Nonsteroidal Anti-Inflammatory Drugs
Allan J. Flach
The term nonsteroidal anti-inflammatory drugs (NSAIDs) has been applied to clycooxygenase inhibitors (COIs) that are useful for the prevention and treatment of several commonly encountered ophthalmic syndromes and diseases. Topically effective preparations are commercially available as ophthalmic solutions that have been approved for use by the Food and Drug Administration (FDA) for more than two decades. Labeled indications include the inhibition of intraoperative miosis during cataract surgery, the treatment of ocular inflammation following cataract surgery, relief of ocular pruritis associated with seasonal allergic conjunctivitis and relief of pain and photophobia associated with refractive surgery. In addition, this group of drugs has been widely used by ophthalmologists throughout the world for the prevention and treatment of cystoid macular edema (CME) after cataract surgery. The purpose of this chapter is to summarize the status of topically applied NSAIDs. This effort will correlate the pharmacology and pharmacodynamics of NSAIDs with related advances in the medical sciences as reflected in laboratory and clinical studies, which is the goal and purpose of ophthalmic clinical pharmacology.1,2
CHEMISTRY
The NSAIDs currently available commercially represent a chemically heterogeneous group of compounds that can be divided into six different chemical classes: salicylates, fenamates, indoles, phenylalkanoic acids, phenylacetic acids, and pyrazolones. Individual members within respective groups are summarized in Table 1 and their structures are shown in Figure 1. NSAIDs is a term chosen to emphasize that drugs of this group have chemical structures that do not include a steroid nucleus derived biosynthetically from cholesterol. Aspirin, chemically known as acetylsalicylic acid, remains the most widely used NSAID throughout the world. However, it cannot be prepared in an aqueous delivery system because it is rapidly hydrolyzed to salicylic and acetic acids. Therefore, it is unstable in solution and is not available in other than solid dosage forms.3 Salicylic acid has anti-inflammatory activity, but it is too irritating for topical ophthalmic use. It is reserved as a keratolytic agent for dermatologic conditions such as psoriasis and warts. Similar to the salicylates, the fenamates and pyrazolones derivatives are considered too toxic for ocular application.4,5,6 Therefore, this chapter reviews the indoles, the phenylalkanoic acids, and the phenylacetic acids that are available as topical ophthalmic preparations.
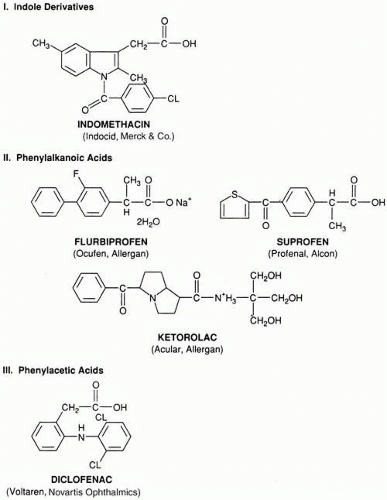 Fig. 1. Structures of nonsteroidal anty-inflammatory drugs. |
Most NSAIDs are weak acids with pKa values between 3 and 6. The unionized form of the molecule is associated with good lipid solubility providing good absorption from the stomach, upper gastrointestinal tract and permitting passage through the lipoidal corneal epithelium of the eye. Generally, pKa values are lower than the respective pH values of the extracellular environment, and, therefore, these drugs exist largely in their ionized forms. However, in a more acid environment, such as that produced by inflammation, the unionized form of drug is available to diffuse into cells. A pH change from 7.4 to 7.0 is accompanied by a 25% increase in the unionized form of the drug. Because the intracellular pH decreases less than the extracellular pH during an inflammatory process, the relatively alkaline environment provided inside the cells favors the ionized form of the drug trapping it within the cell. Thus, the pH difference favors increasing the NSAID intracellular concentration potentially enhancing therapeutic effects.7
The chemical structures of all of the NSAIDs incorporate at least one aromatic ring. The structures of indomethacin, diclofenac, and flurbiprofen include two aromatic rings that are twisted with respect to each other. A study of structure–activity relationships has helped determine the characteristics of at least one NSAID receptor.8 However, there are undoubtedly multiple receptors for NSAIDs with different structural requirements. Therefore, it is unlikely that the characteristics of any single proposed receptor as determined in vivo will explain the pharmacologic activity of this group of drugs.
Indomethacin is the first topically administered NSAID that found widespread use in ophthalmic clinical studies. However, it remains unapproved for use as an ophthalmic formulation in the United States. From a chemical viewpoint, it is the only indole derivative available. This drug is chemically known as 1-(4-chlorobenzoyl)-5-methoxy-2-methyl-1H-indole-3-acetic acid with the empirical formula of C19H16ClNO4 and a molecular weight of 357.80. Indomethacin is soluble in alcohol but insoluble in water. Initially, it was formulated in a solution of sesame seed oil.9 However, this eyedrop proved too irritating for patients. Therefore, the preparation currently available commercially in Europe and other parts of the world is a 1% indomethacin aqueous suspension (Indocid Ophthalmic Suspension; Merck, Sharpe & Dohme, West Point, PA).
The phenylalkanoic acids are water-soluble and, consequently, are easier to formulate as ophthalmic solutions. Flurbiprofen 0.03% (Ocufen Ophthalmic Solution; Allergan, Irvine, CA) and suprofen 1% (Profenal Ophthalmic Solution; Alcon, Ft. Worth, TX) are approved by the FDA for inhibition of intraoperative miosis. However, only flurbiprofen is commercially available. Flurbiprofen is chemically known as sodium (+/-)-2-fluoro-α methyl-4-biphenyl acetate dehydrate with a molecular weight of 302.3. Suprofen is α-methyl-4-(2-thienylcarbonly) benzene acetic acid with the empirical formula of C14H12O3S and a molecular weight of 260.3. It has not been available commercially for several years.
