4 ![]()
Definition
What Is Normal Tension Glaucoma?
Normal tension glaucoma (NTG) is a progressive optic neuropathy that mimics primary open-angle glaucoma (POAG) but lacks the findings of elevated intraocular pressure (IOP) or other mitigating factors that can lead to optic neuropathy. It includes the findings of normal angles on gonioscopy, cupping of the optic nerve, and visual field loss correlating with the cupping and may show progressive damage of the nerve. It is believed to have other influencing factors such as vascular and genetic.
Epidemiology and Importance
How Common Is NTG?
Klein et al1 found the incidence of NTG in the Beaver Dam Eye Study to approach 33%. In Asian populations, such as in Japan, as the patient’s age increases, there is a decrease in average IOP, resulting in a higher percentage of glaucoma patients falling into the normal tension group.2 In fact, as much as two-thirds of the glaucoma in Japan may fall into the category of NTG.3
What Are the Demographic Characteristics of NTG?
Different studies show varying results in evaluating the occurrence of NTG among men and women. Levene3 found in his review that there were more women with NTG, but the Beaver Dam Eye Study1 showed no predilection for either sex. With women having a longer life span, it may be understandable to see more females with NTG (along with other chronic disorders).
Are There Any Genetic Characteristics of NTG?
With regard to inheritance, Werner4 found cases of POAG and NTG within the same family. Miglior5 and Geijssen6 also showed a predilection for several members of the family having NTG. It would be judicious to suggest that other family members not already evaluated be examined by an ophthalmologist.
What Role Does IOP Play in NTG?
Although IOP is generally normal (10–21 mm Hg), several studies include 22 to 24 mm Hg in NTG. The collaborative normal tension study had 24 mm Hg as the upper limit.7 Kamal and Hitchings8 cite a mean IOP of less than or equal to 21 mm Hg, with no more than a single reading of up to 24 mm Hg as still indicative of NTG.
Crichton et al9 found that a 2 mm Hg or greater difference in IOP correlated with greater visual field loss in the eye with the higher pressure; 13 of 47 patients with NTG in this study had asymmetric IOP of 1 ≥ mm Hg. However, many patients with asymmetric visual field loss showed symmetric IOP. Crichton et al allowed an IOP of ≤23 mm Hg to define NTG in this study.
Araie et al10 found a correlation between IOP and visual field progression in this study of 56 eyes. However, Levene’s3 review in 1980 did not find convincing evidence that IOP played a role in NTG. Another study discussed under the treatment of NTG show that lowering IOP helps to slow if not halt progression.7
What Role Might Blood Flow Play in NTG?
Aside from IOP, blood flow in the NTG patient has held a fascination for many researchers. The idea that abnormal blood flow, intermittent or persistent, leads to decreased profusion of the optic nerve, which results in ischemia and decreased nutrition, has been postulated as a significant etiologic factor in the pathogenesis of NTG. Increases in the incidence of migraine and vasospasm in patients with NTG has been investigated by Phelps and Corbett.11 Drance and his colleagues12 showed that capillary flow in the fingers of NTG patients was decreased, and this evidence offered vasospasm as a possible causative factor in NTG. Others have found increased vascular resistance by carotid Doppler imaging (CDI) in patients with NTG.13 Netland et al14 and Kitazawa et al15 found some patients with NTG had less progression if they were on systemic calcium channel blockers. This finding led both groups to suggest that vasoregulation in NTG might be abnormal. Flammer16 felt that calcium channel blockers had a role in controlling vasospasm (seen in narrow bed capillary blood flow) and potentially stabilizing the disease process.
It has been shown that NTG patients, more so than other patients, may be more susceptible to vasodilators such as carbon dioxide.17 Pullinat et al17 went on to suggest that this was due to an already-present predisposition to vasoconstriction in patients with NTG.
Hayreh et al18 suggested in 1994 that episodes of nocturnal hypotension might explain the progressive optic nerve damage and visual field loss in patients with NTG despite normal IOP. They found that these patients had a deeper drop in nighttime blood pressure than in patients with POAG. They went on to postulate that these patients might be more prone to progression if their blood pressure was aggressively treated. Graham and associates19 found more progression in NTG and POAG patients if they had a lower nocturnal blood pressure.
Meyer et al20 compared 20 NTG patients with 20 normal patients. Blood pressure was monitored over 24 hours at 20-minute intervals during the day and 40-minute intervals during the night. They found a significant blood pressure drop in many patients, which was more pronounced in the normal tension patients versus the controls. This drop was thought to have a role in the pathogenesis of NTG.
