
Nystagmus and Other Ocular Oscillations
Nystagmus is a rhythmic, repetitive, to-and-fro movement of the eyes that includes smooth sinusoidal oscillations (pendular nystagmus) and alternation of slow drift and corrective quick phase (jerk nystagmus) (Leigh, 1999). If the size of the oscillation differs in each eye, the abnormal movements are referred to as dissociative nystagmus. If the direction of the oscillations in each eye is the same, the nystagmus is conjugate, and if they differ, the nystagmus is dysconjugate. Nystagmus induced by optokinetic or vestibular stimuli is physiologic but can be affected by pathologic processes. Nystagmus in extreme lateral or vertical gaze (end-point nystagmus) can also be found as a normal variant. End-point nystagmus tends to wane easily and belongs to the variety described below as “gaze-evoked” nystagmus. These physiologic forms of nystagmus may be pathologic if they persist beyond a few beats in end gaze.
An approach to pathologic nystagmus is presented in this chapter. The slow phase reflects the underlying abnormality causing the nystagmus. The slow component may have a uniform velocity or may reduce or gain speed as the eyes move in the direction of the slow component. This slow-phase abnormality is usually due to disruption of the mechanisms that normally function to hold gaze steady. Thus, disorders of the vestibular system, the gaze-holding mechanisms (e.g., the neural integrator), and visual stabilization and pursuit systems may lead to nystagmus (Leigh, 1999).
Vestibular tone imbalance results in an asymmetric input to the horizontal gaze generator; vestibular nystagmus shows linear, constant velocity slow phases reflecting a persistent drive of the eyes toward the damaged vestibular apparatus (labyrinth, nerve, nuclei). An impaired neural integrator (“leaky” integrator) may cause gaze-evoked nystagmus with a negative exponential slow phase. The velocity of the slow component decreases as the eyes move from the periphery of the orbit, where the pull due to the viscosity of the orbital tissues is greatest, toward resting in primary position. The inability of the gaze holding mechanisms to keep the eyes eccentric in the orbit is often present with central or peripheral lesions causing weakness of eye movements. For this reason, this type of nystagmus is sometimes referred to as “gaze-paretic” nystagmus. High gain instability of slow eye movement subsystems (e.g., the pursuit system) may also cause nystagmus, with the nystagmus slow phase having an exponentially increasing time course (“runaway” movements). Such nystagmus in the horizontal plane is seen in congenital nystagmus and in the vertical plane is seen with cerebellar disease. High gain instability may also result in congenital or acquired pendular nystagmus. The types of nystagmus and other ocular oscillations are outlined in Figure 17–1.
Are the Abnormal Eye Movements Binocular and Symmetric, Binocular and Asymmetric, or Monocular?
The oscillations may be confined to one eye (monocular), involve mainly one eye (binocular asymmetric or dissociated), or involve both eyes symmetrically (binocular symmetric) (Burde, 1991).
What Causes Monocular Eye Oscillations and Asymmetric Binocular Eye Oscillations?
Monocular eye oscillations and asymmetric binocular eye oscillations may be due to spasmus nutans and its mimickers, monocular visual deprivation or loss, monocular pendular nystagmus, internuclear ophthalmoplegia and its mimickers, partial paresis of extraocular muscles, restrictive syndromes of extraocular muscles, or superior oblique myokymia.
Spasmus nutans is a benign syndrome characterized by a triad of head nodding, nystagmus, and abnormal head posture (Gottlob, 1995b; Young, 1997). The onset is typically in the first year of life and remits spontaneously within 1 month to several (up to 8) years. The syndrome is occasionally familial and has been reported in monozygotic twins. The sinusoidal nystagmus is often intermittent, asymmetric, or unilateral, and of high frequency and small amplitude with a “shimmering” quality. The nystagmus is usually horizontal but may have a vertical or torsional component. It may be accentuated by near effort and is usually greater in an abducting eye. Rarely, convergence nystagmus may occur (Massry, 1996). The irregular head nodding with spasmus nutans has horizontal, vertical, or mixed components. Patients often also demonstrate a head turn or tilt.
In children with spasmus nutans, monocular nystagmus, or asymmetric pendular nystagmus, one must consider tumor of the anterior visual pathway (e.g., optic nerve, chiasm, third ventricle, or thalamus) (Arnoldi, 1995; Gottlob, 1990; Newman, 1990). These latter patients may also have visual loss, optic atrophy, or other signs of tumor. Other spasmus nutans mimickers include arachnoid cyst, Leigh’s subacute necrotizing encephalomyelopathy, congenital stationary night blindness (Gottlob, 1995a; Lambert, 1993), retinal dystrophy (Smith, 2000), and Bardet-Biedl syndrome (characterized by polydactyly, obesity, cognitive delay, and retinal degeneration) (Gottlob, 1999).
All children with monocular nystagmus or spasmus nutans should undergo a complete ophthalmologic examination. We recommend neuroimaging (preferably magnetic resonance imaging [MRI]) in patients with monocular or predominantly monocular oscillations, spasmus nutans, or a spasmus nutans–like clinical picture (class IV, level C). Although most cases of spasmus nutans are benign, atypical features should prompt further evaluation including older age of onset, associated visual loss, or persistence of symptoms (Gottlob, 1990; Newman, 1990). Some authors, however, have stated that the estimated prevalence of tumor in spasmus nutans is less than 1.4%, and have suggested that without other evidence of an intracranial mass lesion, neuroimaging of infants initially diagnosed with spasmus nutans may not be immediately warranted (Arnoldi, 1995). Electrophysiologic testing should be considered for a myopic child suspected of having spasmus nutans to exclude the diagnosis of congenital stationary night blindness (Lambert, 1993) or retinal dystrophy (Smith, 2000) (class IV, level C).