The third phenylalkanoic acid derivative, ketorolac tromethamine, is currently available as three different commercial preparations: the first approved 0.5% ophthalmic solution (Acular; Allergan), a preservative free 0.5% solution (Acular PF; Allergan) and a lower strength 0.4% ophthalmic solution (Acular LS; Allergan). Acular Ophthalmic Solution is approved for the treatment of postoperative inflammation in patients who have undergone cataract extraction and for the temporary relief of ocular itching caused by seasonal allergic conjunctivitis. Acular PF is indicated for the reduction of ocular pain and photophobia following incisional refractive surgery. Acular LS is approved for the reduction of ocular pain and burning/stinging following corneal refractive surgery. All of these preparations contain the same basic drug molecule ketorolac as a tromethamine salt and is known chemically as (+/-5-benzoyl-2,3-dihydro-) 1H-pyrrolizine-1-carboxylic acid with 2-amino-2-(hydroxymethyl)-1,3-propanediol(1:1). The molecular weight is 376.41 with the empirical formula of C19H24N2O6. It is formulated as tromethamine salt to provide ideal water solubility. Ketorolac exists as both S (-) and R (+) enantiomers and is marketed as the racemate. The S (-) enantiomer is approximately twice as active as an anti-inflammatory agent. Interestingly, and unlike other NSAIDs, the S enantiomer of ketorolac is levorotatory. Ketorolac’s enantiomers exhibit stereoselective pharmacokinetics.10
Diclofenac sodium 0.1% (Voltaren; Novartis Ophthalmics, East Hanover, NJ) is a phenylacetic acid derivative that is approved for use by the FDA after cataract surgery to inhibit postoperative inflammation and for the relief of pain and photophobia following refractive surgery. It is designated chemically as 2-((2, 6-dichloro-phenyl) amino) benzene acetic acid, monosodium salt, with an empirical formula of C14H10Cl2NO2. Its molecular weight is 318.14. It is freely soluble in methanol and sparingly soluble in water. This ophthalmic solution has the faint odor of castor oil.
PREPARATIONS
The FDA approves flurbiprofen 0.03% and suprofen 1% for use as inhibitors of intraoperative miosis. However, suprofen 1% (Profenal Ophthalmic Solution 1%, Alcon) has not been commercially available since 1998. Although flurbiprofen was initially distributed in 2.5 mL, 5 mL and 10 mL volumes, the FDA requested that Allergan remove all but the 2.5 mL volume from the market in an attempt to discourage its use for unapproved indications. Therefore, flurbiprofen is only available as 2.5 mL within a 6-mL bottle. This preparation, called Ocufen, contains 0.03% flurbiprofen sodium, 1.4% polyvinyl alcohol, 0.005% thimerosal, edetate disodium, potassium chloride, sodium chloride, sodium citrate, citric acid, and purified water with an adjusted pH of 6.0 to 7.0 and an osmolality of 260 to 330 mOsm/kg. The manufacturer recommends a total of four drops of solution, administered one drop approximately every half hour beginning 2 hours before surgery, for the inhibition of intraoperative miosis during cataract surgery. The preparation is supplied in a plastic dropper bottle and stored at room temperature (59°F to 75°F or 15°C to 25°C). Flurbiprofen is also available in generic formulation (flurbiprofen 0.03% ophthalmic solution, Bausch & Lomb, Rochester, NY).
Voltaren Ophthalmic Solution is approved for use in inhibiting postoperative inflammation following cataract surgery and for the temporary relief of pain and photophobia after refractive surgery. It is available in 2.5-mL and 7.5-mL volumes dispensed within 5-mL and 10-mL bottles, respectively. This preparation includes diclofenac 0.1%, boric acid, edetate disodium, polyoxyl 35 castor oil, purified water, sorbic acid, and tromethamine adjusted to a pH of 7.2. This ophthalmic solution is supplied in a dropper-tip, plastic squeeze bottle that can be stored at room temperature (59°F to 86°F or 15°C to 30°C). The medication should be protected from light. The manufacturer suggests one drop of solution four times daily beginning 24 hours after cataract surgery and continuing throughout the first 2 weeks of the postoperative period. One drop can be given 1 hour before refractive surgery and 15 minutes after the procedure is completed. Thereafter, one drop is administered four times daily for as long as 3 days.
Ketorolac tromethamine 0.5% ophthalmic solution is available in three different formulations: Acular 0.5% Ophthalmic Solution, Acular LS Ophthalmic Solution, and Acular PF Ophthalmic Solution (Allergan). Acular 0.5% Ophthalmic Solution is available in 3 mL, 5 mL, and 10 mL volumes each within an opaque plastic bottle 5 mL, 10 mL, and 10 mL, respectively, each with a controlled dropper tip. In addition to ketorolac tromethamine 0.5%, these solutions contain benzalkonium chloride 0.01%, edetate disodium 0.1%, octoxynol 40, sodium chloride, and purified water with an adjusted pH of 7.4. This preparation is approved by the FDA for use following cataract surgery for the treatment of postoperative inflammation with treatment initiated 24 hours after surgery and given one drop four times daily for 2 weeks. It is also approved for the relief of ocular itching caused by seasonal allergic conjunctivitis and is recommended by the manufacturer as one drop four times daily.
Acular PF Ophthalmic Solution is available as a sterile solution supplied in single-use vials within a package containing twelve single use vials each containing 0.4 mL of solution. This preservative-free solution contains only ketorolac tromethamine 0.5%, sodium chloride, hydrochloric acid and sodium hydroxide to adjust pH to 7.4, and purified water. This preparation is indicated for the reduction of ocular pain and photophobia after incisional refractive surgery.
Acular LS Ophthalmic Solution is indicated for the reduction of ocular pain and burning/stinging after cataract surgery. It is supplied as a 5 mL volume within a 10-mL bottle. This ophthalmic preparation contains ketorolac tromethamine 0.4%, benzalkonium chloride 0.006%, sodium chloride, edetate disodium 0.015%, octoxynol 40, purified water and is adjusted to a pH of approximately 7.4. It is best stored at 15°C to 25°C or 59°F to 75°F and protected from light.
These ophthalmic NSAIDs are available throughout the world where they are approved for different ophthalmic indications including treatment of allergic conjunctivitis, inhibition of intraoperative miosis during cataract surgery, temporary relief of pain and photophobia after refractive surgery, prevention of postoperative inflammation after cataract surgery, and the prevention and treatment of cystoid macular edema after cataract surgery. In addition, Indomethacin 1% Ophthalmic Suspension is available outside of the United States in a 5-mL dropper bottle.
Pharmacists are trained to prepare NSAID ophthalmic eyedrops by dissolving crushed tablets or the contents of capsules in artificial tears or other vehicles in an aseptic or sterile procedure. However, if improperly prepared, the result can be a potentially dangerous ophthalmic product. For example, 12 hospitalizations in western Pennsylvania, eastern Ohio, and West Virginia for ocular infections were reported in newspapers throughout the United States during the 1990s. Two of these cases required enucleations (Associated Press, San Francisco Chronicle, February 1991). Therefore, a properly qualified pharmacist with a special interest in ophthalmic pharmacology and the compounding of ophthalmic preparations is a requirement for the extemporaneous preparation of NSAID ophthalmic dose forms.
