrønd superior pedicled flap. A canal wall–down mastoidectomy in an endaural approach has just been performed. The tympanomeatal flaps are elevated, the malleus head is resected, the incus is extruded, and the bridge is removed. A retroauricular incision is performed, and the skin is elevated far posterior to the cavity. The subcutaneous tissue and periosteum is detached from the bone. The dashed line indicates the size of the flap, which involes the fibers of the sternocleidomastoid muscle, splenius capitis muscle, and transversus nuchae muscle
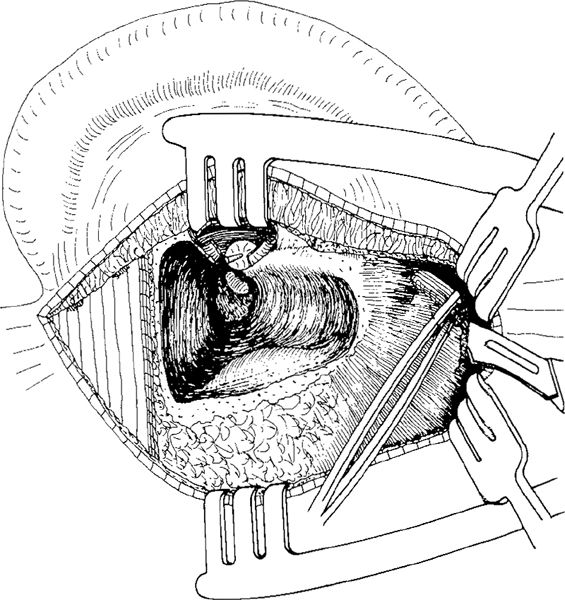
Fig. 897 The muscle fibers of the sternocleidomastoid muscle are cut with a scalpel directed tangentially toward the mastoid tip
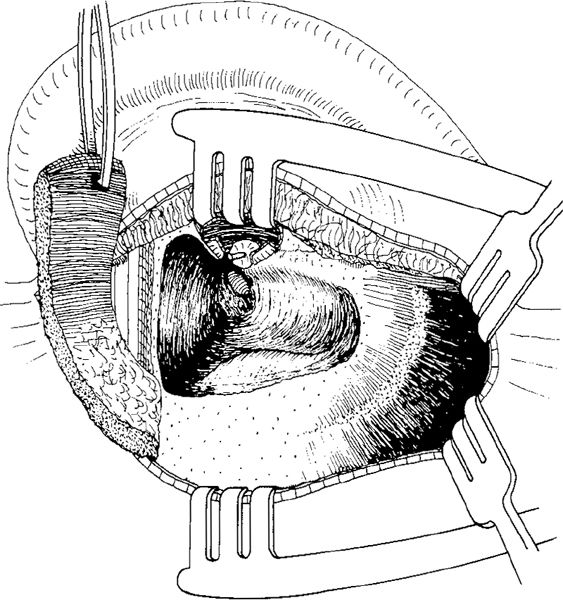
Fig. 898 The entire flap is elevated. Inferiorly, it mainly consists of muscles, while superiorly it consists of subcutaneous tissue and periosteum. It is pedicled posterosuperiorly
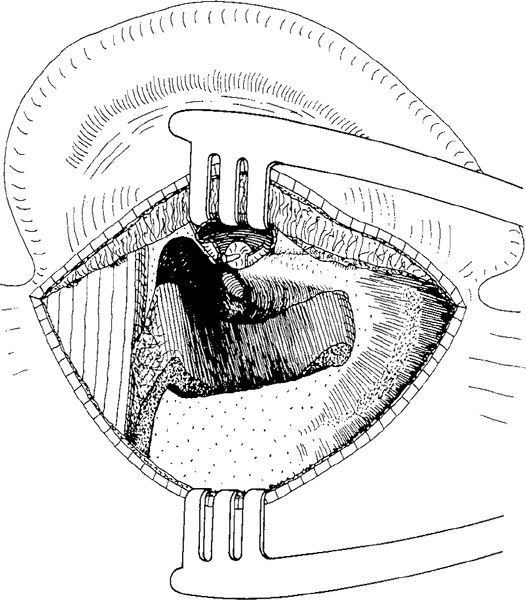
Fig. 899 The flap is placed in the cavity. It mainly covers the posterior walls of the cavity and the sinodural angle, as well as the mastoid tip
The Turner Temporalis Muscle Double Flap
The principle of this modification of the Rambo technique is to raise enough temporalis muscle tissue to divide the muscle into two separate flaps. The first is anterosuperiorly based, consisting of the inferior part of the muscle and covering the mastoid tegmen and the anterosuperior part of the cavity. The other muscle flap consists of the superior part of the temporalis muscle. It is posterosuperiorly based, and obliterates the sinodural angle, the posterior part of the cavity, and the mastoid tip (Turner 1966, 1972).