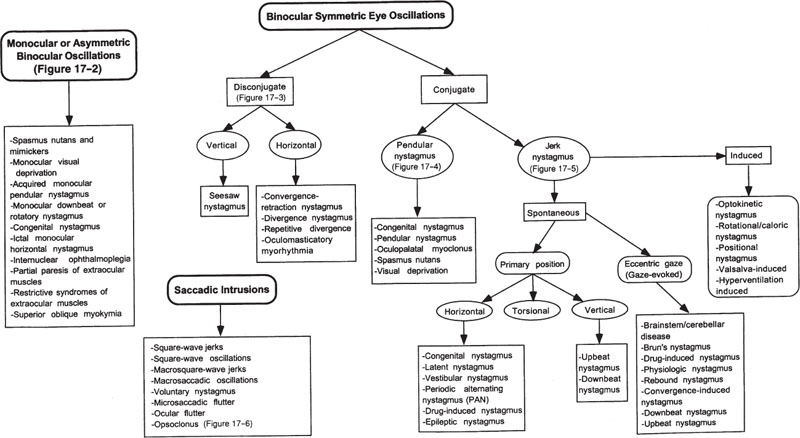
Figure 17–1. Nystagmus and other ocular oscillations.
Monocular nystagmus may occur in adults or children with acquired monocular visual loss, and consists of small, slow vertical pendular oscillations in primary position of gaze. It may develop years after uniocular visual loss (Heimann-Bielschowsky phenomenon) and may improve if vision is corrected. Monocular, small-amplitude, fast frequency, and predominantly horizontal nystagmus in children may be caused by unilateral anterior visual pathway disease (Davey, 1998; Good, 1993).
Acquired monocular pendular nystagmus may also occur with multiple sclerosis, neurosyphilis, and brainstem infarct (thalamus and upper midbrain) and may be vertical, horizontal, or multivectorial. Stahl et al (2000) reported that servo-controlled optics could reduce oscillopsia in acquired pendular nystagmus.
Vertical pendular nystagmus, with greater amplitude in the involved eye, has been described in a patient with chronic monocular myositis of the medial and lateral rectus muscles (Goldberg, 1978). Monocular downbeat nystagmus may occur with acute infarction of the medial thalamus and upper midbrain and with pontocerebellar degeneration; this abnormality is likely due to dysfunction of the ipsilateral brachium conjunctivum. Contralateral unilateral downbeat nystagmus has been described with a paramedian thalamopeduncular infarction (Oishi, 1997). Monocular rotatory nystagmus may occur with brainstem lesions. Congenital nystagmus may rarely be uniocular. One patient has been described who developed ictal monocular horizontal nystagmus during a generalized seizure triggered by photic stimulation (Jacome, 1982). We recommend that neuroimaging be performed in monocular nystagmus (class IV, level C).
Dissociated nystagmus occurs in the abducting eye in internuclear ophthalmoplegia (INO) and in pseudo-INO syndromes. These entities and their evaluation are discussed in Chapter 14. In patients with partial paresis of one of the extraocular muscles, a monocular oscillation may occur in the involved eye or its yoke during an ocular movement into the field of action of the involved muscle (Burde, 1991). Monocular oscillations may also occur in restrictive syndromes (e.g., thyroid ophthalmopathy) in the field of action in which the tethering is occurring (Burde, 1991).
Superior oblique myokymia (SOM) is a disorder of unknown etiology characterized symptomatically by oscillopsia, vertical or torsional diplopia, or both. Affected patients show bursts of rotary oscillations of the eye of small amplitude and high frequency, slow-frequency large-amplitude intorsional movements, or a combination of these paroxysms. Most patients with SOM complain of brief episodes of rapid vertical or torsional movements of the environment or shimmering sensations, usually lasting only a few seconds.
Neuro-ophthalmologic examination of SOM patients often reveals brief episodes of rapid, fine, torsional movements of one eye that are best seen using either the slit-lamp biomicroscope or the direct ophthalmoscope. The abnormal movements can be induced in some patients by movement of the affected eye down and outward, by a head tilt toward the side of the affected eye, by convergence effort, or by movement of the eye downward and back to primary position.
Patients with SOM are usually young adults who are otherwise healthy Most patients report no precipitating event for the onset of their symptoms. Several cases have followed ipsilateral trochlear nerve palsies, leading some authors to suggest that SOM might be associated with the recovery stage of injury to this nerve (Komai, 1992). SOM has occurred several months after removal of a cerebellar tumor. In addition, two cases of SOM have occurred in patients with posterior fossa tumors (one an astrocytoma of the rostral cerebellar vermis with midbrain tectal compression and the other a pilocytic astrocytoma expanding within the fourth ventricle and compressing the midbrain tectum) (Haene, 1993; Morrow, 1990). The rare association of SOM with brainstem tectal disease has caused some authors to recommend neuroimaging examination of the course of the trochlear nerve in all patients with this diagnosis (Morrow, 1990); however, the association of SOM with a posterior fossa tumor is extremely uncommon (Brazis, 1994) (class IV, level U). In one reported case, SOM may have been due to vascular compression of the trochlear nerve by a branch of the posterior cerebral artery noted on thin-slice MRI (Hashimoto, 2001). In another study of six patients with SOM, neurovascular contact at the root exit zone of the trochlear nerve was identified in all patients, suggesting that SOM may be a neovascular compression syndrome (Yousry, 2002). SOM has been described in a patient with a dural arteriovenous fistula (Geis, 1996), and Neetens and Martin described two cases of SOM, one associated with lead intoxication and the other with adrenoleukodystrophy (Neetens, 1983). Some of these associations may well have been coincidental (class IV). We do not recommend neuroimaging for typical isolated SOM but consider MRI scan in patients with atypical features (class IV, level C).
Rosenberg and Glaser obtained from 1 to 19 years (average 8 years) of follow-up for nine patients with SOM (Rosenberg, 1983). These authors noted that the natural history of the disorder is one of spontaneous remissions and exacerbations, with untreated patients frequently enjoying months or even years of remission before subsequent relapses. Indeed, seven of their nine patients continued to have some symptoms after prolonged follow-up.