PHARMACOKINETICS
SYSTEMIC ADMINISTRATION
The NSAIDs that are of greatest ophthalmic interest have anti-inflammatory, analgesic, and antipyretic pharmacologic properties that are similar to those of the salicylates.10,11,12,13,14,15,16 One can emphasize these common pharmacologic activities and refer to NSAIDs as aspirinlike drugs.1 These agents are well absorbed from the gastrointestinal tract after oral administration, thereafter reaching maximum serum levels in 1 to 3 hours in fasting patients.17,18,19,20,21 Subsequently, they are metabolized in the liver and excreted in the bile and urine. Plasma half-lives are variable, possibly related to enterohepatic cycling, which is known to occur with the NSAIDs. Age, gender, and endogenous and environmental factors can affect clearance and, ultimately, the half-life of elimination of these drugs. All these agents are highly bound to protein (90% to 99%) and tissues.22
The rate of absorption of NSAIDs may be decreased by administration with meals or by formulation as slow-release (SR) preparations. Although the efficacy and tolerance of most slow-release preparations are not significantly better than those of conventional-release formulations, there is some evidence that an indomethacin preparation with slow-release characteristics can minimize dizziness and diarrhea.23
Although the NSAIDs are cleared by hepatic metabolism, the activity of some of these agents (aspirin, phenylbutazone, fenbufen, benorylate, and sulindac) is dependent, in part, on the formation of active metabolites.24 Furthermore, there can be differences in the pharmacokinetic profiles of enantiomers of the same drug. However, although the potential importance of stereoselective disposition and metabolic activation of NSAIDs cannot be disputed, there is no evidence that these pharmacokinetic parameters are important clinically during treatment with the NSAIDs currently approved for ophthalmic use.
Orally administered NSAIDs are widely used in the treatment of rheumatic diseases. The marked intersubject variability in pharmacologic response and incidence of side effects remains unexplained. Differences in plasma pharmacokinetics have not been clearly associated with this variability, although studies of the relationship between efficacy and unbound concentrations of NSAIDs are clearly needed. During treatment, increasing the dosage of a given NSAID in a nonresponder seems to do little to enhance efficacy, and selection of a different NSAID is frequently attempted.7 The value of this approach (i.e., changing drugs rather than increasing dose) during ophthalmologic therapy remains to be proved.
Although the NSAIDs are weak acids, and therefore, their renal clearance is increased by alkalinization of the urine, the excretion of unmetabolized drug is not usually a major pathway of elimination. However, renal impairment is of concern because of potential retention of NSAID metabolites and because of an increased risk of renal toxicity. Insofar as renal function deteriorates with age, the elderly are at greater risk of adverse effects.25
TOPICAL ADMINISTRATION
NSAIDs have excellent biphasic solubility and therefore penetrate the eye better after topical application than after systemic administration. For example, the rabbit aqueous humor level of indomethacin was much greater after the administration of either a 1% indomethacin suspension or 1% indomethacin sesame seed oil solution than after the oral administration of indomethacin.26,27 These laboratory observations have been confirmed in human studies.28 Volunteers given oral indomethacin 25 mg four times daily beginning 24 hours before surgery and a 25-mg dose 2 hours preoperatively did not have detectable aqueous humor levels despite mean peak blood levels of 642 ng/mL. However, application of a topical 1% aqueous suspension or a 1% sesame oil solution, five drops applied over 24 hours the day before surgery and one drop 45 minutes before surgery, provided adequate mean peak aqueous levels of solution (429 ng/mL) and suspension (198 ng/mL). Furthermore, these aqueous levels were not associated with measurable blood levels.
The ocular instillation of NSAIDs provides ocular tissue levels, including aqueous humor, adequate to inhibit prostaglandin (PG) synthesis. Ocular absorption and distribution of topically administered flurbiprofen in normal and aphakic rabbit eyes has been studied.8,28 Ocular instillation of 50 μL of 0.03% flurbiprofen provides ocular tissue levels (cornea, conjunctiva, sclera, iris, choroid, retina, ciliary body, and aqueous humor) sufficient to provide 50% inhibition of PG synthetase in phakic eyes (more than 90 ng/mL). Higher concentrations of drug were found in the vitreous humor, choroid, and retina of aphakic eyes. Topical application of 0.5% ketorolac tromethamine solution to normal rabbit eyes provides drug to all the ocular tissues, including cornea, conjunctiva, sclera, iris, ciliary body, lens, choroid, retina, vitreous humor, and aqueous humor.29 Topical application of suprofen 0.5% results in significant ocular levels that are associated with the inhibition of the generation of PGE2, PGF2a, PGI2, and thromboxane B2 from inflamed rabbit corneas. This inhibition is more effective than that achieved with topical prednisolone 1%.15 A comparison of the ocular penetration and subsequent effects of diclofenac, flurbiprofen, and indomethacin on disruption of the blood–aqueous barrier (BAB) in rabbit eyes has been reported.30 The breakdown of the BAB after paracentesis of the anterior chamber is inhibited in a dose-dependent manner. The anti-inflammatory effects persisted 6 hours. Dose-response curves for the NSAIDs are comparable and are in the range of 3 × 106 mol. These dose ranges are comparable to those that have been used for inhibition of PG synthesis in vitro in rabbit conjunctival tissue.
The therapeutic usefulness of the NSAIDs appears to derive, in part, from their ability to inhibit the synthesis of PGs and the associated antimiotic and anti-inflammatory activities.22 An increase in PGE and PGF in the aqueous humor after cataract extraction has been demonstrated.31 Topical indomethacin solution and suspension easily achieved the 60 ng/mL concentration of indomethacin that is the median infective dose (ID50) for in vitro inhibition of PG synthesis within the aqueous humor.32 Therefore, these clinical observations, coupled with the increased potential for undesirable systemic side effects associated with oral administration, suggest that topical administration of NSAIDs is preferred. However, it is too early to conclude that the topical administration of NSAIDs is not associated with significant systemic absorption or systemic toxicity. It appears that a significant percentage of topically applied NSAID can appear in the systemic circulation after absorption from the nasolacrimal outflow system and the vascular nasal mucosa. After topical application to the rabbit eye of 50 μL 0.5% ketorolac (250 μg), peak plasma concentrations of 0.2 μg/ml were measured within about 15 minutes.29,33 Furthermore, after topical administration of flurbiprofen solutions, 74% of the dose appeared to enter the systemic circulation.20 These data appear to conflict with the study previously described.28 However, the results of laboratory determinations can be influenced by the sensitivity and timing of the assay, species differences, and variations in absorption from the nasolacrimal system. Therefore, although systemic absorption of an NSAID is relatively small and variable after topical treatment, it is less than prudent to assume that the topical route lacks systemic toxicity. Eyelid closure and digital occlusion of the nasolacrimal outflow system enhance intraocular penetration of drug and minimize systemic absorption of the instilled medication.34,35 These techniques should help provide an optimum risk:benefit ratio for the patient.
