Nonneoplastic Diseases of the Salivary Glands
Rohan R. Walvekar
Matthew A. Bowen
Nonneoplastic disorders of the salivary gland encompass a wide range of disease processes that can affect the salivary glandular and the ductal system. These can be acute or chronic in their presentation and can also be broadly classified into inflammatory and noninflammatory disorders. Nonneoplastic disease processes affect both the major and minor salivary glands; however, they occur more commonly in the major salivary glands. Classification of the disease process is of importance. Treatment can be targeted toward a more generalized disease process affecting the entire gland (e.g., antibiotics in acute suppurative sialadenitis) or a locally directed treatment aimed at improving salivary flow and function (e.g., stone removal for an obstructed salivary gland). A history and physical examination allows differentiation of lesions or disease processes into their appropriate classification. Additional laboratory studies, special tests, imaging studies, and rarely a pathologic analysis via a diagnostic biopsy may be required to make a specific diagnosis. Extensive testing is rarely necessary to classify nonneoplastic disorders of the salivary gland. This chapter provides an overview of a variety of common nonneoplastic disease processes and also introduces the emerging field of sialendoscopy and its impact on the management of nonneoplastic salivary gland diseases (SGDs).
ACUTE INFLAMMATORY LESIONS
Acute Suppurative Sialadenitis
Acute sialadenitis is a bacterial infection of the salivary glands. High bacterial loads in the oral cavity provide opportunity for infection of the salivary glands. Normal salivary flow is protective against retrograde colonization and overgrowth of bacteria in the salivary ducts and parenchyma. Saliva has antimicrobial properties due to the presence of lysosomes, IgA antibodies, and sialic acid. These proteins are more concentrated in the submandibular, sublingual, and minor salivary glands as compared to the less viscous saliva in the parotid gland. Acute sialadenitis was first reported in 1828. It gained increased attention when President Garfield died from acute parotitis following abdominal surgery in 1881. The current incidence of acute sialadenitis has been reported at 0.02% of hospital admissions (1), with the parotid gland being most commonly affected. Thirty to forty percent of these episodes can occur in the postoperative patient. The disease occurs with the highest incidence after gastrointestinal procedures between postoperative day 3 and 7.
Salivary stasis, reduced flow, and obstruction can be precipitating events for acute sialadenitis. Dry mouth is seen with increasing age affecting up to 30% of patients over the age of 65 years. This could be attributed to a disease process but can also be subsequent to prescribed medications. Eighty percent of prescribed medications cause some degree of xerostomia and more than 400 medications can cause some degree of salivary gland dysfunction. Consequently, it is not surprising acute sialadenitis most frequently occurs in sixth or seventh decade of life. However, all age groups can be affected. A decrease in saliva production can be caused by multiple medical conditions and drug therapies, increasing the risk for acute suppurative sialadenitis. Examples include diuretic therapy for hypertension, osmotic diuresis from diabetes mellitus, and postsurgical fluid shift, especially after gastrointestinal procedures. Debilitated individuals who rely on caregivers for hydration and oral hygiene are also at risk for acute suppurative sialadenitis (Table 48.1). Antisialogogue medications and physical obstruction of salivary flow due to sialolithiasis or salivary duct stricture result in salivary stasis and can cause acute sialadenitis.
TABLE 48.1 SYSTEMIC AND EXOGENOUS SOURCES OF SALIVARY DYSFUNCTION | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
The classical presentation of acute suppurative sialadenitis is the sudden onset of diffuse enlargement of the involved gland with associated induration and tenderness (Fig. 48.1). A detailed history may reveal underlying risk factors or etiology. The gland should be palpated when possible. Bimanual palpation is more effective for the submandibular gland. Palpation may often reveal obstructing salivary stones. Palpation and massage of the gland may result in the expression of purulent exudate from the papilla of the involved gland. The unaffected glands should be palpated while the papillae are visualized to observe for expression and consistency of normal saliva. The purulent exudate should be cultured for aerobic and anaerobic bacteria, and a specimen for Gram staining.