The treatment for a majority of patients with SOM is reassurance, because most are not significantly disabled by their visual symptoms. If the condition disrupts the patient’s work and lifestyle, medications such as carbamazepine or propranolol (Tyler, 1990) may be considered. In Rosenberg and Glaser’s series, 7 of 11 patients were tried on carbamazepine, and 6 noted a prompt decrease or cessation of ocular symptoms (Rosenberg, 1983). All experienced at least one subsequent relapse days to months after the initial improvement, however, and only three chose to continue the medication. We have tried gabapentin in one patient with SOM without subjective or objective improvement.
Brazis et al investigated the clinical presentations and long-term course of 16 patients with SOM (Brazis, 1994). Follow-up information was obtained for 14 of the 16 patients with time from onset of symptoms to most recent contact 3 to 29 years (mean, 12 years). The SOM gradually improved or resolved, at least temporarily, without treatment in a significant number of patients. Three of the patients had complete spontaneous resolution of symptoms for periods of 6 to 12 months without recurrence. Six of 7 patients treated with carbamazepine reported no significant response. One patient remained on the medication for 3 years with only rare symptoms that worsen when attempts were made to taper the drug. Two of the patients treated with propranolol reported no significant benefit, and a third noted dramatic but transient improvement in symptoms. Four of the patients were cured by superior oblique tenectomy combined with inferior oblique myectomy. All four surgical patients experienced disappearance of oscillopsia, although one patient developed postoperative vertical diplopia that gradually resolved. Brazis et al concluded that because SOM is a much more chronic disease than formerly realized and because of the poor long-term effects and potential side effects of the medications used for treatment, medical treatment of SOM, at least with currently available medications, may not be the optimum way to manage the disease. They believe that surgery is the treatment of choice when symptoms of SOM are intolerable to the patient. Other authors have also reported successful treatment of SOM with surgery (de Sa, 1992; Hayakawa, 2000). For example, Kosmorsky et al performed a Harada-Ito procedure on a woman with SOM (Kosmorsky, 1995). This procedure involves nasally transposing the anterior portion of the superior oblique tendon, which is responsible for the cyclorotation, to create an effective weakening of the anterior portion of the tendon instead of temporal displacement utilized for superior oblique paresis. The SOM was abolished and vertical eye movements, including saccades, were unaffected. Samil et al reported one patient with SOM who responded to microvascular decompression of the fourth nerve at the root exit zone (Samil, 1998).
The treatment of SOM is usually reassurance and the condition may be self-limiting. When symptoms are intolerable, medical or surgical therapy may be considered. A weakening procedure of the affected superior oblique muscle combined with a weakening procedure of the ipsilateral inferior oblique muscle or the Harada-Ito procedure is an effective treatment for SOM after failure of medical treatment or as an alternative to such treatment, and should be considered in patients with unacceptable visual symptoms. Microvascular decompression of the fourth cranial nerve at the root exit zone may be another approach, but so far there has been little experience with this procedure for SOM.
The evaluation of monocular or asymmetric binocular oscillations is outlined in Figure 17–2.
What Are the Causes of Dysconjugate Bilateral Symmetric Eye Oscillations?
If the ocular oscillations involve both eyes to a relatively equal degree, the next step in evaluation involves determining whether the eye movements are disconjugate (the eyes moving in opposite directions) or conjugate (both eyes moving in the same direction) (Burde, 1991). When the oscillations are disconjugate, the examiner should determine whether the oscillations are vertical or horizontal. Vertical disconjugate eye oscillations are usually due to seesaw nystagmus. Horizontal disconjugate eye oscillations include convergence-retraction nystagmus (nystagmus retractorius), divergence nystagmus, repetitive divergence, and oculomasticatory myorhythmia.
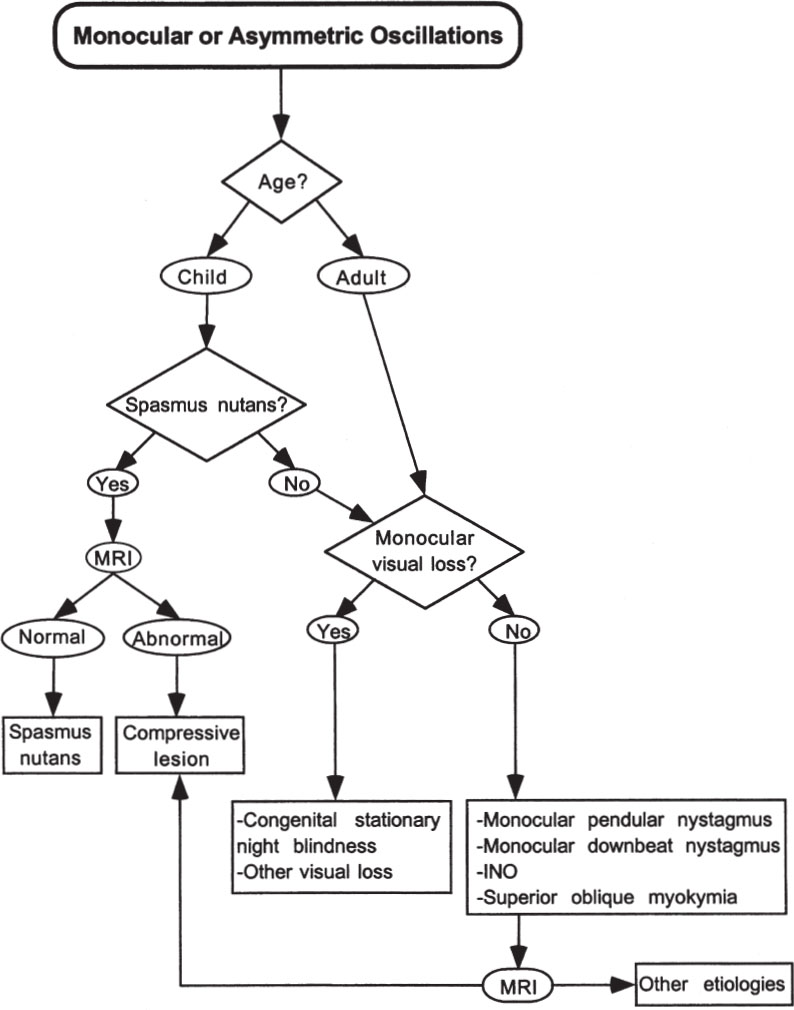
Figure 17–2. Evaluation of monocular or asymmetric oscillations.