PHARMACODYNAMICS AND RATIONALE FOR USE
PHARMACODYNAMICS
PG research began with Ambache’s study of “irin” more than 60 years ago, but the chemical identification of this endogenous mediator occurred subsequently. Many of the major advances in understanding these autacoids have occurred in the past two decades.36 PGs produce many physiologic effects within the eye, including miosis, conjunctival hyperemia, increased permeability of the blood–ocular barriers, and changes in intraocular pressure.37,38,39,40 Furthermore, PGs have become recognized as potential chemical mediators of both cellular and humoral aspects of inflammation and allergy.41,42,43
Aspirin and other NSAIDs decrease the synthesis of PGs by inhibiting cyclooxygenase (COX), the enzyme that catalyzes the formation of endoperoxides from arachidonic acid. In addition, indomethacin has shown inhibitory activity against phospholipase A2 and C. There is little evidence that NSAIDs inhibit lipoxygenase, except at concentrations higher than those achieved therapeutically; therefore, NSAIDs have limited ability to inhibit the generation of leukotrienes, as shown in Figure 2.44,45,46,47,48 However, diclofenac may indirectly limit leukotriene production by sequestration of arachidonic acid into triglyceride pools.49 This would enhance its anti-inflammatory activity because leukotrienes possess chemotactic activity.
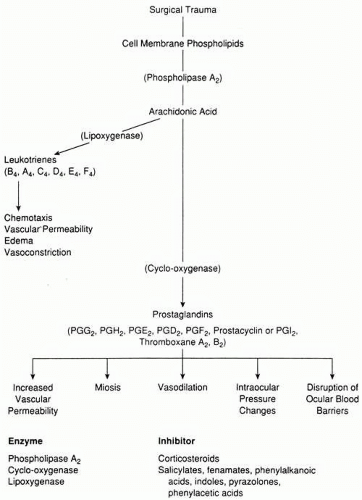 Fig. 2. Mediators of inflammation-potential inhibition. |
Although it is tempting to summarize the pharmacodynamics of NSAIDs by thinking of them simply as COX inhibitors, it is unlikely that this single mechanism accounts for all their pharmacologic effects. Different hypotheses have been suggested. These agents, at higher concentrations, blunt the functions of inflammatory cells such as polymorphonuclear leukocytes. Investigators have described how NSAIDs inhibit the aggregation of polymorphonuclear leukocytes. These drugs inhibit calcium movements and enhance the poststimulation increase in intracellular cyclic adenosine monophosphate (cAMP); these actions could alter the early steps of neutrophil activation. NSAIDs have a free radical scavenger action. As stated previously, they inhibit peripheral blood monocyte phospholipase C activity. In addition, NSAIDs may indirectly reduce vascular permeability.7,22,47,50,51,52,53,54
NSAIDs are anionic, planar molecules that can partition into lipids, such as those found in cell membranes and particularly in the acid environments provided by inflammation. Many membrane effects are likely related to the ability of aspirin like drugs to insert into the plasma membrane’s lipid bilayer where they can disrupt protein–protein interactions and normal signaling events. These drugs inhibit membrane-associated nicotinamide adenine dinucleotide phosphate (NADPH) oxidase activity, uptake of precursor arachidonate, transmembrane anion transport, and mitochondrial oxidative phosphorylation.47,55,56,57 Finally, at high doses; NSAIDs inhibit nonprostaglandin activities, such as proteoglycan synthesis by chondrocytes and chemoattractant binding.58,59,60,61
Despite these qualifications, the inhibition of COX activity does appear to correlate with the therapeutic usefulness of NSAIDs in ophthalmology (i.e., the inhibition of intraoperative miosis, the modification of postoperative inflammation, the prevention and treatment of CME after cataract surgery, the relief of excessive pain and photophobia after refractive surgery and the treatment of allergic conjunctivitis).
Most NSAIDs inhibit not only PGs at sites of inflammation but also PGs that serve to assist with important functions throughout the body. Such inhibition may be harmful as described within the toxicity section of this chapter. The tendency for NSAIDs to impair normal gastrointestinal mucosal function with associated mucosal damage can result in serious gastrointestinal complications. A prospective trial of more than 8,000 patients with rheumatoid arthritis who were taking NSAIDs found the rate of serious gastrointestinal complications to be 1.54% per year.62 NSAIDs are among the most widely used therapeutic agents with approximately $2 billion spent in the United States on prescription NSAIDs alone.63 This means thousands of patients are at risk each year.
CycloOxygenase Isoforms
A potentially useful approach to avoiding some of the complications of NSAID treatment became possible with the identification of two isoforms of COX: COX-1 and COX-2. COX-1, a constitutive enzyme, synthesizes PGs that regulate physiologic processes. It is present in most tissues and, therefore, normally expressed in the gastrointestinal tract, kidneys, platelets, and vascular endothelium when it plays a role in their normal physiologic function. COX-2 is an inducible enzyme that is expressed throughout the body primarily during inflammatory responses, and in association with pain or in relation to fever. However, COX-2 may be constitutive, to some degree, in the absence of inflammation, within body sites such as the brain and kidneys.64 The development of NSAIDs that preferentially inhibit COX-2 provides the potential for relieving pain and inflammation without the adverse effects of COX-1 blockade.65 The advantages of this approach have been questioned in that some believe the enzymatic inhibitory activities demonstrated in vitro may not reflect COX inhibition in human tissues and, therefore, there is some question whether the COX-1 sparing effect translates into prevention of untoward effects during treatment.66 Furthermore, the clinical studies most often quoted that conclude that patients have a 50% (VIGOR Study) to 70% (CLASS Study) decreased gastrointestinal toxicity while using COX-2 inhibitors report a reduction of complicated confirmed upper gastrointestinal events from 1.4% to 0.6% (VIGOR Study) and 1.2% to 0.44% (CLASS Study). Therefore, while the percentages discussed are impressive they reflect relatively small numbers of patients.67,68 Finally, the cardiovascular safety of COX-2 inhibitors has recently been questioned. After the demonstration of an increase by twofold of heart attacks and strokes in patients using rofecoxib (Vioxx, Merck & Co., Whitehouse Station, NJ) for longer than 18 months, this COX-2 inhibitor was removed from the market.69 It is not clear whether other COX-2 inhibitors (celecoxib, Celebrex, Pharmacia, New York, NY; valdecoxib, Bextra, Pharmacia) share this cardiovascular toxicity.70,71,72,73,74
In conclusion, COX-2 inhibitors do not inhibit platelet function, they appear to reduce but not eliminate the risk of gastrointestinal bleeds and perforations and their nephrotoxicity is equivalent to conventional NSAIDs. Finally, it remains to be proven whether inhibition of COX-3 in the brain and the spinal cord may be the mechanism of action of acetaminophen.75
RATIONALE FOR THERAPEUTIC USE
Intraoperative Inhibition of Miosis
Frequently, ophthalmologists are confronted with a miotic pupil during cataract surgery. This can significantly complicate the removal of the cataract and the insertion of an appropriate intraocular lens (IOL). PGs are recognized as one of the mediators of the ocular inflammatory response, including atropine-resistant pupillary miosis, that occurs after ocular trauma.76 After many different types of ocular trauma, including ophthalmic surgery, these mediators are released within the eye and induce miosis.77,78 Pretreatment of experimental animals and humans with indomethacin, and other NSAIDs, reduces the miotic effect of surgical trauma.79,80,81 Flurbiprofen and suprofen were approved for use by the FDA for inhibition of intraoperative miosis during cataract surgery. However, suprofen is no longer commercially available. The studies providing support for this therapeutic benefit from topically applied NSAIDs are discussed in a subsequent section.