Fontana et al21 investigated pulsatile ocular blood flow (POBF) in normal and NTG patients. They found that the POBF was lower in the normal tension group. They also found that if there was asymmetry between the two eyes of an NTG patient, there was a higher incidence of unilateral visual field loss in the eye with the lower blood flow. James and Smith22 evaluated 29 normal patients and 22 NTG patients and also found lower POBF in the normal tension group. Peripapillary retinal blood flow in NTG was investigated by Chung and associates,23 who found that the normal tension group compared to controls had a larger area of reduced blood flow in the peripapillary area. They felt that this could contribute to retinal ganglion cell death and progression of disease.
What Other Findings May Be Present in Patients with NTG?
Carter and associates24 looked at laboratory findings in patients with high tension glaucoma, NTG, and controls. No significant difference was seen between the three groups with regard to coagulation factors, cholesterol, high-density lipoprotein, low-density lipoprotein, triglycerides, and hemoglobin A1C. Plasma viscosity was also shown to be similar in these three groups.
Wax et al25 have investigated the presence of autoimmune antibodies and their potential relationship to glaucoma, especially NTG. Antibodies to retinal proteins were found in higher concentrations in patients with NTG compared to controls. Deposition of these compounds were found in the layer of retinal ganglion cells and in the inner nuclear and outer nuclear layers. The authors hypothesized that these antibodies could have a role in apoptosis. Romano et al26 published a study showing that the concentration of anti-rhodopsin antibodies in serum was elevated in patients with NTG. It has been shown that stress can cause an increase in heat shock proteins, which are neuroprotective by design, but are also antigenic. The resultant antibodies to these heat shock proteins may have the potential to allow damage to occur.27 Wax et al25 found 12% of the NTG patients in the study exhibited an increased level of monoclonal gammopathies, leading them to suggest a similarity to patients with progressive peripheral neuropathies associated with monoclonal paraproteinemia.
Cartwright and Anderson28 reported a 30% prevalence of autoimmune disorders by epidemiologic criteria in patients with NTG. The prevalence of immune-related disorders may have been a factor in the vascular system, making vasospasm or constriction potentially more serious in this group of patients.
Diagnosis and Differential Diagnosis
What Are the Findings in NTG?
Cupping of the optic nerve is often the first finding to suggest NTG. Optic nerve cupping is generally similar to that seen in open-angle glaucoma. The existence of cupping specific to NTG is debated. Some investigators feel that cupping in NTG has more severe slopes,29 with visual field loss exceeding the degree of cupping, but no definitive study has substantiated this theory.3
The amount of peripapillary atrophy may also influence vision according to the work done by Park and associates.30 Tezel et al31 compared patients with NTG, ocular hypertension, and POAG, looking for disc changes characteristic for each group. Noting more nerve loss, this research has suggested that the NTG patients may have presented later in their course. Miller and Quigley32 found no difference between NTG patients, POAG patients, and controls. These physicians found what they felt was a difference in the lamina cribrosa’s structure that possibly could be a factor in the etiology of NTG. Geijssen and Greve33 divided NTG into three groups: myopic, focal ischemic, and senile sclerosis. Their work suggested that the prognosis varied with each group.
Disc hemorrhages have also been linked to NTG; however, several studies have lessened this tie.31,34 Although it is generally agreed that a disc hemorrhage is evidence of future nerve fiber drop out, it is not specific for patients with NTG.35 Seigner and Netland36 described the prognostic value of optic disc hemorrhage in glaucoma, where a disc hemorrhage is interpreted as an indicator of uncontrolled glaucoma.
Topography of the optic nerve in patients with NTG has been investigated for characteristics possibly specific to this entity. Compared to the findings in 50 NTG patients and patients with POAG, disc parameters gathered with the scanning laser tomographic technology (Heidelberg retinal tomography, HRT) showed no significant difference between the groups.37 Although disc differences between patients with glaucoma were different from the controls and from the patients with ocular hypertension, no distinction was found between the groups with pathology (POAG and NTG).
Stroman et al38 looked at optic nerve characteristics from magnetic resonance imaging (MRI) studies; 20 controls and 20 patients with NTG showed no statistical difference between the groups. There was a significant increase in the incidence of small-vessel ischemia in the NTG patients, but this group was also older than the controls (73 years old vs. 67 years old, respectively).
What Are the Visual Field Findings in NTG?
Visual field loss generally occurs similar to that seen in POAG.39 However, it may appear more advanced than the amount of cupping of the nerves seen on examination.21 Levene3 and Greve and Geijessen40 separately felt they found significant variations in visual field loss in patients with NTG. Defects more closely threatening fixation, relatively deeper or steeper in slope, and perhaps more frequently superior in location have been spotlighted by these authors.
In a study by Poinooswamy et al,41 patients with NTG were noted to have defects in their visual fields that were more advanced than in patients with high tension glaucoma (over 21 mm Hg). Within the NTG group, the patients more often presented with unilateral visual field loss. The authors also found that the left eye of the normal tension group was more likely to have a defect present compared to the right eye. Overall, the frequency of unilateral field loss between the high tension group and the normal tension group was similar (21% and 25%, respectively). The authors noted that with increasing age, the frequency of unilateral field loss decreases. They concluded that progression of the disease is not unexpected.