What Are the Clinical Features and Etiologies of Seesaw Nystagmus?
Seesaw nystagmus is a cyclic movement of the eyes with a conjugate torsional component and a dysjunctive vertical component. While one eye rises and intorts, the other falls and extorts; the vertical and torsional movements are then reversed, completing the cycle. This nystagmus is usually pendular and may be due to a large suprasellar lesion compressing or invading the brainstem bilaterally at the mesodien-cephalic junction. Pendular seesaw nystagmus may also be congenital (May, 1997). Seesaw nystagmus may also have a underlying jerk waveform, often due to a intrinsic focal brainstem lesion, either in the lateral medulla (usually on the side opposite the torsional quick phases) or in the mesodiencephalon on the same side as the quick phases (Halmagyi, 1991, 1994). Jerk seesaw nystagmus has a slow phase corresponding to one half-cycle of seesaw nystagmus and is thus often called hemi-seesaw nystagmus.
Seesaw nystagmus likely represents oscillations involving central otolithic connections, especially the interstitial nucleus of Cajal (Halmagyi, 1991). Seesaw nystagmus may also be in part due to an unstable visuovestibular interaction control system. Lesions in the optic pathways may prevent retinal error signals, essential for vestibulo-ocular reflex adaptation, from reaching the cerebellar flocculus and inferior olivary nucleus, thereby making the system less stable. Etiologies responsible for seesaw nystagmus are outlined in Table 17–1.
Chiari malformation type I may be associated with nystagmus of skew in which one eye beats upward while the other eye beats downward (Pieh, 2000). The evaluation of a patient with seesaw nystagmus includes a complete ophthalmologic and neurologic examination. Patients with parasellar lesions often have bitemporal field defects and “bow-tie” optic atrophy associated with pendular seesaw nystagmus. Jerk seesaw nystagmus usually is associated with other brainstem signs. We recommend neuroimaging (preferably MRI attending to parasellar and posterior fossa regions) for patients with seesaw nystagmus, with particular attention to the third ventricle/parasellar area (class IV, level C). The presence of this nystagmus with a skew deviation requires MRI studies for a Chiari malformation (class IV, level C). The treatment of seesaw nystagmus is directed at the responsible lesion. One patient with intermittent seesaw nystagmus responded to clonazepam, and the nystagmus did not recur after withdrawal of the medication (Cochin, 1995). Also, baclofen, with and without clonazepam, improved both nystagmus and associated oscillopsia in another patient, suggesting a possible γ-aminobutyric acid (GABA)-ergic mechanism influencing the interstitial nucleus of Cajal.
Parasellar masses (Barton, 1995) Brainstem and thalamic stroke (Halmagyi, 1991, 1994) Multiple sclerosis (Samkoff, 1994) Trauma Chiari malformation Hydrocephalus Syringobulbia Paraneoplastic encephalitis (with testicular cancer and anti-Ta antibodies) (Bennett, 1999) Whole brain irradiation and intrathecal methotrexate (Epstein, 2001) Septo-optic dysplasia, retinitis pigmentosa, and cone degeneration (May, 1997) Congenital seesaw nystagmus* (Rambold, 1998) |
*Congenital seesaw nystagmus may lack the torsional component or even present with an opposite pattern, that is, extorsion with eye elevation and intorsion with eye depression. With congenital cases, the binocular torsional eye movements may be in phase with clinically visible head oscillations (i.e., head movements are not compensatory for the torsional eye movements) (Rambold, 1998).
What Are the Causes of Horizontal Dysconjugate Eye Oscillations?
Convergence may evoke various forms of nystagmus (i.e., convergence-evoked nystagmus; see below). Convergence-retraction nystagmus is a disorder of ocular motility in which repetitive adducting saccades, which are often accompanied by retraction of the eyes into the orbit, occur spontaneously or on attempted upgaze (Pullicino, 2000). Rotating an optokinetic tape or drum downward may elicit the movements. Convergence-retraction nystagmus is primarily a saccadic disorder as the convergence movements are not normal vergence movements but asynchronous, adducting saccades. Other authors feel that convergence-retraction nystagmus is a disorder of vergence rather than of opposing adducting saccades (Rambold, 2001b). Mesencephalic lesions affecting the pretectal region are most likely to cause this type of nystagmus, which is often associated with abnormalities of vertical gaze. The localization and evaluation of these vertical gaze abnormalities and convergence-retraction nystagmus are discussed in Chapter 14. Convergence nystagmus has been described without vertical gaze abnormalities in patients with dorsal midbrain stroke and in patients with Chiari malformation (Mossman, 1990; Schnyder, 1996). Whipple’s disease may also cause convergence nystagmus at approximately 1 Hz (pendular vergence oscillations) (Selhorst, 1987). Convergence nystagmus has been described in a patient with spasmus nutans (Massry, 1996).
Divergence nystagmus (with divergent quick phases) may occur with hindbrain abnormalities (e.g., Chiari malformation) and is associated with downbeat nystagmus. These patients have slow phases directed upward and inward. Repetitive divergence consists of a slow divergent movement followed by a rapid return to the primary position at regular intervals (Noda, 1987). This rare disorder has been described with coma from hepatic encephalopathy. A similar disorder, probably related to seizures, was reported in a neonate in association with burst-suppression patterns of the electroencephalogram (Nelson, 1986).
