Nystagmus
Mitchell B. Strominger
NYSTAGMUS IS A rhythmic oscillation of one or both eyes. It can be transiently evoked voluntarily or be constantly present as a nonspecific sign of abnormality. Developmental, hereditary, or acquired anomalies of the eye and central nervous system can all be associated with nystagmus.
HISTORY
When patients with nystagmus are evaluated, the history is extremely important to determine the etiology. The history should detail when the nystagmus was first noted, if it has changed over time, is constant throughout the day, changes depending on visual attentiveness, or is associated with a face turn or head movement. The prenatal history is explored for intrauterine infections, especially toxoplasmosis or rubella. A maternal history of anticonvulsant or psychogenic drug use, or gestational diabetes may suggest optic nerve hypoplasia (ONH). The birth history is directed towards prematurity, hypoxic ischemic encephalopathy, intraventricular hemorrhage, hydrocephalus, or developmental delay.
The family history gives information as to a possible hereditary factor. A family history of night blindness or color deficiency suggests congenital stationary night blindness (CSNB) or achromatopsia. For the latter condition, the family history may be especially important, because not every child with achromatopsia shows photophobia in the first few months of life (1). The family’s ethnic background may suggest a metabolic condition, such as Tay-Sachs disease, or a lipofuscinosis.
EXAMINATION
Examination of the symmetry of the face, the position of the ears, dental anomalies, skin tags, and pigmentation is helpful in identifying a developmental syndrome or albinism. The visual acuity is tested binocularly first and then monocularly, at distance and near fixation, and with and without any idiosyncratic head position. In infants, the ability to fixate on and follow moving objects and the use of visual clues is noted. The ability to optically elicit ocular movements using an optokinetic nystagmus tape or drum should also be noted. In the absence of the latter, there is a high likelihood that vision is grossly defective.
The characteristic of the nystagmus waveform should be noted, although this can change during the first year of life (2). It is described by its plane, amplitude, frequency, and symmetry. The plane of oscillation may be principally horizontal, vertical, oblique, or rotary (torsional). The amplitude may be fine (less than 5 degrees), medium (5 to 15 degrees), or large (greater than 15 degrees). If the oscillations are of similar speed in either direction, it is classified as a pendular nystagmus. A nystagmus is considered jerk if there is a biphasic rhythm with a fast phase in one direction, followed by a slow phase in the opposite direction. The frequency should be noted as high, low, or in cycles per second (Hz). A slit lamp or ophthalmoscope can be used to magnify ocular movements. Electronystagmography allows a more exact and permanent objective recording.
The nystagmus is observed for an extended period to determine whether it regularly changes direction with time, suggesting periodic alternating nystagmus (PAN); if both eyes move conjugately; if the pattern changes with eye position; and if the frequency or amplitude varies. Nystagmus that remains horizontal on vertical gaze suggests infantile nystagmus syndrome (INS), fusion maldevelopment nystagmus syndrome (FMDS), PAN, or peripheral vestibular nystagmus.
Examination of the eye should detect any severe bilateral ocular abnormality such as anterior segment dysgenesis, congenital cataracts, or congenital glaucoma. The irides are examined for transillumination defects that would suggest albinism. The posterior pole is evaluated for abnormalities, such as cicatricial retinopathy of prematurity (ROP), retinoblastoma, or coloboma. A blunted foveal reflex suggests albinism. Finally, the optic nerve is examined for pallor, hypoplasia, or increased cupping.
A clinical dilemma arises when an ocular malformation either does not exist or is very subtle. Retinal conditions such as leber congenital amaurosis (LCA), achromatopsia, CSNB, and ocular albinism may be difficult to detect on clinical examination alone. In such cases, an electroretinogram (ERG) should be performed.
NYSTAGMUS ASSOCIATED WITH NEUROLOGIC DISORDERS
Convergence-Retraction Nystagmus
Variable bursts of sustained convergence and retraction of the eyes on attempted upgaze suggest a midbrain disorder. Co-contraction of all the extraocular muscles causes retraction with convergence because of the greater strength of the medial rectus muscles. In infants, one would suspect congenital aqueductal stenosis, in children a pinealoma or obstructive hydrocephalus, and in older adults a vascular accident in the tectal or pretectal area. Parinaud syndrome is convergence-retraction nystagmus in association with vertical eye movement palsies, pupillary abnormalities, lid retraction, and accommodative spasm (3).