The surgical technique for this method is, however, complex and time-consuming. It starts with a large endaural incision, with the vertical skin incision continuing above the pinna and around the postauricular region to the mastoid tip (Fig. 900). It is similar to the Heermann C incision (Vol. 1, p. 24). and to the superior approach (Vol. 1, pp. 63–67), but Turner rotates the auricle completely out of the operating field. A large, laterally-based skin flap is elevated laterally, exposing the posterior ear canal. A swing-door technique with elevation of superior and inferior tympanomeatal flaps exposes the tympanic cavity (Fig. 901). The incision goes through the anterior and superior auricular muscles, and allows extensive exposure of the temporalis muscle fascia by spreading the blades of a pair of Metzenbaum scissors two or three times in various directions. The upper half of the auricle is retracted posteriorly, and the root of the helix along the conchal cartilage is freed from the mastoid process. The auricle is now completely rotated except for a 3.5–4.0–cm pedicle extending from the anterior border of the mastoid tip to the tragus (Fig. 902). After harvesting of the fascia and after a canal wall–down mastoidectomy, the anterosuperiorly-based temporalis muscle flap is cut out and elevated (Fig. 903). The anterior flap is placed in the cavity, and the posterior flap is then elevated. This elevation extends to the inferior edge of the temporalis muscle and to the occipitomastoid suture (Fig. 904). Finally, the posterosuperiorly-based flap is placed in the cavity, covering the posterior part of the mastoid tegmen, the sinodural angle, and the posterior wall of the cavity (Fig. 905). The auricle is replaced, and the fascia is placed under the drum remnant. The tympanomeatal flaps are replaced, covering the muscle flaps. The laterally-based conchal canal skin flap is replaced in such a way that it covers the muscle and maintains a wide ear canal (Fig. 906).