Oculomasticatory myorhythmia refers to acquired pendular vergence oscillations associated with concurrent contraction of the masticatory muscles (Adler, 1990; Louis, 1996). If nonfacial skeletal muscles are involved, it is called oculofacial-skeletal myorhythmia. There is a smooth, rhythmic eye convergence, which cycles at a frequency of approximately 1 Hz, followed by divergence back to the primary position. Rhythmic elevation and depression of the mandible is synchronous with the ocular oscillations that persist in sleep and are unaltered by stimuli. The masticatory involvement may occasionally consist of a permanent bruxism leading to severe tooth abrasions (Tison, 1992). Patients with oculomasticatory myorhythmia may also have paralysis of vertical gaze, progressive somnolence, and intellectual deterioration. This distinct movement disorder has been recognized only in Whipple’s disease (class III–IV, level B).
Therefore, if this condition is diagnosed, empiric antibiotic treatment should be considered and tissue diagnosis should be attempted. Whipple’s disease may be diagnosed by endoscopically guided biopsy of multiple jejunal sites (Adler, 1990; Louis, 1996). Electron microscopy and polymerase chain reaction (PCR)-based testing on intestinal or extraintestinal tissue may also confirm the diagnosis (Louis, 1996; Tison, 1992). PCR can also be performed on cerebrospinal fluid in central nervous system (CNS) Whipple’s disease (Lynch, 1997; Von Herbay, 1997).
The evaluation of disconjugate bilateral symmetric eye oscillations is outlined in Figure 17–3.
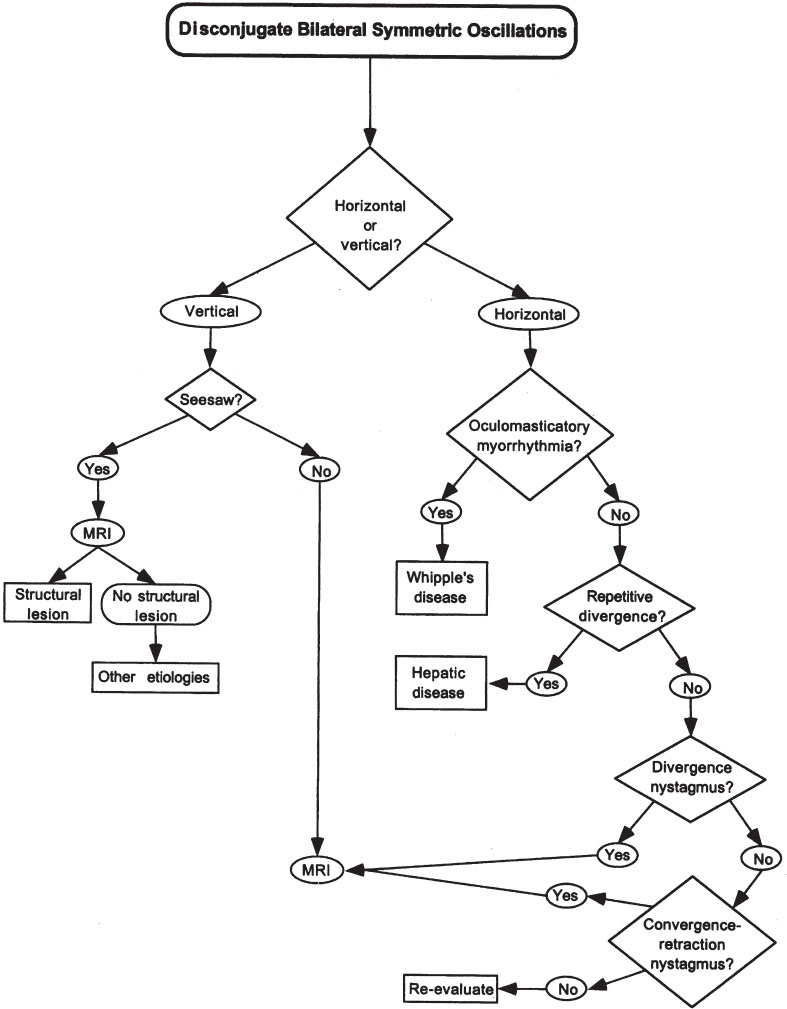
Figure 17–3. Evaluation of disconjugate bilateral symmetric oscillations.
What Are the Causes of Binocular Symmetric Conjugate Eye Oscillations?
Binocular symmetric conjugate eye oscillations may be divided into pendular nystagmus, jerk nystagmus, and saccadic intrusions (Burde, 1991).
What Are the Causes of Binocular Symmetric Pendular Conjugate Eye Oscillations?
Binocular symmetric pendular conjugate eye oscillations may be due to congenital nystagmus, pendular nystagmus, oculopalatal myoclonus, spasmus nutans (discussed above), and visual deprivation nystagmus.
Congenital nystagmus may be noted at birth or in early infancy, or may emerge or enhance in teenage or adult life (Dell’Osso, 1993; Gresty, 1991; Hertle, 1999). It may be familial, hereditary (X-linked, autosomal dominant, autosomal recessive) (Kerrison, 1999; Oetting, 2000) or idiopathic. Metabolic derangements and structural anomalies of the brain, including abnormalities of the anterior and posterior visual pathways, may be responsible (Jacobson, 1998). More important, when it is found later in life it must be distinguished from other forms of nystagmus that have a potentially treatable cause. Congenital nystagmus may be wholly pendular or have both pendular and jerk components. Congenital jerk nystagmus has a slow phase with a velocity that increases exponentially as the eyes move in the direction of the slow phase. Occasionally congenital nystagmus may be purely vertical or torsional, and although these findings usually implicate an intracranial lesion, these forms of nystagmus may occur in sensory congenital nystagmus (Shawkat, 2000). Although irregular, congenital nystagmus is generally conjugate and horizontal, even on upgaze or downgaze (uniplanar), visual fixation accentuates it and active eyelid closure or convergence attenuates it (Gresty, 1991). The nystagmus decreases in an eye position (“null region”) that is specific for each patient. Despite the constant eye motion, these patients do not experience oscillopsia. When they are tested with a hand-held optokinetic tape or drum, the quick phase of the elicited nystagmus generally follows the direction of the tape (reversed optokinetic nystagmus).