Seesaw Nystagmus
Seesaw nystagmus is a unique vertical-torsional oscillation of both eyes in which one eye rises and intorts and its fellow eye falls and extorts. The disjunctive vertical movement alternates to provide the seesaw effect. This disorder may be congenital, but most patients have suprasellar tumors expanding within the third ventricle and compressing the brainstem. Acquired oscillopsia and bitemporal hemianopsia are associated findings (4). Other causes include a lesion in the lateral medulla or pons, syringobulbia, or severe vision loss (5).
Periodic Alternating Nystagmus
PAN is a horizontal jerk nystagmus in which the direction of the fast phase changes spontaneously and cyclically with an intervening neutral period. A typical cycle lasts 1 to 6 minutes. A sequence of jerk waveforms in one direction converts to a neutral period of pendular waveforms, followed by jerk waveforms in the opposite direction. Alternating head turns may accompany the jerk nystagmus periods. PAN appears to result from a spatial and temporal shift in the null zone (6). PAN usually remains horizontal in vertical gaze and is hypothesized to arise from an instability of the optokinetic-vestibular system. It may coexist with downbeat nystagmus, both of which suggest an abnormality in the caudal medulla (7). PAN was found on eye movement recordings of patients with idiopathic infantile nystagmus who had mutations on the FRMD7 gene on Chromosome Xq26 (NYS 1 locus) (8). Up to one-third of patients with albinism also demonstrate PAN (6). Acquired PAM occurs most commonly with disease involving the midline cerebellum. Inhibitory pathways that use gamma-aminobutyric acid (GABA) in the nodulus and uvula control the time course of rotationally induced nystagmus and therefore Baclofen, a GABA agonist, can be effective in its treatment (9).
Downbeat Nystagmus
Downbeat nystagmus is recognized by a deficit in downward pursuit whereby the eyes drift upward, and a corrective sac-cade returns the eyes to the primary position. It is maximal in downgaze, lateral gaze and when the head is erect or hyperextended. A rare congenital hereditary form has been identified that is usually self limited, and associated with good vision and a normal neurologic examination. A compensatory chin-down head posture is sometimes noted (10). More commonly, downbeat nystagmus is acquired and signifies an abnormality of the cerebellum (flocculus or paraflocculus). The commonest causes are cerebellar degenerations and structural lesions at the craniocervical junction such as Chiari malformation (Fig. 23.1). Alcohol, lithium, anticonvulsants, and thiamine, magnesium, and B12 deficiency may also give rise to this condition (11).
Upbeat Nystagmus
A vertical vestibular or smooth pursuit deficit similar in type but opposite in direction to downbeat nystagmus is thought to cause upbeat nystagmus, which may increase or convert to downbeat nystagmus with convergence. It may occur congenitally as a variant of congenital nystagmus (CN) with anterior visual pathway disease (12). Acquired forms occur with lesions of the brainstem (mainly the pontomesencephalic junction, rostral medulla, or caudal pons), cerebellar vermis, or after meningitis (13).
Peripheral Vestibular Nystagmus
Lesions of the labyrinth or eighth nerve cause a horizontal and rotary jerk nystagmus on lateral gaze opposite the side of the lesion. Vertigo may be marked, and tinnitus and deafness occur in concert. Visual fixation decreases
the intensity of the nystagmus and vertigo, which lasts minutes, days, or weeks. Central pathways eventually compensate even if the underlying cause remains. Common causes are Meniere disease, infectious or vascular disorders, and trauma (14).
the intensity of the nystagmus and vertigo, which lasts minutes, days, or weeks. Central pathways eventually compensate even if the underlying cause remains. Common causes are Meniere disease, infectious or vascular disorders, and trauma (14).
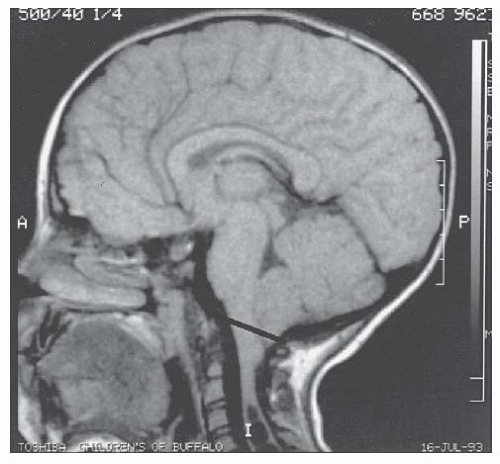 FIGURE 23.1. Arnold-Chiari malformation. Sagittal magnetic resonance imaging scan of type I Arnold-Chiari malformation with mild cerebellar tonsillar herniation below line. Note associated syrinx in cervical cord. |
NYSTAGMUS ASSOCIATED WITH VISUAL LOSS
Visual loss, or the lack of visual development, within the first 2 years of life is usually associated with nystagmus. Acquired monocular visual loss, due to an anterior visual pathway tumor or other ocular disorder, may be associated with a fine, rapid, monocular nystagmus (15). Nystagmus is usually not present in patients with cortical visual impairment because of the retention of visual input to the brain via the extrageniculostriate visual system.
