16
Normal Vocal Fold Vibratory Amplitude and Mucosal Wave
 Amplitude of Vibration
Amplitude of Vibration
Amplitude of vibration can be defined as the extent of lateral movement of each vocal fold during phonation. It is judged as the displacement of the medial edge of the vocal fold from its position at the closed phase of the vibratory cycle to its position at the maximal open point of the cycle. Amplitude of vibration is judged separately for the right and left vocal folds.
The term glottal width has been used to describe a phenomenon with characteristics that overlap those of amplitude of vibration. Glottal width, however, does not look at the right and left vocal folds individually. It is defined as the size of the largest opening between the vocal folds during the vibratory cycle and depends on the extent of lateral movement of both vocal folds.
In perfect vocal fold vibration, glottal width and amplitude of vibration should provide the same information. In that scenario, the glottal width should be twice the vocal fold amplitude of one vocal fold because the amplitude of vibration for each vocal fold is equal. However, if the vocal folds are not moving symmetrically (at the same time), these two parameters may be different. For example, if the right vocal fold reaches the maximal open point prior to the left vocal fold, yet both vocal folds move the same distance, the glottal width would be smaller than normal whereas the amplitude of vibration for each vocal fold would still be normal. In a clinical situation, amplitude of vibration combined with an assessment of vibratory symmetry is better at defining the extent of vocal fold excursion than either measurement alone, because it takes into account the difference in both timing and extent of movement between the two vocal folds. For many research experiments, the specifics of the extent of movement of the right versus the left vocal fold are not of interest, and the pertinent information is the glottal area available for outward flowing air. However, because the amplitude of vibration is more commonly used in a clinical setting and is related to vocal quality, we will confine our discussion to amplitude of vibration.
The amplitude of vibration depends on the pliability of the vocal fold tissues, the subglottal pressure, and the force of medial compression. These factors can either increase or decrease the amplitude of vibration. Increased tissue pliability increases the amplitude of vibration because pliable tissues are more easily displaced by the force of the outflowing air. Tissue that is less pliable requires stronger airflow to move it the same distance that more pliable tissue moves with a weaker airflow. In situations of stable tissue pliability, increased subglottal pressure results in larger amplitudes of vibration, whereas decreased subglottal pressure results in smaller amplitudes of vibration. Increased subglottal pressure can occur in two ways: (1) by increasing the volume of air exhaled and (2) by increasing the medial compression of the vocal folds. Medial compression of the vocal folds occurs secondary to increased laryngeal muscular contraction. During normal phonation, there is a relationship between subglottal pressure and medial compression. Increased medial compression results in an increased resistance to airflow through the glottis and requires that increased subglottal pressure be generated to overcome that resistance, thus initiating and maintaining vocal fold vibration. To produce a typical amplitude of vibration, the medial compression and subglottal pressure need to be carefully balanced. Increasing medial compression, without a substantial increase in breath support, generally produces smaller amplitudes of vibration. In addition to the physiology of producing a habitual voice, other typical voice changes such as a pitch increase or decrease or a change in loudness also are linked to changes in the amplitude of vibration (Video Clips 5 and 6).
High-pitched phonation is associated with smaller amplitudes of vibration, and conversely, low-pitched phonation is associated with larger amplitudes of vibration (Video Clip 5). Clinicians should expect smaller amplitudes of vibration in high-pitched phonation as a result of a decrease in the availability of pliable tissue. This phenomenon is mediated by the stretching action of the cricothyroid muscle on the vocal folds. The cricothyroid muscle pulls the vocal folds anteriorly and medially, making them taut, and, as this happens, the tension on the vocal fold tissues increases and lateral movement is impeded. In lower-pitched phonation, the thyroarytenoid muscle relaxes and decreases the tautness and tension on the vocal fold tissues. This allows the vocal fold tissues to easily move laterally in the outflowing air and results in amplitudes of vibration that are larger than those seen with habitual pitch and loudness.