Symptomatic oscillopsia in patients with congenital nystagmus is unusual but may be precipitated after visual maturation by new or changing associated visual sensory conditions (e.g., decompensating strabismus or retinal degeneration) (Hertle, 2001). Congenital nystagmus has been associated with many disease processes affecting the visual afferent system including ocular and oculocutaneous albinism, achromatopsia, optic nerve hypoplasia, Leber’s amaurosis, coloboma, aniridia, cone dystrophies, corectopia, congenital stationary night blindness, Chédiak-Higashi syndrome, Joubert syndrome, and peroxisomal disorders. It has also been associated with hypothyroidism. The evaluation of children with congenital nystagmus thus should include a complete ophthalmologic examination, especially attending to symptoms of photophobia and paradoxical pupillary constriction in darkness, and thyroid functions. An electroretinogram (ERG) may be helpful even with a normal afferent exam (Cibis, 1993). For example, 56% of 105 consecutive patients with congenital nystagmus were found to have retinal disease when tested with ERG (Cibis, 1993).
Congenital nystagmus often decreases in an eye position (“null region”) that is specific for each patient, and convergence often attenuates the nystagmus. Prisms can be used to take advantage of the dampening effect of convergence and the null region–lens combinations can be adjusted so that an asymmetric arrangement of base-out prisms both converge the eyes and turn them toward the null angle. Leigh et al suggest 7.00-diopter base-out prisms with –1.00-diopter spheres added to compensate for accommodation (Leigh, 1994). Contact lenses may improve vision in patients with congenital nystagmus, possibly due to tactile feedback. Another approach for the treatment of severe nystagmus in general involves employing an optical system to stabilize images on the retina (Leigh, 1994; Yaniglos, 1992). The combination of high “plus” (i.e., converging) spectacle lenses with high “minus” (i.e., diverging) contact lenses is used with the converging system focusing the image at the center of eye rotation (thus, stabilizing the image) and the diverging system moving the image back to focus on the retina. The contact lens moves with the eye so it does not negate the effect of image stabilization produced by the spectacle lens. This imaging system is theoretically beneficial but difficult to maintain in practice, especially as the system disables the vestibulo-ocular reflex and is thus only useful when the patient is stationary.
Congenital nystagmus may also be treated with botulinum toxin injections into the extraocular muscles or surgery. Acuity was restored in four patients, to the extent that they were able to receive daytime drivers licenses, by multiple horizontal recti injections of botulinum toxin (Carruthers, 1995). Surgical procedures effectively control congenital nystagmus by attempting to move the attachments of the extraocular muscles so that the null angle corresponds to the new primary position (the null region is shifted and broadened), to decrease nystagmus outside the null region, and to prolong foveation time by changing the waveform and dampening the nystagmus (Atilla, 1999; Bilska, 1995; Helveston, 1991; von Noorden, 1991; Zubkov, 1993). Procedures used include the Anderson-Kestenbaum procedure, which moves the eyes to the null region, divergence procedures, large recessions of the horizontal rectus muscles, and combined procedures (Lee, 2000; Leigh, 1994). Finally, biofeedback has been reported to help some patients with this disorder. Evans et al performed a randomized, double-masked, placebo-controlled trial of various treatments for congenital nystagmus and concluded that these putative therapies should be assumed to be placebos until proven otherwise by randomized trial (class III–IV, level C) (Evans, 1998).
Latent nystagmus is common and generally congenital (Gresty, 1992; Wagner, 1990; Zubkov, 1990). It appears when one eye is covered. Both eyes then develop conjugate jerk nystagmus, with the viewing eye having a slow phase directed toward the nose (i.e., the quick phase of both eyes beat toward the side of the fixating eye). Although present at birth, latent nystagmus is often not recognized until later in life, when an attempt is made to determine monocular visual acuity during vision screening at school. Latent nystagmus is usually associated with strabismus, especially esotropia; amblyopia may occur and binocular vision with normal stereopsis is rare. In addition to horizontal strabismus, upward deviation of the covered eye (dissociated vertical deviation or alternating sursumduction) and a torsional, occasionally pendular, component to the nystagmus may occur. Latent nystagmus is a marker for congenital ocular motor disturbance and does not indicate progressive structural brain disease (Burde, 1991).
Manifest latent nystagmus is an oscillation that occurs in patients with strabismus or acquired visual loss who have a jerk nystagmus in the direction of the fixing eye (i.e., right-beating nystagmus when fixing with the right eye and left-beating nystagmus when fixing with the left eye) (Burde, 1991). Patients with infantile uniocular blindness may have a bilateral horizontal nystagmus that represents a manifest nystagmus of the latent type (Kushner, 1995). These patients often have a family history of strabismus; the monocular blindness (opacity of the media or suppression) acts as an occluder, making manifest what would have been latent nystagmus. Therapy for latent nystagmus consists of measures to improve vision, such as patching for amblyopia in children or surgical correction of strabismus (Zubkov, 1993).
Voluntary nystagmus (psychogenic flutter) occurs in normal subjects, sometimes as a familial trait, and consists of bursts of high-frequency horizontal oscillations composed of back-to-back saccades (Lee, 1993; Sato, 1999). The movements may be vertical or torsional as well. This movement will completely disappear if patients are forced to keep their eyes open, because it requires tremendous volitional effort and cannot be sustained for prolonged periods of time (Burde, 1991). Voluntary nystagmus is often accompanied by a “fixed look” required to produce the symptoms, eyelid flutter, and convergence. Voluntary nystagmus may be associated with spasm of the near reflex (Sato, 1999) and has been described as a component of nonepileptic seizures (Davis, 2000).
