26

Nursing Care for Outpatient
Endoscopic Sinus Surgery
Modern treatment of paranasal sinus diseases has undergone significant advancement over the past decade. Contemporary techniques and endoscopic sinus surgery, with its specially trained personnel and specialized instrumentation, are ideally suited for the outpatient surgery center because of the relatively short anesthesia and generally overall good health of the patients. Although some patients still require an inpatient setting for their surgery because of significant medical problems, especially uncontrolled asthma, the rhinologist has become generally comfortable operating in ambulatory facilities that have become the mainstay site for this type of surgery.
Effective and safe outpatient ESS relies significantly on appropriate case selection, preoperative teaching by experienced personnel, and proper surgical instrumentation. In addition to an experienced surgeon, a well-trained surgical team whose members are familiar with ESS ideally includes the surgical nursing staff in charge of instrumentation and the patient in the operating room, the anesthesia team, pre- and postoperative nurses who manage the patient before and after surgery, and a nurse from the surgeon’s office who coordinates office activity with ambulatory surgical facility.
 Preoperative Evaluation
Preoperative Evaluation
As with most other outpatient surgical procedures, patient selection and preparation take place during the initial surgical consultation. Patients with significant medical problems, especially cardiac or pulmonary disease, may not be candidates for outpatient surgery or may require special preoperative assessment by primary care physicians, medical subspecialists, and/or anesthesiologists well in advance of the planned surgery. This assessment may preclude surgery in an ambulatory surgical facility.
Another group of patients who should not be treated in an ambulatory facility are those with intracranial or intraorbital complications of sinusitis who will require monitoring of their disease complications and sequelae by skilled nursing personnel, often in intensive care or step-down observation units.
Endonasal and paranasal tumors should be biopsied endoscopically in a surgical suite. Although biopsy of these tumors is usually performed successfully in the outpatient setting, definitive excision is often reserved for an appropriate inpatient facility.
A history of previous surgery and intraoperative problems should be obtained. Past experiences of severe nausea and vomiting following anesthesia should be noted. Family history of bleeding problems and atypical anesthesia events should be obtained.
 Preoperative Teaching
Preoperative Teaching
Ideally, postsurgical instructing should begin during the preoperative office visit. Written material that details the operative recovery period and provides answers to many of the most commonly asked questions and concerns for postsurgical sinus patients is provided to the patient by the physician, nurse clinician, and/or surgery scheduling personnel well in advance of the proposed surgery date (Fig. 26–1). This provides the patient ample opportunity to review this material and to share it with others who will assist in providing care following surgery. Clinical staff should be available to answer questions that may arise from this material. For selected patients, the process of informed consent is reinforced by use of videotape education materials such as “Functional Endoscopic Sinus,” produced by the American Academy of Otolaryngology Head and Neck Surgery.
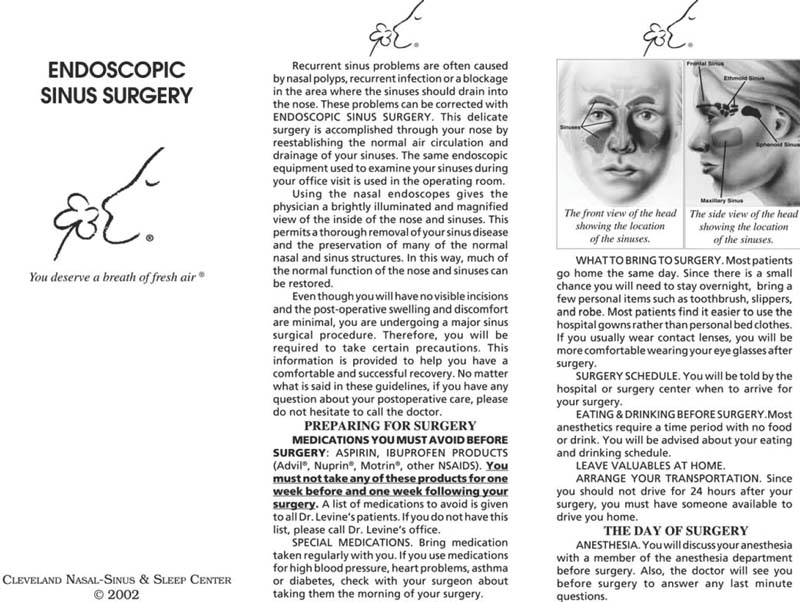
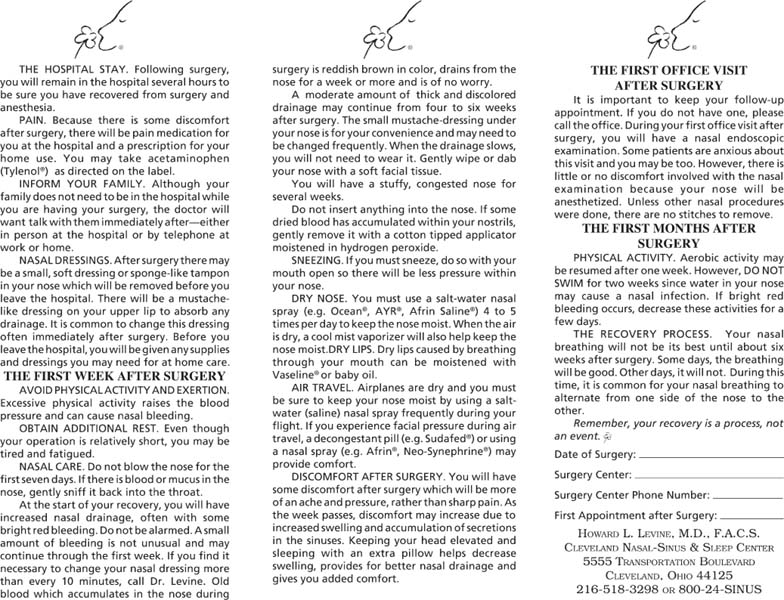
FIGURE 26–1 The patient brochure containing preoperative and postoperative instructions.
Specific instructions are provided to patients regarding the avoidance of aspirin, nonsteroidal anti-inflammatory drugs, certain vitamin and herbal medications, and anticoagulants for 2 weeks prior to surgery. An updated list of these medications should be kept by physicians, nurses, and surgery-scheduling personnel to minimize the risk that these medications are used by patients prior to surgery. This list should also be made available to each patient.
Successful preoperative teaching also necessitates instructing patients about their recovery period. Each patient is informed that several visits are required following surgery for removal of any intranasal dressings and debridement of eschar and exudate that are nearly always present following surgery. Patients may be advised to take pain medication ½ hour prior to each visit. They may choose to be accompanied by a friend or relative who is responsible for transportation should they feel the need. Patients must understand that significant resolution of their sinus symptoms may not occur until 6 to 8 weeks following surgery. They are informed that “recovery is a process, not an event.”
The authors generally use a nasal and sinus outpatient facility consisting of a freestanding ambulatory surgery center that is part of a larger group of independent office suites. This building also has CT scanning equipment and laboratory facilities in association with a designated presurgical testing area. After patients have had the opportunity to schedule their procedure with the surgical scheduling staff, they are directed to the testing area for the appropriate preadmission testing.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