Historically, Staphylococcus aureus has been attributed as the causative microbe in up to 90% of cases of suppurative sialadenitis. Other aerobic organisms implicated include Streptococcus pneumoniae, Escherichia coli, and Haemophilus influenzae. More recent microbiology studies have revealed that while S. aureus remains the most common bacteria; anaerobic, gram-negative, and polymicrobial infections are not uncommon (2,3). The most common anaerobic organisms are Bacteroides melaninogenicus and Streptococcus micros. In one study, anaerobic bacteria were isolated in 64% of cases, and β-lactamase-producing organisms were isolated from 51% of cases (3). Histologic examination shows glandular destruction with abscess formation. Ductal wall erosion is seen with associated penetration of glandular parenchyma.
 Figure 48.1 Acute suppurative parotitis affecting the left parotid gland. |
Initial treatment consists of antibiotics, warm compresses, gland massage, and sialogogues. Aerobic and anaerobic cultures are obtained to direct antimicrobial therapy. Empiric treatment with penicillinase-resistant antistaphylococcal antibiotic should be initiated while awaiting cultures. Efforts should be made to correct causative risk factors or comorbidities, such as uncontrolled diabetes, which can compromise treatment response. Oral or parenteral hydration should be given as appropriate. Computed tomography (CT) or ultrasound imaging is useful if an abscess or regional spread of infection is suspected. Sialography is contraindicated. Similarly, sialendoscopy, a relatively new diagnostic and therapeutic technique, is also contraindicated in this setting (4). Imaging can detect obstruction due to sialolithiasis or salivary strictures that can be addressed once the active infection has subsided.
In the event of abscess formation, incision and drainage is indicated and can be performed using a modified Blair incision to expose the parotid capsule. A hemostat can then be used to spread in the direction of the facial nerve fibers to enter the abscess cavity. Management of the abscess cavity follows standard recommendations that include packing or placement of a drain based on each individual case scenario. CT-guided or ultrasonographyguided needle aspiration may also be an option that can obviate open surgery. Treatment initiation usually results in rapid improvement within 24 to 48 hours. If the patient does not respond to therapy, antibiotic resistance, immune status, and abscess formation should be considered. Mortality rates up to 20% have been reported in the literature.
Mumps
The most common acute viral infection of the salivary glands is mumps. Prior to the release of the mumps vaccine in 1967, the incidence of mumps in the United States was as high as 300,000 cases per year and the most common cause of parotid swelling. This dramatically decreased to 266 reported cases in 2001 (5). Subsequently, the demographics of mumps shifted from being a disease of childhood to most commonly affecting young adults. Several outbreaks in the United States and other vaccinated countries have been reported in recent years (6,7,8). Prodromal symptoms include fever, malaise, myalgia, and anorexia.
The onset of parotitis usually occurs within 24 hours but may follow up to a week later. Parotitis is generally bilateral, but may be unilateral. Other salivary glands, such as the submandibular gland and sublingual gland, are less frequently involved and are almost never solely involved. Other manifestations include orchitis, aseptic meningitis, pancreatitis, and myocarditis. Sensorineural hearing loss is a rare complication. Diagnosis is made by confirmation of antibodies to the mumps S and V antigens. Diagnosis can also be made by isolating the virus from the cerebrospinal fluid (CSF) during the first 3 days of clinical symptoms for patients presenting with aseptic meningitis. Virus is also present in the saliva for approximately 1 week starting 2 to 3 days before onset of parotitis. Viral cultures of urine will also be possible for the first 2 weeks of illness (9,10,11). PCR or viral cultures can also be used to detect the virus. Therapy is symptom based. Chronic obstructive sialadenitis may develop many years after the acute episode of mumps.
The onset of parotitis usually occurs within 24 hours but may follow up to a week later. Parotitis is generally bilateral, but may be unilateral. Other salivary glands, such as the submandibular gland and sublingual gland, are less frequently involved and are almost never solely involved. Other manifestations include orchitis, aseptic meningitis, pancreatitis, and myocarditis. Sensorineural hearing loss is a rare complication. Diagnosis is made by confirmation of antibodies to the mumps S and V antigens. Diagnosis can also be made by isolating the virus from the cerebrospinal fluid (CSF) during the first 3 days of clinical symptoms for patients presenting with aseptic meningitis. Virus is also present in the saliva for approximately 1 week starting 2 to 3 days before onset of parotitis. Viral cultures of urine will also be possible for the first 2 weeks of illness (9,10,11). PCR or viral cultures can also be used to detect the virus. Therapy is symptom based. Chronic obstructive sialadenitis may develop many years after the acute episode of mumps.