Any congenital or perinatal condition that results in occlusion of the visual axis, distortion of the retinal image, or malformation of the sensory retina or optic nerve can result in nystagmus. Although electronystagmography may show complex or varied waveforms, the type of nystagmus is often related to the severity of the visual impairment. A moderate disruption in vision may result in pendular nystagmus, whereas a more severe form of the same disorder may produce a searching nystagmus. Although this may be helpful prognostically, some ocular malformations usually are readily recognized. The more common ocular malformations in which nystagmus may be a prominent sign include bilateral coloboma, congenital cataracts, congenital glaucoma, bilateral cicatricial ROP, aniridia, persistent fetal vasculature, bilateral retinal dysplasia, and congenital toxoplasmosis with macular involvement. Other abnormalities that may be more difficult to recognize and will be further discussed include Leber congenital amaurosis, optic nerve hypoplasia, albinism, achromatopsia, congenital stationary night blindness, and X-linked juvenile retinoschisis.
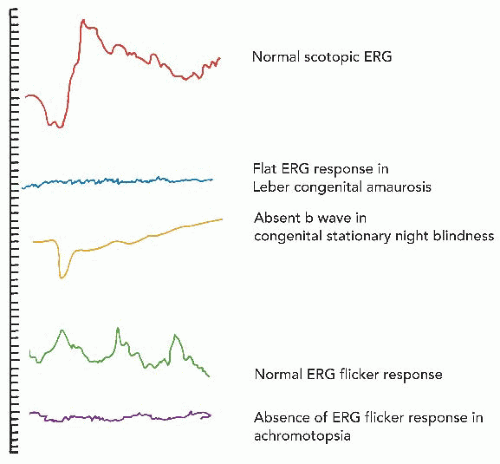 FIGURE 23.2. Electroretinographic findings in an infant with nystagmus. |
Leber Congenital Amaurosis
This autosomal-recessive disorder is characterized by diminished vision starting at or shortly after birth and can be divided into eleven subtypes depending on gene locus and defect. LCA2 results from RPE65 (retinal pigment epithelium-specific 65 KDa) deficiency that disrupts the retinoid cycle. Recent studies of subretinal gene therapy using recombinant adeno-associated virus to carry the RPE65 gene have shown promising results (16).
Acuity is less than 20/200 in up to 95% of affected individuals, and a searching nystagmus is present in 75%. The pupils are poorly reactive, and many children exhibit the oculodigital sign (habitual eye rubbing). The fundus is usually normal in infancy. Pigmentary disturbances of the peripheral retina develop during childhood in most patients, along with optic disk pallor and arteriolar attenuation. A markedly reduced or absent response to the ERG is noted in virtually all patients (Fig. 23.2). A variety of ocular conditions, including keratoconus, keratoglobus, macular coloboma, disk edema, cataract, and strabismus, have been associated with LCA. As many as 15% of patients may have mental retardation. Other systemic associations include medullary cystic kidney disease, cardiomyopathy, and skeletal abnormalities.
Optic Nerve Hypoplasia
Optic nerve hypoplasia (ONH) is a congenital, nonprogressive condition characterized by a paucity of axons within the optic nerve and a diminished ganglion cell layer of the retina. Ophthalmoscopically, ONH is recognized by a small, pale nerve head. Classically, it is surrounded by a ring of white sclera and a second pigmented or nonpigmented ring outlining the scleral rim, giving rise to the term double-ring sign (Fig. 23.3). The retinal vessels usually appear relatively normal, but the retina may be deep red in color because of the thinness of the nerve fiber layer.
Severe bilateral ONH results in a searching nystagmus, whereas mild, unilateral ONH may not have visual symptoms. In one study, 78% of those with bilateral involvement, poor vision, and nystagmus had additional ocular abnormalities, compared with 21% of patients with unilateral ONH (17). Delayed development is the most frequent nonocular disorder, followed by hypopituitarism, cerebral palsy, and epilepsy. Other associations include midline facial defects and abnormalities of the cerebral cortex, brainstem, and cerebellum including absence of the septum pellucidum and agenesis of the corpus callosum (18




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