This principle holds true for vocally normal speakers voluntarily increasing or decreasing the pitch of their phonation and should not be applied to persons with voice disorders that cause high- or low-pitched phonation. One can expect this relationship between pitch and amplitude of vibration to be altered with certain types of vocal fold pathology. A key example of the difference can be found in persons who have a low-pitched voice due to vocal fold edema. These individuals may demonstrate a smaller than normal amplitude of vibration, rather than the larger amplitude expected with low pitch, because there is expansion of the tissues with fluid. The fluid under the vocal fold mucosa makes it taught and thus prevents the mucosa from “blowing in the wind” of the exhalation.
The relationship between amplitude of vibration and loudness is not as clear as that of amplitude of vibration and pitch. Loud phonation is mediated by high subglottal pressure (Video Clip 6). As discussed above, there are two ways to increase subglottal pressure. These two ways have different effects on the amplitude of vibration. If one phonates loudly by increasing the volume of expired air, as we hope one would, then the amplitude of vibration increases relative to the increase in loudness of the individual’s speech. However, if phonation is made louder by increasing medial compression of the vocal folds rather than by increasing expiratory volume, then the amplitude of vibration is restricted by the muscular contraction. Clinicians need to evaluate the method of increasing loudness in their patients prior to judging the normalcy of the change in the amplitude of vibration with changes in loudness. If it is difficult to determine the role of medial compression on the amplitude of phonation after eliciting a natural loud phonation, further instructions regarding the production of loud phonation can be given to the patient. Most patients can easily be instructed to take a larger than normal breath prior to a loud phonation, which should result in an appropriate sample of phonation upon which to judge increased amplitude.
Luckily, softer phonation is less complicated with regard to the amplitude of vibration. Softer phonation is associated with smaller amplitudes of vibration due to the smaller force of the exhaled air on the vocal fold tissues. One should remember that this discussion regarding amplitude of vibration holds true for vocally normal speakers voluntarily increasing or decreasing the volume of their phonation and cannot be applied to persons with voice disorders that cause loud or soft phonation. An example of the difference between vocally normal speakers and those with a voice disorder can be found in persons who have a soft voice due to vocal fold atrophy (Video Clips 16 and 17). These persons may have larger than normal amplitude of vibration as there is less tension on the vocal fold tissue to impede the mucosa from moving laterally by the force of the exhaled air (Video Clip 24). It is important to remember that what causes a loud or soft voice in persons without voice disorders may be very different than what causes it in persons with voice disorders.
Amplitude of vibration is judged during stroboscopy of phonation at a normal pitch and loudness. Amplitude of vibration should also be judged during high- and low-pitched phonation and during loud and soft phonation to ensure that the changes in amplitude, which we may expect from our knowledge of physiology, do occur. Given that amplitude of vibration is judged at the relatively short open phase of the vibratory cycle, we need stroboscopy, kymography, or high-speed videoendoscopy to be able to see this feature of vocal fold vibration.
Typical amplitude of vibration has been defined for stroboscopy by Bless et al. as one third the width of the visible portion of the vocal folds.1 In the clinic, a five-point scale of severely decreased, decreased, typical, increased, and severely increased is commonly used (Fig. 16.1). Quantitative measures of vibration amplitude are available when using high-speed videoendoscopy and the resulting kymography. Because of the restrictions of stroboscopy, measurements of vibratory features using stroboscopy are not accurate or reliable.
 Mucosal Wave
Mucosal Wave
The mucosal wave is the wave-like movement of the vocal fold cover (epithelium and superficial layer of the lamina propria) during vibration. An exact, agreed upon definition of mucosal wave is difficult to find, as there seems to be some disagreement among experts in the field. That being said, the mucosal wave is generally agreed to encompass the differential between the lower and upper margins of the vocal folds as can be seen during the closing phase of vibration. There is disagreement about whether the movement of the mucosa on the superficial aspect of the vocal fold during the closed phase of vibration should be included in the term mucosal wave, although many clinicians do include an evaluation of this movement in their assessment of the mucosal wave. Furthermore, there is an upward swelling or vertical motion of the mucosa prior to the opening phase that some have included in their definition of mucosal wave (Fig. 16.2; Video Clip 7).