Treatment of Postoperative Inflammation After Cataract Surgery
Postoperative inflammation can induce tissue injury after contemporary cataract surgery in spite of the advances in technique and instrumentation.82,83,84 An evaluation of the treatment of inflammation is complicated by the multiplicity of ocular tissues: conjunctiva, sclera, cornea, aqueous humor, iris, ciliary body, choroid, retina, vitreous humor, and optic nerve. Each tissue represents a different environment for the expression of the inflammatory response.85,86
In clinical practice, the ophthalmologist examines postoperative patients with the slit lamp biomicroscopy to look for evidence of excessive inflammation in the early postoperative period.87,88,89 The accumulation of cells and protein (recognized as flare) within the aqueous humor is accepted as the clinical sign of a surgically induced anterior uveitis.88 Some physicians have advocated the use of anterior segment fluorophotometry to permit greater objectivity, better reproducibility, and quantification of these observations of inflammation.90,91,92,93,94,95,96 This technique assumes that the breakdown of the BAB, as measured by fluorescein accumulation in the anterior chamber, correlates with the accumulation of cells and protein within the anterior chamber of the eye. The fluorophotometric technique has been used to follow acute anterior uveitis90 and extracapsular cataract surgery postoperative inflammation.96 The laser cell flare meter also provides accurate and sensitive instrumentation to quantify inflammatory cells and flare following an inflammatory insult. However, it is not yet in widespread use even in clinical research performed within the United Stares despite the frequent criticism of its absence in clinical studies.97
The pathophysiologic significance of many of the potent endogenous agents (bradykinin, histamine, serotonin, chemotactic factors, and arachidonic acid metabolites such as PGs, prostacyclin, thromboxane A2, and leukotrienes) liberated during and following ocular surgery is unclear. However, evidence has accumulated that PGs are one of the mediators of the ocular inflammatory response.39,98 Therefore, the ability of NSAIDs to inhibit the synthesis of PGs appears to be a major part of the mechanism by which they reduce the clinical signs and symptoms of postoperative inflammation. The FDA approves diclofenac 0.1% and ketorolac tromethamine 0.5% ophthalmic solutions for use in treating postoperative inflammation following cataract surgery in the United States. In addition, indomethacin 1% ophthalmic suspension is available in other parts of the world for the treatment of postoperative inflammation.
Topically applied glucocorticoids are commonly used by ophthalmologists to reduce postoperative inflammation.99 They are approved for use after cataract surgery and implantation of an IOL to prevent excessive inflammation: 1% rimexolone (Vexol 1%, Alcon) and 0.5% loteprednol (Lotemax 0.5%, Bausch & Lomb)100,101,102 The pharmacodynamics of the glucocorticoids and the NSAIDs overlap in that glucocorticoids inhibit phospholipase A2 and are, therefore, also inhibitors of PG synthesis.32 However, glucocorticoids have many other effects on inflammation, including those on white cells (inhibit migration of macrophages and neutrophils; induce lymphocytopenia, eosinopenia, and monocytopenia; and induce neutrophilic leukocytosis), blood vessels (reduce capillary permeability and suppress vasodilatation), and inflammatory chemical mediators (inhibit degranulation of neutrophils, mast cells, and basophils; stabilize lysosomes and suppress action of lymphokines).103,104 In addition, by inhibiting phospholipase A2, steroids not only decrease the synthesis of PGs but also inhibit the lipoxygenase pathway and decrease leukotriene formation (see Fig. 2). These differences in pharmacodynamic activity between steroids and NSAIDs may result in different therapeutic efficacies and toxicities. Furthermore, they may provide for synergism (additivity or potentiation) when NSAIDs are used with steroids. Historically, the concomitant use of corticosteroids during studies of postoperative inflammation has confused the critical evaluation of NSAID effects and has contributed to a delay in the FDA approval process in the United States. Glucocorticoids have only recently been approved for use as a postoperative anti-inflammatory agent and, therefore, prior to this approval the FDA considered them a placebo during studies of postoperative inflammation. This is discussed in a subsequent section of this chapter.
Prevention and Treatment of Cystoid Macular Edema After Cataract Surgery
CME is one of the most common causes of reduced vision following cataract surgery.105 Inasmuch as the pathophysiology of this problem is not completely understood,106,107,108,109,110 any attempt to understand the therapeutic effect from a given medical treatment will be incomplete. However, inflammation appears to be a major component of the pathogenesis of CME.111,112,113,114,115,116,117,118 In support of this rationale are several observations and associations, including the signs and symptoms,112 the increased capillary dilatation and permeability observed with the fluorescein angiogram,119 and the retinal pericapillary cellular infiltration within pathology specimens taken from patients with CME at the time of their death.114 Increased leakage from the anterior uvea has been observed during iris angiography performed in the presence of CME.111,120,121,122,123 Finally, there is greater anterior ocular inflammation in the immediate postoperative period, as measured with slit lamp examination and anterior ocular fluorophotometry, in eyes that eventually develop angiographic CME 6 weeks after surgery, compared to eyes that do not.96
PGs appear to be part of the pathogenesis of CME. PGs produce inflammation,124,125,126 are present in ocular tissues,127 are released during ocular surgery,128 and can disrupt the BAB.39,111,120,121,123,129,130 An active transport system for PGs has been demonstrated in the ciliary body area,131 and a transvitreal path from the anterior segment to the retina has been identified.132 PGs’ ocular pharmacologic effects are consistent with several of the anatomic changes recognized as part of CME, such as perifoveal capillary dilatation, increased capillary leakage, and breakdown of the BAB.39,133 Therefore, it is not surprising that the rationale for prevention and treatment of CME has focused on NSAIDs, with the goal of reducing the production of PGs.110 NSAIDs are approved for use in the treatment and prophylaxis of CME throughout the world but not in the United States. This is discussed in a later section of this chapter.
