Nonneoplastic Lesions of the Larynx
The larynx is most often biopsied because of suspicion of malignancy. Many biopsies will be diagnosed as conventional squamous cell carcinomas; however, many nonneoplastic pathologies can also involve the larynx (Table 15.1). This chapter reviews the various infectious and inflammatory processes that can involve the larynx, as well as nonneoplastic polyps and cysts.
CONTACT ULCER
Contact ulcer or laryngeal granuloma is a relatively common lesion that typically involves the posterior portion of one or both sides of the larynx. The descriptor “contact” emphasizes the traumatic etiology for most of the lesions, which includes, but is not limited to, endotracheal intubation, acid reflux (peptic contact ulcer), and vocal cord abuse related to shouting, coughing, etc.1,2,3,4,5 and 6 Patients tend to be older than 30 years and most are men. Most patients present with hoarseness and may be noted to have low-pitched voices and frequent coughing. Occasionally, patients may present with severe pain. The posterior vocal cords are usually ulcerated; however, some lesions can have a marked nodular or polypoid appearance simulating neoplasia.2,5,6 Although the epithelium is frequently ulcerated and covered with a fibrinous exudate (Fig. 15.1, e-Fig. 15.1), lesions can be covered by a proliferative epithelium that resembles pseudoepitheliomatous hyperplasia. Abundant granulation tissue is seen either at the ulcer site or immediately beneath the squamous epithelium and comprises the bulk of the lesion (Fig. 15.2, e-Fig. 15.2). Occasionally, atypical stromal cells may be seen; however, stromal mitotic figures are rare (e-Fig. 15.3).6 The granulation tissue is composed of numerous capillaries and a mixed inflammatory infiltrate. It should not have the lobular growth pattern typical of lobular capillary hemangiomas
that are found in the mouth and sinonasal area. Indeed, true lobular capillary hemangiomas or pyogenic granulomas of the larynx either do not occur or are extremely rare.7
that are found in the mouth and sinonasal area. Indeed, true lobular capillary hemangiomas or pyogenic granulomas of the larynx either do not occur or are extremely rare.7
TABLE 15.1 Nonneoplastic Diseases of the Larynx | ||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||
FOREIGN BODY REACTION
Foreign body reactions within the larynx are most often iatrogenic.5,8,9,10 and 11 The most extensively studied reaction is that secondary to Teflon injection.5,8,11 Teflon, or polytetrafluoroethylene, is a synthetic substance that can be injected into a paralyzed vocal cord to restore glottic competence. In general, this induces a localized foreign body giant cell reaction that is walled off by fibrous tissue. Occasionally, the material may infiltrate
into the surrounding tissues. The resultant foreign body reaction may form a mass that bulges into the larynx. Histologically, clusters and sheets of multinucleated foreign body-type giant cells that contain birefringent clear material are present with intermixed chronic inflammation and fibrosis (Fig. 15.3, e-Figs. 15.4 and 15.5). Other materials, including
silicone, Gore-Tex, and titanium, may be used for vocal cord medialization.9,10 These foreign materials are generally not absorbed and induce surrounding fibrosis and chronic inflammation with a variable foreign body reaction.
into the surrounding tissues. The resultant foreign body reaction may form a mass that bulges into the larynx. Histologically, clusters and sheets of multinucleated foreign body-type giant cells that contain birefringent clear material are present with intermixed chronic inflammation and fibrosis (Fig. 15.3, e-Figs. 15.4 and 15.5). Other materials, including
silicone, Gore-Tex, and titanium, may be used for vocal cord medialization.9,10 These foreign materials are generally not absorbed and induce surrounding fibrosis and chronic inflammation with a variable foreign body reaction.