Although pendular nystagmus is often congenital, acquired forms exist. Acquired pendular nystagmus may be wholly horizontal, wholly vertical, or have mixed components (circular, elliptical, or windmill pendular nystagmus). Pendular nystagmus may be symmetric, dissociated, or even monocular and often causes distressing oscillopsia and decreased visual acuity (Averbuch-Heller, 1995b; Barton, 1993; Lopez, 1996). Damage to the dentatorubro-olivary pathways (Guillain-Mollaret triangle) is found in some cases of acquired pendular nystagmus, which is most often caused by multiple sclerosis, stroke, or tumor of the brainstem or other posterior fossa structures (Averbuch-Heller, 1995b; Barton, 1993, 1999; Lopez, 1996; Revol, 1990; Schon, 1999; Starck, 1997; Talks, 1997). In multiple sclerosis, pendular nystagmus may be a sign of cerebellar nuclear involvement or result from optic neuropathy, but the most consistent finding on MRI is a lesion in the dorsal pontine tegmentum, perhaps affecting the central tegmental tract (Barton, 1993). In a study of 27 patients with acquired pendular nystagmus, MRI findings were characterized by multiple areas of abnormal signal with statistically significant ones occurring in areas containing the red nucleus, the central tegmental tract, the medial vestibular nucleus, and the inferior olive (Lopez, 1996). The abundance of abnormal MRI signals, predominantly in the pons but also in the midbrain and the medulla, suggests that large or multiple structural lesions may be required to elicit pendular nystagmus. Acquired convergence-induced pendular nystagmus may occur with multiple sclerosis (Barton, 1999) and we recommend neuroimaging (e.g., cranial MRI) for all unexplained cases of acquired pendular nystagmus (class III–IV, level B).
Other causes of acquired binocular pendular nystagmus include Pelizaeus-Merzbacher disease, mitochondrial cytopathy, Cockayne’s syndrome, neonatal adreno-leukodystrophy (a peroxisomal disorder), and toluene addiction (Kori, 1998; Maas, 1991; Trobe, 1991). Spontaneous horizontal pendular nystagmus in a patient with a surgically acquired perilymph fistula was found related to the heart rate and may have been caused by pressure transfer of blood pulses to the labyrinth (Rambold, 2001a). Congenital, familial, or acquired bilateral paralysis of horizontal gaze may be associated with pendular nystagmus; the familial type may also be associated with progressive scoliosis and facial contractures with myokymia. Pendular nystagmus may also appear with blindness or monocular loss of vision; in the latter case, it may be monocular (see above). Binocular visual loss may cause nystagmus that has both horizontal and vertical components that change direction over seconds or minutes (i.e., a wandering null point) (Good, 1990). Blind patients may have windmill nystagmus, in which there are repeated oscillations in the vertical plane alternating with repeated oscillations in the horizontal plane.
Horizontal pendular pseudonystagmus has been described in patients with horizontal essential head tremor and bilateral vestibular dysfunction (Bronstein, 1992; Verhagen, 1994). The deficient vestibulo-ocular reflex results in ocular oscillations in space when the head oscillates, and funduscopy reveals a fine pendular motion of the eyes that is reduced by firm support of the head. The oscillopsia improves with treatment of the tremor with propranolol. Yen et al described two renal transplant patients who developed pseudonystagmus and oscillopsia caused by immunosuppressant (tacrolimus)-induced head tremor and gentamicin-induced vestibulopathy (Yen, 1999). Although the patients were initially thought to have nystagmus, closer observation revealed no true nystagmus but corrective saccades compensating for an absent vestibulo-ocular reflex during the head tremor (pseudonystagmus). Typically patients with vestibulo-ocular impairment have only head movement–induced oscillopsia, but these patients had constant oscillopsia because the visual tracking system (smooth pursuit) could not compensate for the loss of vestibular function at immunosuppressant-induced head oscillation greater than 1 Hz. Vestibular rehabilitation helped one of these patients.
Palatal myoclonus is a continuous rhythmic involuntary movement of the soft palate that may be accompanied by synchronous movements of other adjacent structures, such as the face, pharynx, larynx, or diaphragm. The association of pendular nystagmus with palatal myoclonus is not infrequent, and the condition is then termed oculopalatal myoclonus or oculopalatal tremor (Eggenberger, 2001; Talks, 1997). Oculopalatal myoclonus may be of two types (Nakada, 1986):
1. A lateral form, consisting of jerky, nystagmoid movements with simultaneous oblique and rotatory components associated (and synchronous) with lateralized palatal myoclonus (in this form, the eye on the side of the myoclonus intorts as it rises and extorts as it falls, whereas the opposite eye extorts as it rises and intorts as it falls).
2. A midline form in which vertical to-and-fro pendular eye movements occur synchronous with symmetric bilateral palatal myoclonus.
Oculopalatal myoclonus involves vestibulo-ocular reflex adaption mediated by the cerebellar flocculus, and floccular integrity is preserved inmost patients (Nakada, 1986). The lateral form implies unilateral disease, whereas the midline form indicates bilateral disease. Damage to the dentatorubro-olivary pathways (Guillain-Mollaret triangle) is found in cases of oculopalatal myoclonus, which is most often caused by multiple sclerosis or vascular lesions of the brainstem. MRI often shows enlargement of the inferior olivary nuclei (Talks, 1997).
There may be an association between the one-and-a-half syndrome (see Chapter 14) and oculopalatal myoclonus (Wolin, 1996). In five patients with one-and-a-half syndrome and facial nerve palsy, oculopalatal myoclonus developed in 4 months to 3 years. Involvement of the facial nerve may predict subsequent development of oculopalatal myoclonus. Oculopalatal tremor may be associated with delayed (tardive) ataxia (Eggenberger, 2001).