Treatment of Seasonal Allergic Conjunctivitis
Approximately 20% of the general population experience symptoms of allergy.134 The most common type of allergic conjunctivitis is seasonal rhinoconjunctivitis accounting for more than 50% of all cases of allergic conjunctivitis. The hallmark symptom is itching. Evidence exists that ketorolac has mast cell stabilizing ability.135 PGE1 lowers the threshold of human skin to histamine-evoked itching.136 PGD2 is the primary PG produced by the mast cell in type I hypersensitivity reactions.43 There is some evidence, including its identification in tears of patients with vernal conjunctivitis, that PGF may also be involved in allergic disease.137 Interestingly, some PGs may have anti-inflammatory activities possibly participating in negative feedback systems that result in the allergic response being self-limited.138
Ketorolac tromethamine 0.5% solution has been approved for use in relieving ocular pruritus associated with allergic seasonal conjunctivitis. Ketorolac solution given four times daily for 1 week was more effective than placebo in relieving itching and clinical signs and symptoms of allergic conjunctivitis, including erythema, edema, and mucous discharge.139,140
Relief of Pain and Photophobia Associated With Refractive Surgery
Patients experience pain after refractive surgical procedures. The role of PGs in the production of pain is unclear.141 The corneal epithelium and stroma have PG-synthesizing capability that is enhanced after injury and different endogenous mediators, including PGs, stimulate peripheral nerves and cause discomfort.142 Small concentrations of PGE2 and PGI2 produce sensitivity to touch. Investigators have reported that while PGs increase the sensitivity of pain receptors, they do not induce the pain itself.143 Autacoids, including PGs, increase the amounts of cyclic adenosine monophosphate and ionic calcium at the nociceptor membrane and decrease the activation threshold.144 A randomized, double-masked, placebo-controlled study of the effect of topical administration of indomethacin 1% suspension in patients with corneal scars, erosions, infiltrates, and edema reported significant improvements in symptoms such as photophobia, itching, burning, foreign-body sensation, tearing, and pain.145
At present, the FDA approves diclofenac 0.1% and ketorolac tromethamine 0.5% ophthalmic solutions for use after refractive surgery. Clinical studies supporting the use of these topically effective NSAIDs for this indication are summarized in a subsequent section of this chapter.
THERAPEUTIC POTENTIAL: REVIEW OF CLINICAL STUDIES
INHIBITION OF INTRAOPERATIVE MIOSIS
Adequate pupil dilatation is desirable during cataract extraction and IOL implantation. Decreasing pupil size is the only statistically significant risk factor for vitreous loss and zonular breaks in 1,000 extracapsular cataract extractions, as described in a prospective study of intraoperative complications.146 The incidence of vitreous loss with larger pupils (greater than 6 mm) averaged 2.8%, compared to 5.9% for smaller pupils (less than 6 mm). Flurbiprofen 0.03% (Ocufen Ophthalmic Solution) and suprofen 1% (Profenal Ophthalmic Solution) are approved by the FDA for use as intraoperative inhibitors of miosis.147,148 The published clinical studies that provide support for the claim that NSAIDs inhibit intraoperative miosis are summarized in Table 2. These studies show that NSAIDs have a statistically significant effect in maintaining mydriasis, compared with placebo, when administered preoperatively with concurrent topical sympathomimetics and parasympatholytics.
TABLE 2. Nonsterioidal Anti-Inflammatory Drugs and Inhibition of Intraoperative Miosis | |||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||
The published data suggest that the pharmacologic effect of NSAIDs on pupil size is small.149,150 Furthermore, this small effect appears to be quite variable from one surgical practice to another. One well-designed clinical study that provides support for the efficacy of flurbiprofen is a double-masked, placebo-controlled, randomized study of 34 white patients who received one drop of flurbiprofen 0.03% solution or vehicle in the eye to be operated at 6:00 AM and 7:00 AM, the morning of surgery, and 60, 45, and 30 minutes preoperatively.149 In addition, each patient received tropicamide 1% and phenylephrine 2.5% at 60, 45, and 30 minutes preoperatively. Preoperative pupil measurements were taken before conjunctival incision and compared to postoperative measurements taken after irrigation and aspiration of cortical material. The flurbiprofen-treated group showed a mean decrease in pupil size of 2.5 mm, and the control group showed a mean decrease of 3.9 mm (p = 0.003). Two controlled studies showing efficacy are required for new drug approval by the FDA. The second study remains unpublished, but it is of similar design, and its results are provided in the Summary Basis of Approval for Ocufen.147 A total of 48 patients were enrolled. The mean percentage decreases from baseline pupil diameter were significantly less in the flurbiprofen-treated group for one surgeon (p = 0.03) but not for the other surgeon (p = 0.26). In addition, the control eyes’ decreases from baseline pupil diameter were different for the different surgeons, which was explained as a variability in the amount of iris trauma during surgery. Therefore, it appears that the potential benefit of flurbiprofen 0.03% can vary with surgical technique.