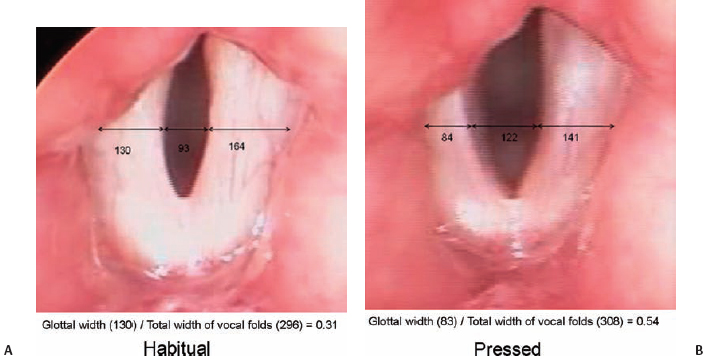
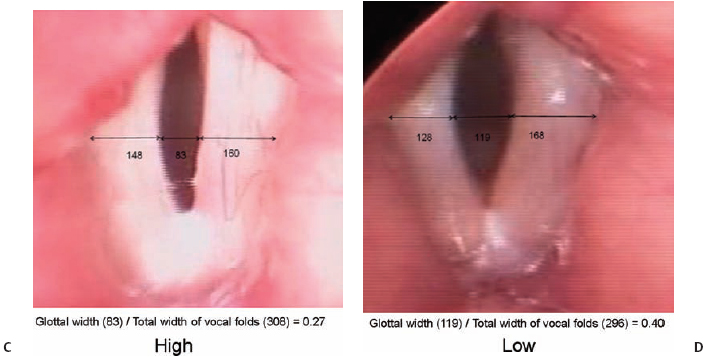
Fig. 16.1 (A) Amplitude of vibration measured from stroboscopic recordings of habitual pitch and loudness. Measures represent the number of pixels. The glottic opening is approximately one third of the total width of the superior surface of the vocal folds. (B) Amplitude of vibration measured from stroboscopic recordings of pressed phonation. During pressed phonation, the amplitude of vibration is approximately one half of the total width of the superior surface of the vocal folds. (C) Amplitude of vibration measured from stroboscopic recordings of high-pitch phonation. As the vocal folds are stretched and vibrate at a higher frequency, the amplitude of vibration decreases and is approximately one quarter of the total width of the superior surface of the vocal folds. (D) Amplitude of vibration measured from stroboscopic recordings of low-pitch phonation. At lower frequency of vibration, the amplitude of vibration is relatively larger, approximately 40% of the total width of the superior surface of the vocal folds.
The pliability of the vocal fold mucosa has been considered one of the most important endoscopic indicators of vocal fold health and is directly reflected by the characteristics of the mucosal wave. Furthermore, the mucosal wave depends on the ability of the superficial vocal fold tissues to vibrate independently from the deeper structures and requires that the relationship of the vocal fold histologic layers be in balance. (See Chapter 3 for a more indepth discussion of vocal fold histology.) The mucosal wave is therefore not just an indicator of the health of the superficial tissue. It also provides information regarding the underlying layers of the lamina propria and the thyroarytenoid muscle.
The mucosal wave can be impacted by not only the vocal fold anatomy but also by changes in the loudness and pitch of phonation. High-pitched phonation is associated with a smaller mucosal wave, and conversely, low-pitched phonation is associated with a larger mucosal wave. Clinicians should expect the mucosal wave to decrease when gliding from habitual to high-pitched phonation (Video Clip 5). This occurs with lengthening of the vocal folds due to contraction of the cricothyroid muscle. The superficial vocal fold tissues are placed on stretch at higher frequencies of vibration leading to a decrease in the amount of available movable tissue. The cricothyroid muscle acts like a person pulling on two ends of a rubber band: as the rubber band stretches, the rubber gets thinner. The reduction in mass of the vibratory portion of the vocal folds, which causes them to vibrate faster, also reduces the tissue available for production of the mucosal wave. The opposite is true for lower-pitch phonation. When a person purposefully phonates in a lower pitch, he or she relaxes the thyroarytenoid muscles and allows for an increase in pliable mucosa that can “blow in the wind” of exhalation.