Other Viral Diseases
Other viruses have been implicated in acute viral parotitis, including cytomegalovirus, Coxsackie A and B, cytopathic human orphan virus, echoviruses, influenza A, and lymphocytic choriomeningitis virus (12). Treatment of all viral infection is symptomatic. Added antibacterial therapy is indicated in the presence of superimposed infections.
HIV
Several salivary gland manifestations may occur in patients with human immunodeficiency virus (HIV). Diffuse gradual enlargement of the salivary glands may be seen and has been termed HIV-associated SGD (HIV-SGD). HIV-SGD may be encountered at any time in the HIV disease process, and may be the presenting symptom. The parotid gland is most commonly affected. Xerostomia can be present, mimicking Sjögren syndrome (SS). Other salivary gland manifestations of HIV include Kaposi sarcoma and lymphoma. While non-HIV-related lymphoepithelial (LE) cysts also occur, a significantly increased incidence of parotid LE cysts has occurred since the emergence of HIV. LE cysts histopathologically resemble branchial cleft cysts with an epithelial-lined cyst within a lymphoid stroma. Dave et al. (13) propose a classification system for lymphocytic parotid gland enlargement in HIV-positive pediatric patients: (a) parotid gland lymphadenopathy, (b) benign LE lesion, and (c) benign LE cysts. Treatment consists of observation and antiretroviral therapy. Needle aspiration can offer temporary symptomatic relief for large cysts, but recurrence is expected. For severe symptomatic cases, or for cosmetic reasons, sclerotherapy is a reasonable option (13). Sclerotherapy agents used include alcohol (14), doxycycline (15), and sodium morrhuate (16). Surgery or radiation therapy should be reserved for resistant cases (13).
GRANULOMATOUS INFECTIONS OF THE SALIVARY GLANDS
Tuberculosis of the Salivary Glands
Although cervicofacial involvement is the most common extrapulmonary manifestation of Mycobacterium tuberculosis infection (17), salivary gland involvement by far is rare. Older children and adults are most commonly affected. Parotid involvement is most common with primary M. tuberculosis infection, while in disseminated pulmonary infections, the submandibular gland is more commonly involved. Most cases of primary tuberculosis of the salivary gland are believed to arise from a focus of infection in the tonsil or teeth. The presentation is that of an enlarging firm parotid mass that is identical to a neoplasm on imaging (18). Clinical presentation may mimic acute inflammatory sialadenitis and diagnosis requires positive acid-fast salivary stain and purified protein derivative (PPD) test. However, PPD test is unreliable because of increasing incidence of nontuberculous mycobacterial (NTM) infections that give a negative PPD test. Fine needle aspiration can reveal caseous necrosis in some cases. PCR of fine needle aspirate is highly sensitive (18), but may not be easily obtained. After the diagnosis is made, treatment is the same as for any tuberculosis infection. In resistant cases, excision may be necessary and will be curative.
NTM are more common than M. tuberculosis in cervicofacial mycobacterial infections. Salivary gland involvement is still rare relative to involvement of cervical lymph nodes. Mycobacterium kansasii, Mycobacterium scrofulaceum, and Mycobacterium avium are the most commonly encountered NTM. These organisms are common in soil, water, and food, and are carried by domestic and wild animals. NTM infection is most commonly encountered in children younger than 5 years old. The typical presentation is tender induration in the region of the salivary gland that fails antibiotic therapy. The overlying skin develops thinning and adherence to the infected gland, with a characteristic violaceous hue. Abscess formation is common. Fine needle aspiration biopsy carries a risk of fistula formation, but is useful for microscopic evaluation for acid-fast bacilli in the aspirate. Culturing NTM takes weeks and is frequently negative, but useful if positive. Antibiotic treatment with clarithromycin or other antibiotics can be attempted, but often results in several weeks to months of treatment, during which the patient remains symptomatic and fistulization or repeated abscess formation must be managed. Therefore, complete gland excision of the affected gland is advocated as the definitive treatment (i.e., parotidectomy with facial nerve preservation).