Only one published report exists that supports suprofen’s ability to inhibit intraoperative miosis.150 This multicenter study included 412 patients enrolled by eight different surgeons. Patients received either suprofen 1% ophthalmic solution or vehicle in a double-masked fashion every 4 hours the day before surgery and every hour prior to surgery for three additional doses. Surgeons used their usual regimen of mydriatics, both preoperatively and intraoperatively. Pupillary diameters were measured both before the initial surgical incision and before IOL implantation or instillation of miotic. Most, but not all, of the investigators demonstrated a statistically significant (p = 0.034) decrease in pupil size in their vehicle-treated patients. The difference in reduction of the mean pupil diameter was small (suprofen = 1.01 mm, vehicle = 1.48 mm), as reported in Table 2. These observations are described and analyzed in greater detail in a review article.151
The FDA has not approved for intraoperative inhibition of miosis ketorolac 0.5% or diclofenac 0.1% ophthalmic solutions for use during cataract surgery. However, controlled studies have demonstrated these topically applied NSAIDs to have this effect. For example, ketorolac 0.5% ophthalmic solution was compared to flurbiprofen 0.03% ophthalmic solution in a well-controlled, masked, prospective study of 118 patients. Horizontal pupillary diameter measurements were obtained at the start of surgery, just before phacoemulsification, before lens implantation, and after lens implantation. While mean horizontal pupillary diameters were similar at the start of surgery in both treatment groups, a consistent trend of larger pupillary diameters was seen in all subsequent surgical intervals in the ketorolac-treated group. The more significant inhibition of miosis at all intervals, and the more stable mydriasis throughout the surgery within the ketorolac-treated group encouraged the authors to conclude ketorolac is an effective inhibitor of miosis during phacoemulsification and implantation of an IOL.152
Although indomethacin ophthalmic suspension is not approved for any indication in the United States, it was the first NSAID studied in eyedrop form. One study of this topical preparation reports a statistically significant inhibition of intraoperative miosis.153 Although stated to be a double-masked study, it is unclear how the investigators made the suspension indistinguishable from the placebo solution used during this comparison. A second investigation, reported from The Netherlands, compares indomethacin 0.5% aqueous solution (prepared extemporaneously with polyvinyl-pyrolidone, sodium phosphate, benzalkonium chloride, and ethylenediaminetetraacetic acid [EDTA]) and placebo vehicle solution in a double-masked study. Pupil diameters were measured at four different times: the beginning of surgery, after the capsulotomy, after expression of the lens nucleus, and at the end of cortical aspiration. Differences existed at each time period, but the greatest difference between mean pupillary diameters was after the expression of the lens nucleus, at which time the results favored NSAID treatment in a statistically significant fashion. The authors believed a decrease in miosis made the removal of nucleus and cortical material easier.154
Although different topically applied NSAIDs have been compared, a significant difference between their effects on maintaining pupil dilatation during cataract surgery if present appears to be subtle. Most studies agree that flurbiprofen is as effective as indomethacin in maintaining mydriasis during cataract surgery.8,9,155,156 Ketorolac is reported as providing a more stable mydriatics effect during phacoemulsification compared to flurbiprofen.152 Less pupil constriction was seen among patients pretreated with flurbiprofen or indomethacin than among those treated with diclofenac ophthalmic solution or placebo.157 A more sustained mydriatic effect was observed after administration of flurbiprofen then after indomethacin.158 Although these reports suggest that there may be subtle differences between the topically applied NSAIDs and their ability to maintain mydriasis during cataract surgery that appear to favor ketorolac, we await a prospective, double-masked, randomized study comparing all them during contemporary cataract surgery before we can conclude there is a clinically significant difference.
In summary, the studies supporting NSAID efficacy for the inhibition of intraoperative miosis consistently describe a statistically significant effect. Because pupil area increases with the square of the radius, an apparently small difference in pupil diameter can reflect a pupil area difference that is more impressive. It is interesting that the changes in pupil diameters in vehicle-treated eyes in different studies often appear smaller than those in NSAID-treated eyes. Although it is tempting to explain this by assuming differences in surgical technique, such reasoning does not explain why, occasionally, a given surgeon had less miosis in the vehicle group.151 Therefore; endogenous factors other than PGs may be playing important roles in the development of intraoperative miosis. This possibility has been elaborated upon in an editorial159 concerning the value of routine use of preoperative NSAIDs during cataract surgery.
Furthermore, some surgeons can maintain intraoperative mydriasis with only parasympatholytic and sympathomimetic agents. A study has examined NSAID efficacy for intraoperative inhibition of miosis and the significance of using, concurrently, epinephrine within the irrigation solutions.156 Epinephrine (0.3 mL of 1:1000) without preservative was mixed with 500 mL of buffered saline solution and used as an intraocular irrigating solution during the irrigation and aspiration of cortical material. Indomethacin 1% (Indocid Ophthalmic Suspension) was compared to flurbiprofen 0.03% (Ocufen Ophthalmic Solution) and placebo, each with and without epinephrine within the irrigation solution. The authors concluded: “The use of intraoperative epinephrine was by far the most effective factor in reducing progressive miosis, regardless of whether antiprostaglandins were used.”156 However, the therapeutic benefit of NSAID treatment, while less than that of epinephrine, was additive. Few would criticize surgeons for using NSAIDs preoperatively to enhance mydriasis. However, it seems clear that an adequate intraoperative dilatation can be maintained simply by using good surgical technique, some combination of preoperative parasympatholytic and sympathomimetic eyedrops, and intraoperative epinephrine in the intraocular irrigation solution.
POSTOPERATIVE ANTI-INFLAMMATION
Initially, the ability of indomethacin suspensions and solutions to suppress postoperative inflammation appeared to be quite variable.160 However, Sawa and Masuda161 suggested that NSAIDs prevent synthesis of PGs but probably do little to antagonize their effects once present. Therefore, one potential explanation for the inconsistent anti-inflammatory response observed after indomethacin treatment was that once inflammation was established, treatment with the NSAID was of less benefit. Subsequently, studies were designed to evaluate the effectiveness of indomethacin and other topically applied NSAIDs given prior to and/or immediately after surgical procedures. These studies report more consistent anti-inflammatory activity from topically applied NSAIDs administered before surgery. It is interesting that both 0.1% diclofenac and 0.5% ketorolac ophthalmic solutions have been approved for use following cataract surgery beginning 24 hours after surgery and continuing for 2 weeks. However, there is evidence from a relatively small study that there may be benefit from initiating treatment with topical NSAIDs 3 days prior to surgery.162
Evaluation of the Inflammatory Response to Cataract Surgery
Slit lamp biomicroscopy is commonly used by clinicians to look for evidence of excessive inflammation in the early postoperative period. Subjective clinical scoring methods quantify the severity of the anterior ocular inflammatory response.87,88,89 These were used to study indomethacin’s effect on postoperative anterior chamber cells and flare and conjunctival vasodilation.9,94,163 However, these techniques suffer from observer bias and error and problems with reproducibility. Therefore, investigators recognized a need for greater objectivity and sensitivity and emphasized the potential usefulness of anterior ocular fluorophotometry.93,94,95,164,165