Fig. 16.2 (A) The mucosal wave differential as captured via high-speed endoscopy. The white arrows indicate the width of the mucosal wave. (B) The mucosal superficial tissue wave as captured via high-speed endoscopy. The blackarrows indicate the position of the wave as it travels over the superficial surface of the vocal fold.
One thing to remember is that the above discussion regarding mucosal wave holds true for vocally normal speakers voluntarily increasing or decreasing the pitch of their phonation and should not be applied to persons with voice disorders that cause high- or low-pitched phonation. The same example used to illustrate this point for the amplitude of vibration can be applied to illustrate this point for mucosal wave. Persons who have a low-pitched voice due to vocal fold edema may have smaller than normal mucosal waves because there is fluid in the lamina propria tenting the mucosa of the vocal fold and preventing the mucosa from “blowing in the wind” of the exhalation. It is important to remember that what causes a high- or low-pitched voice in persons without voice disorders may be very different than what causes a low-pitched voice in persons with a voice disorder.
Louder phonation is associated with a larger mucosal wave, and conversely, softer phonation is associated with a smaller mucosal wave (Video Clip 6). Clinicians should expect an increased mucosal wave with louder phonation as a result of the build-up of greater subglottal pressure. The larger subglottal pressure is required to initiate and sustain vocal fold vibration in the presence of increased medial compression of the vocal folds mediated by the lateral cricoarytenoid, thyroarytenoid, and the interarytenoid muscles. Softer phonation is associated with less medial compression and less subglottal pressure. Thus, softer phonation does not have the physical properties that would create a larger mucosal wave.
Mucosal wave is judged with stroboscopy during phonation with a normal pitch and loudness. Mucosal wave should also be judged during high- and low-pitched phonation and during loud and soft phonation to ensure that the changes in mucosal wave, which we may expect from our knowledge of physiology, do occur. Given that the mucosal wave is generally defined as the differential between the lower and upper margins of the vocal folds, as can be seen during the closing phase of vibration, we need stroboscopy, kymography, or high-speed videoendoscopy to be able to see the mucosal wave.
A typical mucosal wave has been defined for stroboscopy by Bless et al. as a differential that is as wide as one-half of one of the vocal folds.1 In the clinic, a five-point scale of severely decreased, decreased, typical, increased, and severely increased is commonly used. There are some clinics and researchers that use a six-point scale of 0 = typical mucosal wave to 5 = absent mucosal wave. Given the valuable information available from larger than typical mucosal waves, there may be a benefit to evaluating mucosal wave as being typical, larger than normal, or smaller than normal. Currently, there are no clinically viable quantitative measures of mucosal wave.
 Conclusion
Conclusion
Amplitude of vibration and mucosal wave tend to vary in a similar pattern as they are mediated by similar factors such as medial compression, subglottal air pressure, and tissue pliability. During an endoscopic examination, it is helpful to make sure that there is a rationale for similarities and differences in how the amplitude of vibration and mucosal wave are varying. Because amplitude of vibration and mucosal wave can vary with pitch and loudness, it is quite important to ensure that the phonation being evaluated under endoscopy is of habitual pitch and loudness. One particular consideration is the tendency for some persons to increase pitch and loudness when phonating with a rigid endoscope in their oral cavity. Additional samples of purposefully produced high- and low-pitched phonation and loud and soft phonation are helpful in evaluating and understanding the phenomena associated with amplitude of vibration and mucosal wave.
Reference
1. Bless DM, Hirano M, Feder RJ. Videostroboscopic evaluation of the larynx. Ear Nose Throat J 1987;66: 289–296
Additional Suggested Reading
Hirano M, Bless DM. Videostroboscopic Examination of the Larynx. San Diego, CA: Singular; 1993
Poburka BJ. A new stroboscopy rating form. J Voice 1999;13:403–413
Shaw H, Deliyski D. Comparison of glottal configuration and glottal width recorded with stroboscopy and high-speed videoendoscopy in normophonic speakers. Presented at: 36th Symposium of The Voice Foundation: Care of the Professional Voice; June 2007; Philadelphia, PA
Shaw HS, Deliyski DD. Mucosal wave: a normophonic study across visualization techniques. J Voice 2008; 22:23–33
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