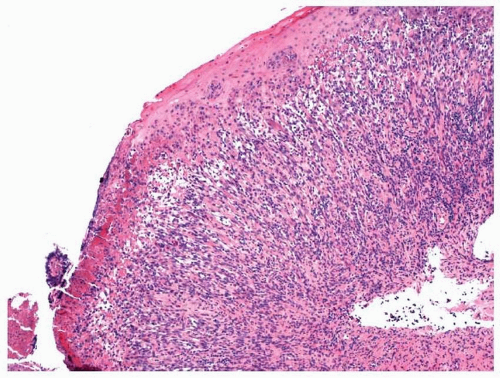 FIGURE 15.1 A contact ulcer with eroded epithelium and a fibrinous exudate. |
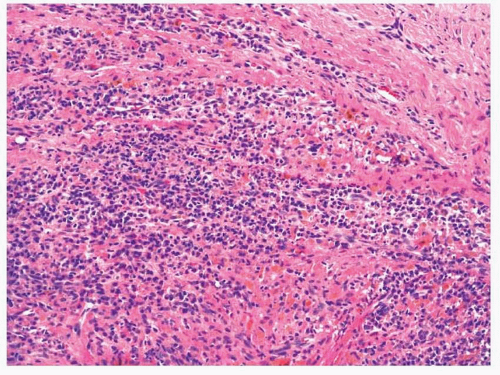 FIGURE 15.2 Abundant chronic inflammation can be seen within the stroma of a contact ulcer. |
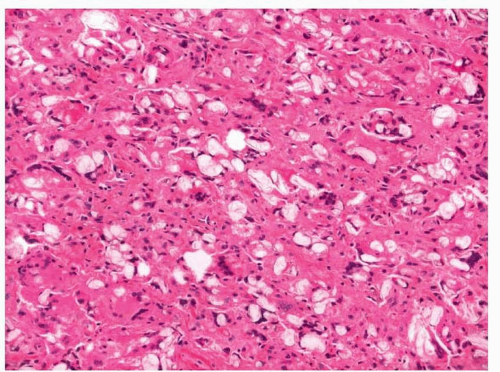 FIGURE 15.3 Foreign body giant cells with foreign material are observed in this reaction to Teflon. |
INFECTIOUS DISEASES
The larynx may be infected by a great host of organisms that more commonly involve the lungs or sinonasal area. Many of these entities present as mass lesions and an infectious etiology is often unsuspected. Pathologists, however, should be well aware of these lesions, as the correct diagnosis can spare a patient unnecessary treatment.
Tuberculosis
Patients with long-standing tuberculosis are frequently noted to have laryngeal involvement in advanced disease.12 Since the advent of effective antituberculosis treatments, laryngeal involvement has only seldom been reported and, when reported, it has been described as a mimic of laryngeal carcinoma.12,13,14,15 and 16 As such, patients are older, usually in their fifth or sixth decade of life, and typically present with hoarseness and a solitary laryngeal mass that frequently involves the vocal cords. Only rarely do patients have more developed pulmonary symptoms (although pulmonary disease may be present). Grossly, the lesions are sometimes ulcerated and can appear granular and nodular. Laryngeal disease shares
the histologic features of tuberculosis found elsewhere, with caseating granulomatous inflammation and Langhans giant cells (Fig. 15.4, e-Fig. 15.6).15 Histochemical and immunohistochemical staining for acidfast bacilli can sometimes be helpful for distinguishing this disease from other granulomatous diseases of the laynx. (Table 15.2).
the histologic features of tuberculosis found elsewhere, with caseating granulomatous inflammation and Langhans giant cells (Fig. 15.4, e-Fig. 15.6).15 Histochemical and immunohistochemical staining for acidfast bacilli can sometimes be helpful for distinguishing this disease from other granulomatous diseases of the laynx. (Table 15.2).
TABLE 15.2 Granulomatous Diseases of the Larynx | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
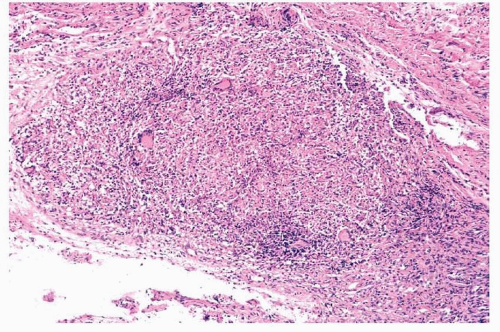 FIGURE 15.4 Laryngeal tuberculosis appears similar to tuberculosis seen at other sites in the body with necrotizing granulomatous inflammation. |
Leprosy
The larynx is the second most common site in the head and neck after the sinonasal area to be affected by leprosy.15 Within the larynx, the lesions are painless and develop supraglottically and then progress to the glottis. The lesions may appear nodular and ulcerated, and infection can eventually lead to laryngeal stenosis. Histologically, the process is similar to that noted in the nasal area and is usually composed of a mixture of chronic inflammatory cells and large, foamy macrophages. Mycobacterium leprae (Hansen’s bacillus) may be identified by histochemical staining for acidfast bacilli.
Fungal Infections
Fungal infections of the larynx are uncommon, are frequently associated with widespread disease, and are most often found in immunocompromised patients. Laryngeal histoplasmosis may present as either multiple nodular or ulcerated lesions.15,17 These lesions may also appear somewhat granular and verrucoid. Patients frequently have involvement of the vocal cords with concomitant disease within the mouth.17 The microscopic appearance is variable. A mixture of acute and chronic inflammation is usually present with numerous large macrophages with abundant granular cytoplasm. Some cases may have well-formed caseating granulomatous inflammation and others may be devoid of granulomata. The overlying epithelium is often ulcerated; however, marked pseudoepitheliomatous hyperplasia may be present and should not be confused with squamous cell carcinoma. Although the organisms can frequently be seen on routine hematoxylin and eosin (H&E)-stained material, silver or periodic acid-Schiff (PAS) staining can also be used to highlight their presence (Fig. 15.5, e-Fig. 15.7).