However, some have suggested that anterior ocular fluorophotometry may not provide an appropriate measure of anterior ocular inflammation. In support of this contention, conditions associated with a breakdown of the BAB in the apparent absence of acute anterior uveitis are cited: exposure to chemical irritants and drugs, trauma, light, paracentesis, and a relatively inert intraocular foreign body, such as an IOL. However, each of these exposures is recognized as a potential etiology for inflammation,166 and each of these insults has been used as a model to study ocular inflammation.128 The therapeutic goal of treatment after each of these exposures is to minimize the inflammatory response, including breakdown of the BAB, with the use of corticosteroids and parasympatholytics such as atropine. Atropine is a drug well recognized as capable of stabilizing the BAB,167,168,169,170 and it was at one time considered an anti-inflammatory drug. The occurrence of contralateral breakdown of the BAB after cataract surgery has been reported.171 This observation is considered by some as evidence that BAB breakdown need not correlate with anterior ocular inflammation. However, it may reflect our poor understanding of this consensual ocular phenomenon.172,173
Therefore, it appears reasonable to assume that aqueous humor fluorophotometric measurements of breakdown of the BAB usually correlate with levels of intraocular inflammation. The advantage of fluorophotometry is its ability to objectively produce quantitative data for consistent and reliable comparisons.90,174,175 It is reassuring that the results of direct measurements of aqueous protein and cells compare favorably with anterior segment fluorophotometry.176,177 In addition to fluorophotometry, laser cell-flare measurements have been used to make more objective and reliable measurements of cell and flare response in the postoperative period as is discussed in subsequent sections. However, despite these advances, investigators continue to use less accurate methods to follow inflammation.97
Concurrent Corticosteroid Administration: A Potential for Synergism
Many studies of NSAID anti-inflammatory activity include concurrent administration of corticosteroids. For example, most of the clinical studies of indomethacin used corticosteroids in the treatment of postoperative inflammation,9,94,163,164,165,178 as previously summarized.151 Corticosteroids have anti-inflammatory activity and overlap with NSAIDs in their ability to inhibit the generation of PGs after an inflammatory insult. Therefore, it is not possible, using the results of these studies, to conclude whether the observed effects on postoperative inflammation are related to NSAID treatment or to a synergistic effect achieved with corticosteroids and NSAIDs. Evidence for the existence of this synergism is provided in subsequent sections of this chapter. In addition, it is not possible to determine whether the concurrent steroid treatment is masking a tendency for topically applied NSAIDs to cause ocular irritation.9 Therefore, one must review clinical studies, without concurrent steroid treatment, to form an accurate opinion about the potential efficacy and toxicity of an NSAID when given alone for postoperative inflammation.
Placebo-Controlled Studies: Cataract Surgery
Anti-inflammatory effects from topically applied NSAIDs with and without concurrent corticosteroid treatment have been studied in double-masked, randomized, placebo-controlled studies of patients after cataract surgery with and without implantation of an IOL. Therefore, it is not surprising that the FDA approves two topically applied NSAIDs for this indication. The major clinical studies that provide evidence supporting this anti-inflammatory effect following the topical application of 0.5% ketorolac tromethamine (Acular, Allergan) and diclofenac 0.1% (Voltaren, Novartis Ophthalmics) ophthalmic solutions are summarized in Table 3. Although diclofenac 0.1% ophthalmic solution was the first drug approved by the FDA for use as an anti-inflammatory treatment after cataract surgery, the complete data supporting the efficacy of such treatment (i.e., a comparison of diclofenac 0.1% ophthalmic solution with placebo that supported the approval of this drug by the FDA) have yet to be published. The Summary Basis of Approval for Voltaren, available from the FDA, reveals that diclofenac treatment was significantly better than placebo in attenuating the postoperative “mean inflammation score” (cells and flare combined) and the conjunctival and ciliary inflammations, as observed during slit lamp examination on postoperative days 4, 8, and 15. Unfortunately, the details of many of these studies have not been published, which makes a critical evaluation difficult. However, one published study includes 148 subjects 99 treated with 0.1% diclofenac and 49 treated with an identical placebo vehicle solution) and included only subjects with significant postoperative inflammation (+4 score for combined cells and flare) 22 to 34 hours following surgery. The diclofenac treated subjects demonstrated significantly lower scores for their combined cells and flare 4, 8 and 15 days after surgery. Furthermore, there were 4 times fewer drop outs related to excessive inflammation within the diclofenac-treated group compared to the placebo-treated group.179 A summary of related abstracts and foreign studies has been published that provides an additional glimpse at the data supporting diclofenac’s approval by the FDA.180 Among those abstracts is a multicenter, double-masked, parallel, placebo-controlled study of more than 300 patients that was presented during the 1990 meeting of the Association for Research in Vision and Ophthalmology.181 This report describes an experimental approach similar to that used by Kraff et al,179 and it supports their observations and conclusions. Finally, there are suggestions that diclofenac has been used orally to reduce inflammation following cataract surgery.182,183 This is an unapproved use of the systemic preparation.
TABLE 3. The Effects of Nonsteroidal Anti-Inflammatory Drugs on Postoperative Inflammation: Randomized, Double-Masked, Placebo-Controlled Studies | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Four major studies published in the peer-reviewed literature reflect the data that the FDA reviewed prior to approving 0.5% ketorolac tromethamine for use as a postoperative anti-inflammatory drug. All four studies describe the effects of 0.5% ketorolac tromethamine ophthalmic solution compared to placebo treatment and they consistently demonstrate an impressive anti-inflammatory activity without concurrent administration of postoperative corticosteroids. These four studies can be divided into two major groups of clinical investigations. One group consists of two investigations that study the use of preoperatove and postoperative 0.5% ketorolac on subjects undergoing cataract surgery, includes all subjects demonstrating all degrees of postoperative inflammation and include both slit lamp biomicroscopy observations and fluorophometry evaluations.91,184 The two subsequent clinical studies required that treatment be initiated 24 hours after surgery, that only slit lamp biomicroscopy observations be recorded and enrolled only subjects with a significant inflammatory reaction at the first postoperative visit.185,186 All four of these studies are summarized in Table 3.
These published studies permit a careful evaluation of ketorolac’s ability to provide a significant postoperative anti-inflammatory effect. For example, preoperative and postoperative 0.5% ketorolac tromethamine solution, one drop three times daily for 19 days, reduced anterior ocular inflammation during the first month after extracapsular cataract extraction (ECCE), compared to placebo without the application of any corticosteroids.91 All patients were examined with the slit lamp biomicroscopy on postoperative days 1, 2, 12, 19, and 28. Lid edema, conjunctival vasodilatation, ciliary flush, and anterior chamber cells were graded 0 to 3+ at each of these examinations. Fluorophotometry was used to quantify the anterior chamber reactions. Topical treatment was significantly more effective than placebo treatment in reducing lid edema, conjunctival vasodilatation, and ciliary flush on postoperative days 2, 12, and 19 (p = 0.001), and it was significantly more effective in decreasing anterior chamber cells on day 12 (p = 0.043), as determined by slit lamp biomicroscopy. Anterior ocular fluorophotometry measurements favored NSAID treatment at all postoperative examination days (p = 0.001).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