Cat-Scratch Disease
Cat-scratch disease is caused by the gram-negative bacillus Bartonella henselae. A local infection at the scratch site is followed 1 to 2 weeks later by lymphadenopathy in the
draining lymph nodes. Parotid or submandibular lymph nodes may be involved. Lymph node enlargement progresses over 1 to 2 weeks and can persist for 2 to 3 months. Abscess formation may occur. Observation is usually sufficient with reassurance that the lymphadenopathy will spontaneously resolve. If the patient is highly symptomatic, antibiotics can be prescribed. Rifampin, erythromycin, gentamycin, azithromycin, and ciprofloxacin are all therapeutic options (19). Actinomycosis may also involve the salivary glands. Long-term penicillin therapy is combined with incision and drainage and excision of necrotic tissue for symptom control.
draining lymph nodes. Parotid or submandibular lymph nodes may be involved. Lymph node enlargement progresses over 1 to 2 weeks and can persist for 2 to 3 months. Abscess formation may occur. Observation is usually sufficient with reassurance that the lymphadenopathy will spontaneously resolve. If the patient is highly symptomatic, antibiotics can be prescribed. Rifampin, erythromycin, gentamycin, azithromycin, and ciprofloxacin are all therapeutic options (19). Actinomycosis may also involve the salivary glands. Long-term penicillin therapy is combined with incision and drainage and excision of necrotic tissue for symptom control.
Sarcoidosis
Sarcoidosis is a granulomatous disorder with many systemic manifestations encompassing every organ system. Parotid gland involvement has been reported in 6% to 30% of patients with sarcoidosis (20,21,22). One notable presentation is that of uveoparotid fever (Heerfordt syndrome), which is characterized by uveitis, parotid enlargement, and facial paralysis, and has been reported to affect 0.3% of patients with sarcoidosis (23). Parotid swelling can last months to years and eventually resolves spontaneously. Submandibular, sublingual as well as minor salivary gland involvement may also occur. Biopsy of the minor salivary glands may establish diagnosis. Corticosteroids are effective, especially in the acute phase and for the management of facial paralysis. Uveitis can lead to glaucoma.
Sjögren’s Syndrome
Sjögren’s Syndrome (SS) is an autoimmune disorder with symptoms including xerostomia, dry eyes, and salivary gland enlargement (Fig. 48.2). SS is common and underdiagnosed. In the United States, approximately 1 million people have an established diagnosis, with an estimated 2 to 4 million people being affected. The male:female ratio is 9:1. SS affects people of all ages, but is typically diagnosed between the fourth and sixth decades. Primary SS affects the exocrine glands alone. In secondary SS, there is a coincidence of another autoimmune disorder, such as rheumatoid arthritis or systemic lupus erythematosus. The pathophysiology is poorly understood, but leads to B and T cell-mediated damage to exocrine glands. Non-organ-specific autoantibodies are present in approximately 60% of cases (24). These include rheumatoid factor (RF), antinuclear antibodies, and antibodies to the small RNAprotein complexes Ro/SS-A and La/SS-B. The histopathologic hallmark of SS is focal dense lymphocytic infiltration with little or no surrounding edema or fibrosis. CD4+ T cells predominate, with B cells accounting for approximately 20% of cells. Infiltration begins by surrounding glandular ducts and expanding to replace acinar epithelial cells. Acinar loss leads to decreased glandular function (25). A wide range of systemic and other organ-specific manifestations are possible. Fatigue and arthritis are common. Interstitial pneumonitis, rash or dry skin, achlorhydria, hepatosplenomegaly, genital dryness, myositis, and pancreatitis may be encountered. SS patients have been found to have a 44 times higher relative risk of developing lymphoma, which may present early or late in the disease. Predictors of lymphoma development include persistent enlargement of the parotid glands, splenomegaly, lymphadenopathy, palpable purpura, leg ulcers, low C4 level, mixed monoclonal cryoglobulinemia, and cross-reactive idiotypes of monoclonal RFs (26). Although the most prominent ocular symptom of the disease is dry eye, this is not a frequent presenting symptom. On the contrary, dry mouth (xerostomia) is a more common presenting complaint (27). Dry mouth is a debilitating feature of the disease and affects overall quality of life of these patients. Examination often denotes a dry oral mucosa with minimal expression of saliva when the parotid or submandibular glands are massaged. Placement of a tongue blade in the oral cavity causes it to adhere to the buccal mucosa confirming xerostomia.