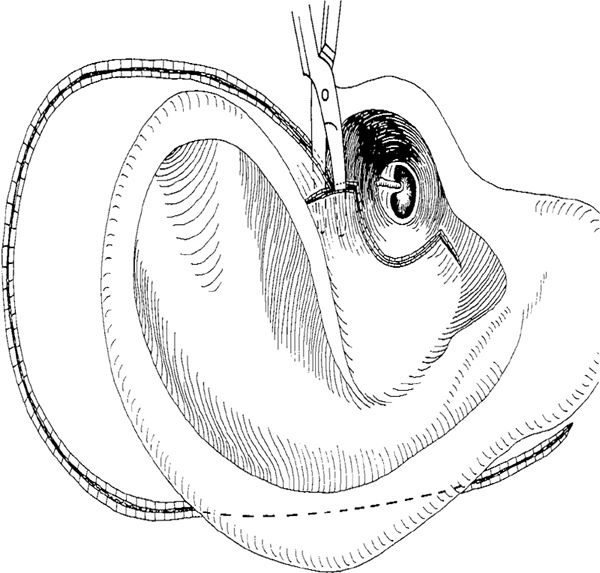
Fig. 900 The Turner temporalis muscle double flap. An endaural approach, with a lateral circumferential incision and radial incisions at the 6-o’clock and 12-o’clock position is made. The vertical incision goes far around the pinna, through the postauricular region, to the mastoid tip
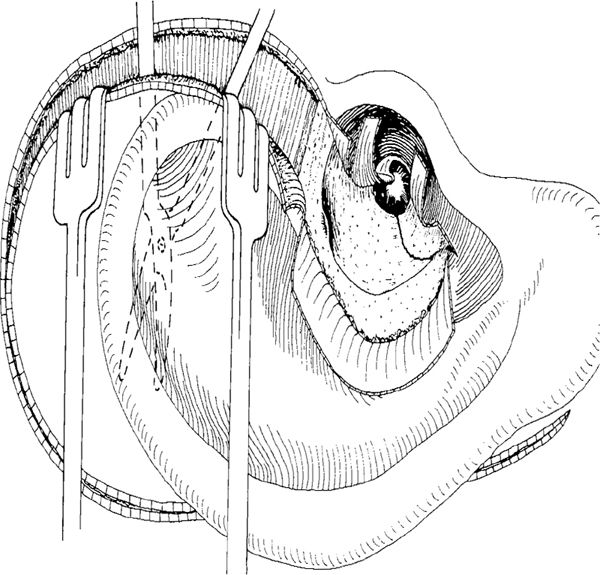
Fig. 901 A laterally-based conchal flap is elevated. The pinna is liberated from the temporalis muscle fascia after the blades of a pair of Metzenbaum scissors have been spread two or three times in various directions. In the tympanic cavity region, the tympanomeatal flap is cut at the 9-o’clock position. Superior and inferior skin flaps are elevated, exposing the edges of the total perforation
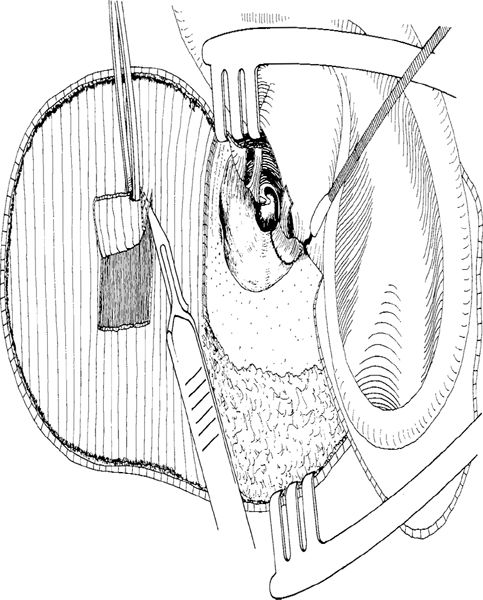
Fig. 902 After it has been totally freed, the auricle is rotated out of the operating field, but remains attached to the anterior part of the ear canal, with a 3–4 cm–long pedicle extending from the anterior border of the mastoid tip to the tragus. A large area of the temporalis muscle is exposed, and a large piece of fascia is harvested
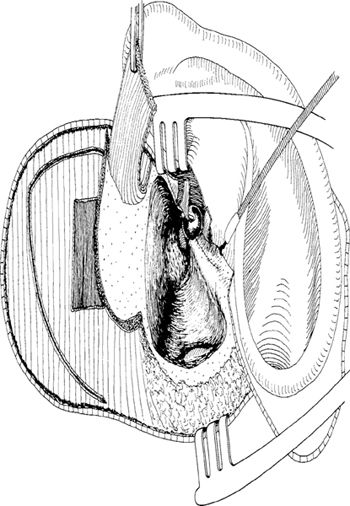
Fig. 903 A canal wall–down mastoidectomy with removal of the bridge is performed, and the anterosuperiorly-pedicled temporalis muscle flap is cut out and elevated
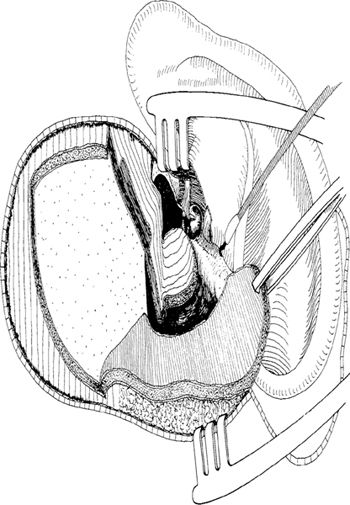
Fig. 904 The anterior flap is placed in the anterior part of the cavity, and the large, posteriorly-pedicled flap is elevated
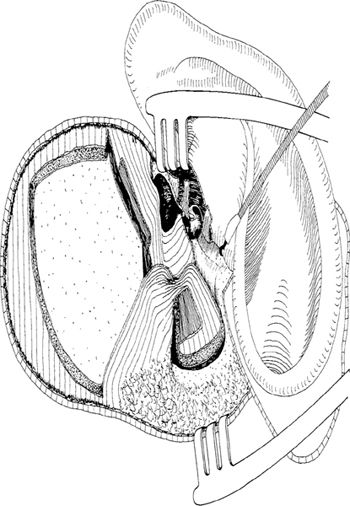
Fig. 905 The superoposteriorly-pedicled flap is placed in the posterior part of the cavity