Crichton et al’s9 study was similar in its conclusion that, with a 2 mm Hg or greater difference between eyes, a correlation was seen with more visual field loss in the eye with higher IOP. This research also found that in several cases of asymmetric visual field loss, there was symmetric IOP.
Caprioli and Spaeth42 showed that in NTG, one could find defects that were deeper, steeper, and closer to fixation. Levene3 also found that fixation was threatened more often than in patients with POAG. Caprioli et al43 compared visual field defects in POAG (high tension glaucoma) and NTG, and found that more diffuse loss was seen in younger patients with higher IOPs. In one study, 30% of 53 patients with unilateral NTG had visual field loss in the fellow eye within an average follow-up of 25 months.44 Furthermore, the loss in the second eye was often (75%) in the same region of loss in the first eye; 88% of the losses first appeared in the paracentral region, and, overall, 69% of the losses were superior in location. Araie45 showed no overall difference in the pattern of loss between normal tension and POAG patients.
How Should the NTG Patient Be Evaluated?
NTG is a diagnosis of exclusion. Taking the adage that “common things are common,” the physician should exclude other possible etiologies of optic nerve cupping with or without visual field loss. When NTG is suspected, a comprehensive history should be taken to rule out chronic anemia, cardiopathies, acute blood loss, episodes of systemic hypotension, decreased cerebral blood flow, blood dysplasias, and neurosyphilis.
A diurnal curve should be completed before the diagnosis of NTG is affirmed. Opinions vary as to the number of specific readings, but at least three readings (early morning, noon, mid- to late afternoon) should be required. To evaluate IOP one morning and again a few months later in the afternoon is totally inadequate.
The amount of cupping should be recorded by drawing or photography. Nerve layer topography or polarimetry of the nerve fiber layer may supplement, but at this time not replace, a drawing or stereo disc photographs. These newer technologies appear to have more value in monitoring the patient for change rather than in diagnosing glaucoma.46
Perimetry should be performed for baseline information. An automatic static threshold perimetric test is, at present, the state of the art. Because glaucoma (POAG or NTG) is a spectrum, the cupping can be abnormal or progressive before perimetric deficits appear. Therefore, the diagnosis of NTG does not require that a visual field defect be present. Blue-yellow perimetry may be of value in detecting visual field loss before standard white-on-white testing can elicit a loss of function.
With regard to radiologic studies, computed tomography (CT) and MRI studies in an asymptomatic patient have a very low yield for finding central nervous system abnormalities. Stroman and associates at the American Academy of Ophthalmology46 found a low incidence of intracranial lesions in patients suspected of having NTG (2 of 53 patients). This study also showed that diffuse small-vessel disease changes were more frequent in the NTG group. Based on this study, it seems that unless a patient presents with a visual field defect suggesting cerebral etiology or the patient shows progression despite apparently adequately reduced IOP (25–30%), radiologic studies need not be requested nor a neurologic consult sought.
Treatment and Management
In the face of progressive nerve cupping and/or visual field loss, the ophthalmologist should consider poor compliance and inadequate IOP control (Fig. 4–1). The physician must urge the patient to use the prescribed medication as directed. A diurnal curve should be performed to search for IOP spikes. After the data are gathered, changes in medications and surgery (laser or incisional) should be considered. Visual fields should be repeated to verify the consistency of new progression. Disc photos may need repeating to objectively compare with previous ones. The newer imaging techniques, such as HRT, scanning laser polarimetry, and ocular coherent tomography (OCT) may also have more of a role in detecting or verifying progression.
If no evidence of visual field loss accompanies a mildly increased cup-to-disc ratio, the ophthalmologist should examine siblings for the possibility of physiologic cupping. The physician may also choose to follow the suspicious patient, looking for progression, before instituting therapy.