Extrapulmonary involvement in blastomycosis is common. When it affects the larynx, patients typically present with hoarseness, with or without coexistent pulmonary or cutaneous lesions.15,18,19 Laryngeal blastomycosis is typically described as erythematous, irregular, and granular lesions that may also appear verrucoid. Histologically, these lesions are characterized by pseudoepitheliomatous hyperplasia with mixed acute and chronic inflammation. Langhans giant cells are usually seen, together with intraepithelial microabscesses and granulomata, some of which may be suppurative (Fig. 15.6). The causative organism, Blastomyces dermatitidis, can usually be identified with H&E-stained material or with silver or PAS stain. It characteristically demonstrates broad-based budding (e-Figs. 15.8 and 15.9).
Rarely, Coccidioides immitis can involve the larynx.20,21 Patients with laryngeal infection almost always have coexistent pulmonary disease. For an unknown reason, most reported cases have affected blacks. Patients typically present with hoarseness and a sore throat. Grossly, the lesions most often involve the cords and typically appear granular and nodular.
Frequently, the differential diagnosis includes squamous cell carcinoma or tuberculosis. Histologically, pseudoepitheliomatous hyperplasia is often seen with mixed inflammation and giant cells, with or without well-formed granulomata. The characteristic spherules and endospores of the organisms can be seen both by conventional H&E stain and by silver or PAS stain.
Frequently, the differential diagnosis includes squamous cell carcinoma or tuberculosis. Histologically, pseudoepitheliomatous hyperplasia is often seen with mixed inflammation and giant cells, with or without well-formed granulomata. The characteristic spherules and endospores of the organisms can be seen both by conventional H&E stain and by silver or PAS stain.
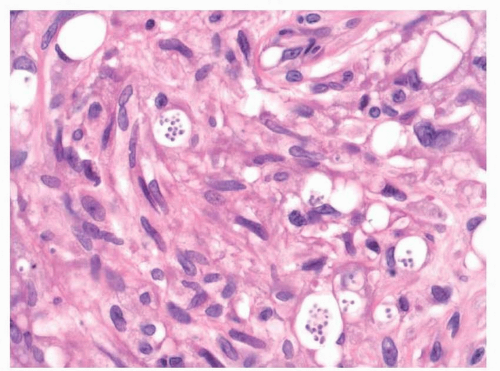 FIGURE 15.5 Intracellular organisms consistent with Histoplasma are seen in this case of laryngeal infection. |
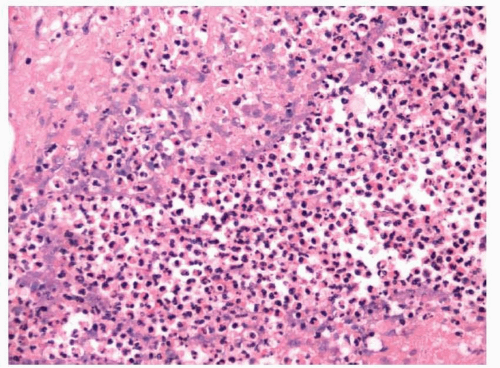 FIGURE 15.6 This case of laryngeal blastomycosis has numerous suppurative granulomata. |
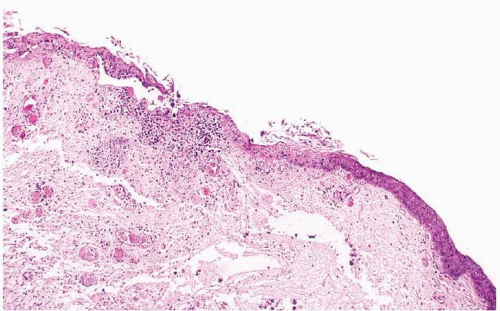 FIGURE 15.7 Surface erosion with numerous pseudohyphae is seen in this case of laryngeal candidiasis. |
Other fungal organisms may also involve the larynx, and infections secondary to Cryptococcus neoformans, Candida albicans, Aspergillus spp., Rhinosporidium seeberi, and Paracoccidioides spp. have been reported (Fig. 15.7, e-Fig. 15.10).22,23,24,25 and 26 Each of these may be seen in immunocompromised patients with or without more widespread disease. Occasionally, they may present in apparently immunocompetent patients without evidence of disease elsewhere. Patients typically present with hoarseness and have granular and sometimes exophytic lesions involving the larynx. As with other fungal infections, pseudoepitheliomatous hyperplasia is often present (e-Fig. 15.11). A mixed inflammatory infiltrate is typically seen, which can involve the epithelium. Fungal organisms may be identified on routine and special stains. A mucicarmine stain can be used to highlight the capsule of C. neoformans (e-Fig. 15.12).
Bacterial Infections
Bacterial infection of the supraglottic larynx and hypopharynx is now rare, thanks to vaccination for Haemophilus influenzae and Corynebacterium diphtheriae.




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