The evaluation of the patient with pendular nystagmus depends on the clinical circumstances and associated neurologic findings. In patients with multiple sclerosis, the diagnosis is usually obvious by a history of remissions and exacerbations of neurologic signs and symptoms associated with abnormalities on neurologic examination, suggesting a disseminated process. Brainstem stroke or tumor is diagnosed by mode of onset of symptoms, associated neurologic signs and symptoms, and MRI. Ophthalmologic exam will reveal blindness as a cause for the nystagmus in some patients. MRI is warranted in all patients with palatal myoclonus (class III–IV, level B).
The neurotransmitters involved in pendular nystagmus are unknown, but cholinergic and GABA-ergic pathways may be involved. Anticholinergic agents have produced variable treatment results (Barton, 1994; Leigh, 1991). In a randomized, double-blind study, trihexyphenidyl improved only one of five patients with pendular elliptical nystagmus. In another double-blind study, intravenous scopolamine reduced nystagmus and improved vision in five patients (Barton, 1994; Jabbari, 1987). Isoniazid relieved nystagmus and oscillopsia in two of three patients with pendular elliptical nystagmus due to multiple sclerosis, but others have not found this drug to be helpful (Leigh, 1994; Traccis, 1990). Memantine (a glutamate antagonist) caused complete cessation of nystagmus in 11 of 14 patients with acquired pendular nystagmus due to multiple sclerosis (Starck, 1997). These 11 responders had fixation pendular nystagmus (i.e., nystagmus increased with fixation). A dramatic suppression of pendular nystagmus in a patient with multiple sclerosis was described after smoking cannabis, but not by taking orally administered capsules containing cannabis oil (Schon, 1999).
Although the mechanism of action of gabapentin is unknown, Stahl et al have measured the effects of this agent on vision and eye movements in acquired pendular nystagmus in two patients with multiple sclerosis and one with brainstem stroke (Stahl, 1996). An oral dose of 600 mg produced improvement of vision due to changes in ocular oscillations in all three patients. The drug was well tolerated and was continued at 900 to 1500 mg daily in divided doses with long-term benefit. All the patients reported useful visual improvement that enabled them to read, watch television, and recognize faces. In other studies, gabapentin improved acquired pendular nystagmus in 10 of 15 patients (Averbuch-Heller, 1997) and 3 of 8 patients (Bandini, 2001).
Several reports have suggested that injection of botulinum toxin either into selected extraocular muscles or into the retrobulbar space might be effective in the treatment of acquired nystagmus (Carruthers, 1995; Leigh, 1992; Repka, 1994; Ruben, 1994a,b; Talks, 1997; Tomsak, 1995). Leigh et al injected the horizontal rectus muscles of the right eye of two patients with acquired pendular nystagmus (Leigh, 1992). The treatment effectively abolished the horizontal component of the nystagmus in the injected eyes of both patients for 2 months. However, side effects including diplopia, ptosis, and worsening of the oscillopsia in the uninjected eye (attributed to plastic-adaptive changes in response to paresis caused by the botulinum toxin) limited the effectiveness of the treatment. In another study, botulinum toxin injection into the retrobulbar space of three patients with acquired pendular nystagmus abolished or reduced all components of the nystagmus (Tomsak, 1995). Again, side effects of the treatment seem to be the limiting factor. Others have reported variable improvement in visual function and oscillopsia with retrobulbar or horizontal recti botulinum injection, with transient ptosis the most common side effect (Ruben, 1994a,b). Repka et al injected 25 to 30 units of botulinum toxin into the retrobulbar space of six adults with acquired nystagmus (Repka, 1994). Each patient had subjective and objective improvement of distance visual acuity following injection with reduction of the amplitude but not the frequency of the nystagmus. Visual improvement lasted no more than 8 weeks but persisted for 6 months in two patients with oculopalatal myoclonus. The authors concluded that retrobulbar botulinum toxin injection may improve visual function for patients with acquired nystagmus and that improvement seemed to be longer for patients with oculopalatal myoclonus. Further studies on the safety and efficacy of botulinum toxin injection for acquired nystagmus are warranted (class IV, level U).
Lesions of the Guillain-Mollaret triangle are thought to induce cholinergic denervation supersensitivity of the inferior olive, which results in the oculopalatal myoclonus. Anticholinergic agents (trihexyphenidyl) have thus been tried effectively in four patients with palatal myoclonus without ocular involvement (Jabbari, 1987) and in one patient with vertical pendular nystagmus identical to that seen with oculopalatal myoclonus but without palatal involvement (Herishanu, 1986). Valproate and carba-mazepine have each been reported to reduce the nystagmus of palatal myoclonus. Finally, as noted above, the nystagmus in patients with oculopalatal myoclonus may be especially sensitive to retrobulbar botulinum toxin injection (Repka, 1994).
The evaluation and treatment of pendular nystagmus is outlined in Figure 17–4.
What Are the Causes of Binocular Symmetric Jerk Nystagmus?
Binocular symmetric conjugate jerk nystagmus may be divided into that which is present spontaneously and that which is induced (Burde, 1991). Spontaneous jerk nystagmus may be further divided into forms present in primary position and forms present predominantly on eccentric gaze.
Spontaneous symmetric conjugate jerk nystagmus that occurs in primary position may be predominantly horizontal, predominantly torsional, or predominantly vertical. Spontaneous symmetric conjugate jerk nystagmus in primary gaze that is predominantly horizontal includes congenital nystagmus (above), latent nystagmus (above), vestibular nystagmus, periodic alternating nystagmus, drug-induced nystagmus, and epileptic nystagmus. Spontaneous symmetric conjugate jerk nystagmus in primary gaze that is purely torsional is a form of central vestibular nystagmus. Spontaneous symmetric conjugate jerk nystagmus in primary gaze that is predominantly vertical includes upbeat nystagmus and downbeat nystagmus.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