It is my experience that most glaucoma patients prefer to try topical medications before moving on to surgery The collaborative NTG study group has shown that reducing IOP 30% or more slows the progression of this disease.7 It seems reasonable to set this as a goal for our patients. Although beta-blockers are the mainstay in the treatment of elevated IOP, it is often difficult to medically reduce the “normal” IOP with a single medication. Schuman et al47 have shown that many patients presently on a systemic beta-blocker may respond in a decreased manner to topical beta-blockers. Prostaglandin analogues and α-adrenergic agonists, along with topical carbonic anhydrase inhibitors (CAIs) may be better choices in this group of patients.47
Laser trabeculoplasty often helps to lower IOP in NTG, but may require adjunctive medications or itself be used as an adjunctive medication. Incisional surgery has also been successful in obtaining significant reductions in IOP. The ophthalmologist may also consider other methods of improving the situation, but not necessarily decreasing the IOP in patients diagnosed with NTG. Calcium channel blockers may help improve blood flow.14,15 Betaxolol has been shown to possibly have a similar mechanism of action in preserving visual field function while also lowering IOP.48,49 Neuroprotection or regulation of apoptosis may be a useful tool in the near future. Brimonidine (an α-adrenergic agonist) may have the ability to upregulate “survival” signals, based on experiments in animals.50–52
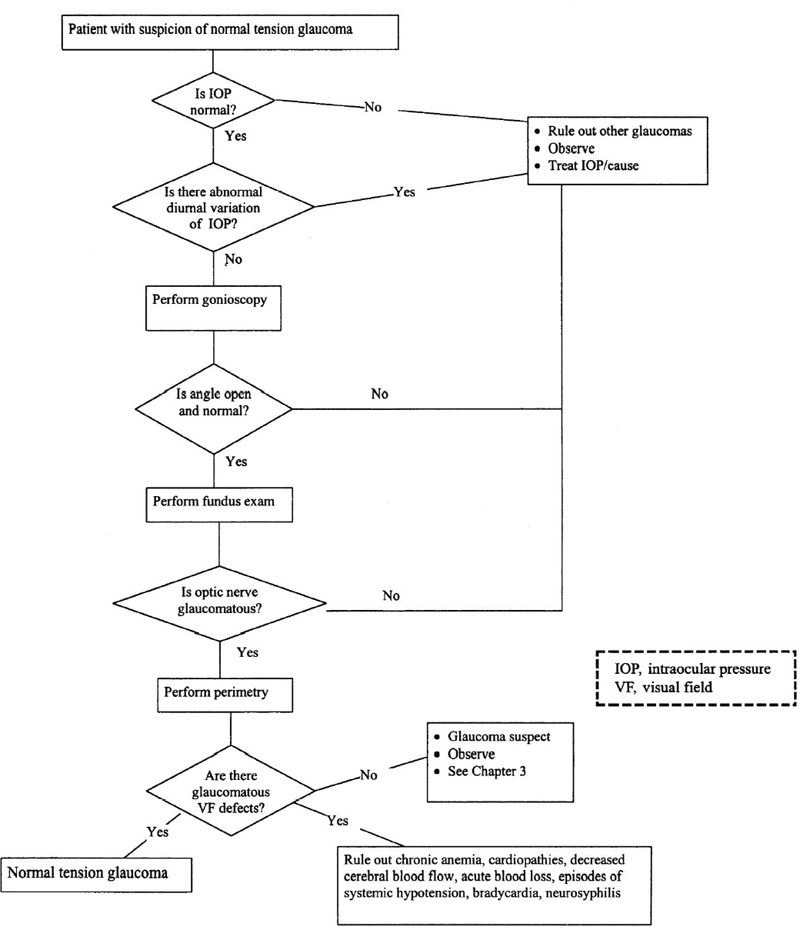
Figure 4–1. Management of a patient with suspicion of normal tension glaucoma.
Kamal and Hitchings8 reported that 24-hour blood pressure monitoring is used in their patients who worsen despite lowering of the IOP. They look for episodes of systemic hypotension and work with the patient’s family physician to try to minimize this, as well as to flatten out the diurnal variation of the IOP with topical medications.
Future Considerations
IOP that is not tolerated by the optic nerve will always be a major risk factor in glaucoma, regardless of type. Research into the factors causing “intolerable” IOP continues, with work being focused on the trabecular meshwork, immunologic status, genetic variables, blood flow, and apoptosis. Invariably, with further knowledge, distinctions between NTG and POAG will change, so that these two may become more distinct or more similar.
References
5. Miglior M: Low critical tension glaucoma: present problems. Glaucoma 1987;9:77.
6. Geijssen HC: Studies on normal pressure glaucoma, vol. 1. Amsterdam: Kugler, 1991;1.
16. Flammer J: Therapeutic aspects of normal-tension glaucoma. Curr Opin Ophthalmol 1993;4:58–64.
26. Romano C, Burnett DA, Li Z, et al: Anti-rhodopsin antibodies in sera from patients with normal-pressure glaucoma. Invest Ophthalmol Vis Sci 1995;36:1968–1975.
33. Geijssen HC, Greve EL: Vascular concepts in glaucoma. Curr Opin Ophthalmol 1995:6:71–77.
40. Greve EL, Geijessen HC: Doc Ophthalmol 1983;35:101.
52. Wen R, Cheng T, LiE Cao W, et al: α2-Adrenergic agonists induce basic fibroblast growth factor expression in photoreceptors in vivo and ameliorate light damage. J Neurosci 1996;16:5986–5992.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


