(32%), Staphylococcus aureus (10%), and Moraxella catarrhalis (9%) (7). Since the introduction of the 7-valent pneumococcal vaccine for children, there has been a trend toward decreasing prevalence of S. pneumoniae isolates and increasing prevalence of H. influenzae isolates derived from adults with acute maxillary sinusitis (8).
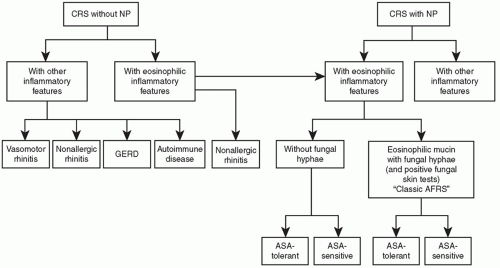 Figure 35.1 Classification for CRS. |
Without requiring antigen specificity, T-cell-mediated inflammation may be propagated and magnified by the presence of bacterial exotoxins. Superantigens are not only linked to a dramatic upregulation in T-cell response, but have also been associated with increased eosinophils, increase in IL-5 and upregulation of PGE2 (11).
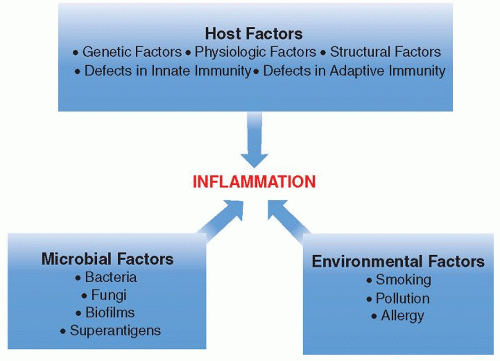 Figure 35.2 Underlying factors contributing to the pathophysiology of CRS. |
case-control studies have now documented a significant independent association between secondhand smoke and CRS (30,31).
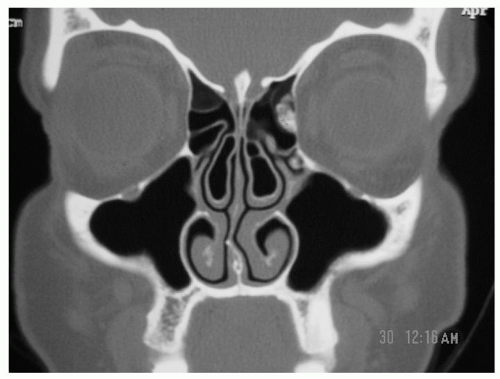 Figure 35.3 Coronal CT scan showing bilateral concha bullosa. |
Otolaryngology-Head and Neck Surgery (AAO-HNS). Their work resulted in the publishing of “working definitions” for rhinosinusitis in 1997 (48). The Task Force proposed a symptom-based format for the diagnosis of rhinosinusitis, with major and minor symptom categories (Table 35.1). According to the duration of the symptoms, rhinosinusitis was defined as acute when symptoms lasted 4 weeks or less, subacute when symptoms were present for 4 to 12 weeks, or chronic for symptoms lasting longer than 12 weeks. The term recurrent acute rhinosinusitis was reserved for patients with four or more episodes per year with disease-free intervals in between. An acute exacerbation of CRS was defined as a sudden worsening of symptoms in a patient already diagnosed with CRS, with return to baseline symptoms after treatment. A strong history consistent with rhinosinusitis would require the presence of either two major factors, or one major and two minor factors. When only one major factor or two or more minor factors were present, this constituted a suggestive history in which rhinosinusitis should be included in the differential diagnosis.
TABLE 35.1 SIGNS AND SYMPTOMS ASSOCIATED WITH DIAGNOSIS OF RHINOSINUSITIS (1996 RHINOSINUSITIS TASK FORCE) | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||
TABLE 35.2 DIAGNOSTIC CRITERIA FOR SINUSITIS FROM 2007 TASKFORCE | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|