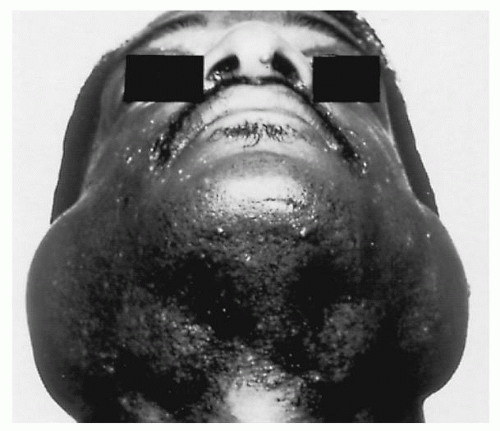 Figure 48.2 SS in patient with acquired immunodeficiency syndrome-related complex. |
Diagnostic criteria have been established (European-American Consensus Group Modification of the European Community Criteria for Sjögren’s Syndrome) based on the presence of four of the following six criteria: symptoms of dry eye, signs of dry eye (abnormal results of Schirmer test), symptoms of dry mouth, signs of abnormal salivary glandular function, minor salivary gland biopsy focus score of greater than 1, and presence of SS-A or SS-B antibodies (28). Sensitivity and specificity range from 85.1% to 93.5% and 93.3% to 94.0%, respectively. Imaging such as CT or magnetic resonance (MRI) of the parotid gland can demonstrate speckled calcification that is often encountered in patients with SS having parotid involvement (Fig. 48.3).
Treatment for SS involves symptomatic treatment for xerostomia and prevention of ocular or dental damage. Salivary production can be improved by stimulation of
existing salivary flow. This can be done by use of sugarless or sour candies, fruit slices such as peaches or nectarines. Citrus flavored sugarless tablets (“Salivasure,” Scandinavian Health and Beauty Products, Perkasie, PA) are available. Malic acid in the tablets and maltose lozenges also stimulate salivary sections and reduce symptoms of oral dryness (29). Pilocarpine, a muscarinic-cholinergic agonist acting predominantly on M3 receptors, is a systemic sialogogue that may be prescribed and does provide symptom relief. However, side effects including sweating, flushing, and increased urination are common and can be dose-limiting. Cevimeline is a derivative of acetylcholine with a higher affinity for M1 and M3 receptors on the salivary glands (30,31) and has been shown to be of benefit in a doubleblinded placebo controlled randomized study that studied the drug randomly in 197 patients with primary and secondary SS (32).
existing salivary flow. This can be done by use of sugarless or sour candies, fruit slices such as peaches or nectarines. Citrus flavored sugarless tablets (“Salivasure,” Scandinavian Health and Beauty Products, Perkasie, PA) are available. Malic acid in the tablets and maltose lozenges also stimulate salivary sections and reduce symptoms of oral dryness (29). Pilocarpine, a muscarinic-cholinergic agonist acting predominantly on M3 receptors, is a systemic sialogogue that may be prescribed and does provide symptom relief. However, side effects including sweating, flushing, and increased urination are common and can be dose-limiting. Cevimeline is a derivative of acetylcholine with a higher affinity for M1 and M3 receptors on the salivary glands (30,31) and has been shown to be of benefit in a doubleblinded placebo controlled randomized study that studied the drug randomly in 197 patients with primary and secondary SS (32).
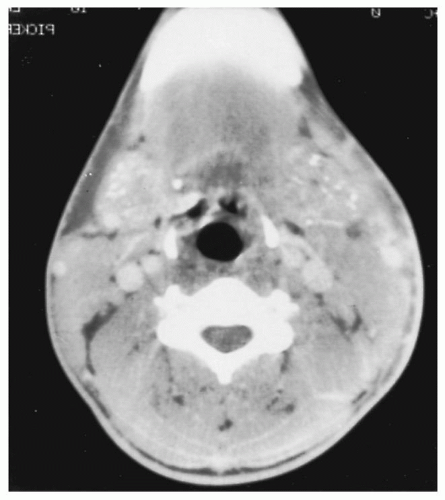 Figure 48.3 CT of a patient with SS showing stippled calcification. |
Oral secretions can be replaced by encouraging the patient to take frequent sips of water. Artificial saliva preparations that contain methyl cellulose provide more viscosity and lubrication than water. Fluoride treatments can be used to reduce dental caries. In addition, patients should be counseled to take meticulous care of dentition with frequent (at least once every 6 months) visits to the dentist for cleaning and plaque control (33). Novel therapeutic options such as sialendoscopy with irrigation of the salivary ductal system with or without instillation of steroids has also been shown to demonstrate benefit in terms of improvement of salivary gland discomfort, reduced incidence of salivary gland swelling, and improved salivation (34). The authors’ personal experience in this area suggests a potential in the future for a combined therapeutic options that would involve salivary endoscopy with irrigation with or without steroid injections in conjunction with medical therapy to optimize and individualize treatment protocols.