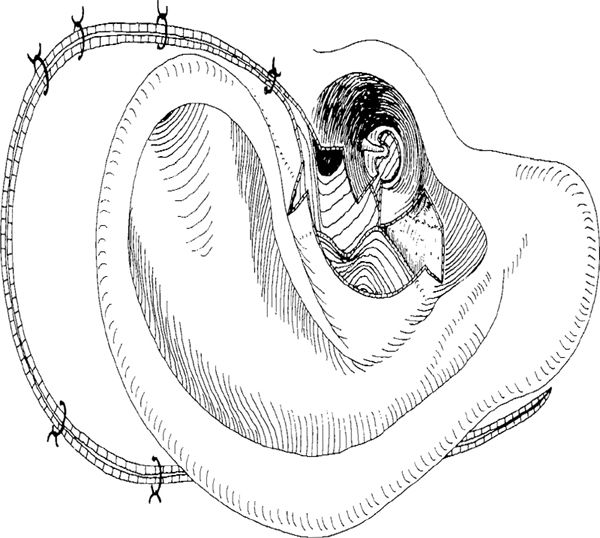
Fig. 906 The auricle is replaced and partly sutured. The subtotal perforation is covered with an underlay fascial graft, and the tympanomeatal flaps are replaced, partly covering the anterior muscle flap. The conchal flap is replaced, and the ear canal is widened
Posterosuperiorly Based Musculofascial Flap
For reconstruction of old radical cavities, Dawlatly (1992) described an obliteration technique using part of the temporalis muscle pedicled posterosuperiorly, along with fibrous tissue and periosteum. After a large S-shaped retroauricular skin incision (Fig. 907), a large area of temporalis muscle fascia is exposed (Fig. 908). A piece of fascia is dissected and partly elevated. The fascia is still partly attached to the muscle, and will be used to cover the drum region (Fig. 909). Using cutting diathermy, a circular piece of the temporalis muscle is developed and elevated together with the periosteum to a level 1 cm inferior to the lower edge of the muscle. The posterosuperior pedicle is composed of subcutaneous tissue, fibrous tissue, and the periosteum, its vascularization coming from the occipital artery (Fig. 910). The flap is placed in the cavity, and covers its posterior wall and the antrum (Fig. 911). The pedicled fascial graft then covers the tympanic cavity region (Fig. 912).
The use of pedicled fascia is unnecessary, and a free fascial graft is easier to handle. There is no evidence of better survival for pedicled fascia as an ear drum graft when compared with a free fascial graft.
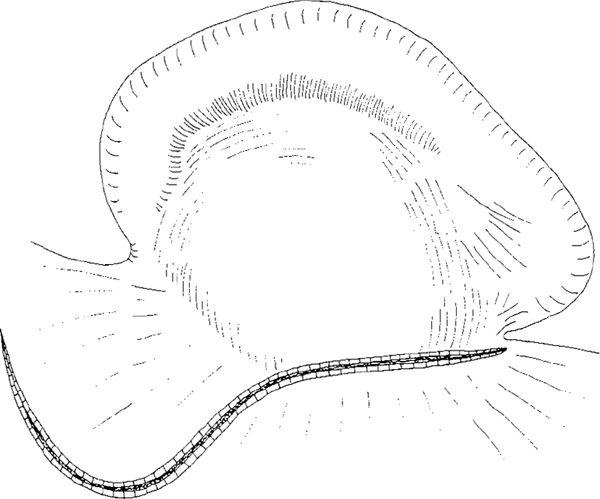
Fig. 907 Superoposteriorly pedicled musculofascial flap (Dawlatly). A large S-shaped retroauricular incision is made
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