Chronic Sialadenitis
Chronic sialadenitis is characterized by recurrent inflammation and pain in the major salivary glands. Precipitating events include the triad of stasis, obstruction, and reduced salivary flow rate. Sialolithiasis, salivary duct stricture, external duct compression, systemic disease (e.g., SS), or states (e.g., dehydration) may be causative. As seen with acute suppurative sialadenitis, the parotid gland is more commonly involved. Repeated glandular infection results in permanent damage to the salivary gland characterized by sialectasia, ductal ectasia, and progressive acinar destruction combined with a lymphocytic infiltrate. Symptoms are often exacerbated by eating. The structural changes with chronic repeated infections result in reduced function. Xerostomia develops in up to 80% of patients as the salivary glands become progressively damaged. Chronic inflammation damages the gland, with findings of ductal ectasia, acinar destruction, and a lymphocytic infiltrate of the parenchyma.
Patients with chronic sialadenitis present with a history of recurrent painful swelling of the affected salivary gland(s) that is often aggravated by eating. Physical examination confirms asymmetric, firm, and occasionally tender glands. The glands can also be atrophic and hard in consistency that can be either diffuse or discrete. In the latter case, imaging and needle biopsy may be required to rule out a coincidental neoplasm. Examination of the oral cavity must be performed to assess xerostomia, quality and consistency of the saliva, patency of the duct opening at the papilla, and to perform bimanual palpation of the glands. Examination may often reveal a calculus that may be palpable in the floor of the mouth or over the masseter muscle. Ultrasonography is a valuable adjunct to physical examination and can help detect salivary stones that are not palpable clinically, as well as neoplastic process and strictures.
Gland massage during exam typically reveals decreased salivary output. The consistency of saliva may also vary and can be more tenacious as compared to a normal water-like consistency of saliva. Changes in saliva occur as a result of the chronic inflammatory process. During acute episodes, sodium and chloride values approach those in the serum; glucose is elevated while phosphate levels decrease. Levels of plasma derived IgA, IgG, IgM, albumin, and transferrin are increased, as well as myeloperoxidase, lactoferrin, and lysozyme, which are derived from inflammatory infiltrate or the acini. The pattern of immunoglobulins in the saliva shifts from IgA-predominance (normal for saliva) to IgG-predominance. After the acute episodes have resolved, the increased levels of sodium and proteins in the saliva remain in patients with chronic sialadenitis. However, these levels normalize in patients with noninflammatory enlargements.
The diagnostic workup should include imaging with a CT with and without intravenous contrast to evaluate for calculi or neoplasms within the gland. Sialography may be useful to detect ductal abnormalities such as ectasia or strictures. More recently, several authors have described specialized MRI protocols to view the salivary gland ducts, termed MRI sialography, which may prove useful as the technique is developed (35,36,37). Workup for SS or indolent mycobacterial infections should be considered.
After excluding treatable causes, initial treatment for chronic sialadenitis includes sialogogues, hydration, massage, and antibiotics during acute exacerbations. When conservative management is insufficient, several procedures have potential to decrease symptomatic burden. However, results are inconsistent, which can lead to frustration for the patient and physician. Treatment options include papillary dilation (with or without sialodochoplasty), steroid injection into the duct, dilation of ductal strictures, ductal ligation to promote gland atrophy, gland irradiation, and surgical gland extirpation. Sialendoscopy has been gaining increasing attention as a diagnostic and therapeutic tool, which may spare gland removal (38).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


