41 Non-neoplastic Laryngeal Pathology • Paroxysmal laryngospasm • Laryngeal stenosis • Laryngeal carcinoma • Vocal cord nodules • Globus pharyngeus • Laryngomalacia • Reflux symptom index – Hoarseness or problem with your voice – Clearing your throat – Excessive mucous or postnasal drip – Difficulty swallowing food, liquid, or pills – Coughing after you ate or lying down – Breathing difficulties or choking episodes – Troublesome or annoying cough – Sensation of something sticking in your throat or a lump in your throat – Heartburn, chest pain, indigestion, or stomach acid coming up • Reflux finding score – Infraglottic oedema: 0, absent; 2, present – Ventricular obliteration: 0, absent; 2, present; 4, complete – Erythema: 0, none; 2, arytenoids; 4, diffuse – Laryngeal oedema: 0, none; 1, mild; 2, moderate; 3, severe; 4, polypoid – Post-commissure hypertrophy: 1, mild; 2, moderate; 3, severe; 4, obstructing – Granuloma/granulation tissue: 0, absent; 2, present – VF oedema: 0, none; 1, mild; 2, moderate; 3, severe; 4, polypoid – Thick mucus: 0, absent; 2, present • Acute <3 weeks • Self-limiting • Erythema and oedema of vocal cord • Typically affects 18- to 40-year-olds • Aetiology includes vocal misuse, infection typically viral • Treatment: humidification, voice rest, Cochrane database showed no evidence for antibiotics • Chronic >3 weeks • Fluctuating dysphonia, chronic cough (night>day), laryngospasm secondary to mucous strands • Consider occupational history including exposure to toxic substances • Consider drug history: e.g., diuretics may dry mucosa, calcium channel blockers/nitrates may predispose to gastro-eosophageal reflux disease (GORD) secondary to reduction in tone of lower oesophageal sphincter • Autoimmune causes include: – Hemoptysis – Stridor – Upper airway narrowing – May have tender larynx and develop tracheomalacia • Systemic cutaneous causes include: • Treatment: – Avoid stimulating/irritating factors, e.g., cigarette smoke – Treat underlying medical cause – Supportive measures include good oral hydration, steam inhalations – Biopsy to confirm diagnosis • Tuberculosis: posterior one-third larynx may mimic carcinoma • Sarcoidosis: granulomas, nodules, supraglottic swelling, vocal cord palsy • GPA: subglottis ± renal involvement • With or without anaphylaxis • Acute allergic histamine-mediated inflammatory reaction • Acute vascular dilation and capillary permeability • Oral and laryngopharyngeal structures frequently affected • Precipitating factors: – Penicillin – Aspirin – Other non-steroidal anti-inflammatory drugs – Angiotensin-converting enzyme inhibitors • Hereditary form: • Occult lymphoma leading to C1 esterase inhibitor deficiency can occur • Associated with pruritus • Hoarseness present when larynx involved • Treatment involves: • Treatment of hereditary form: • Upper motor neuron disorders: • Lower motor neuron disorders: • Aka laryngeal dystonia • Categories: • Characteristic features: • Treatment: • Adduction of VFs during inspiratory phase of respiration leading to total obstruction or stridor • Categories: • Muscular tension dysphonia • Voice fatigue syndrome • Abnormal loudness—e.g., with poor hearing • Abnormal pitch • False-cord phonation • Conversion reaction dysphonia—stressor related to onset of dysphonia • Malingering dysphonia • Pyschogenic dysphonia—stressor is in intermediate or distant past • Elective mutism • Psychogenic overlay • Air-filled dilatation of the saccule of the laryngeal ventricle • 80% male • Mean age 55 years • 30/year in the United Kingdom • Associated with ventricular cancer in 5 to 54% • Aetiology is unknown • Characteristic features:
41.1 Conditions Associated with Laryngopharyngeal Reflux
41.1.1 Extraesophageal Reflux Scoring Systems
 Validated and highly reproducible
Validated and highly reproducible
 9-item questionnaire
9-item questionnaire
 Scores per item vary from 0 (no problem) to 5 (severe problem)
Scores per item vary from 0 (no problem) to 5 (severe problem)
 Max score 45
Max score 45
 Score > 15 about 90% chance of supraoesophageal reflux
Score > 15 about 90% chance of supraoesophageal reflux
 Items:
Items:
 Validated
Validated
 8-item scale
8-item scale
 Based on fiberoptic laryngoscopic findings
Based on fiberoptic laryngoscopic findings
 Max score 26
Max score 26
 Score more >5 is abnormal
Score more >5 is abnormal
 Items:
Items:
41.2 Laryngitis
 Granulomatosis with polyangiitis (GPA)
Granulomatosis with polyangiitis (GPA)
 Amyloidosis
Amyloidosis
 Relapsing polychondritis
Relapsing polychondritis
 SLE—nodules, ulceration
SLE—nodules, ulceration
 Pemphigus
Pemphigus
 Stevens–Johnson syndrome
Stevens–Johnson syndrome
 Rheumatoid arthritis—paralysis of cricothyroid/arytenoids joint
Rheumatoid arthritis—paralysis of cricothyroid/arytenoids joint
 Conservative:
Conservative:
 Surgery:
Surgery:
41.3 Chronic Granulomatous Laryngeal Conditions
41.4 Angioedema
 Medications:
Medications:
 Food additives and preservatives
Food additives and preservatives
 Blood transfusions
Blood transfusions
 Infections
Infections
 Insect bites
Insect bites
 Deficiency of C1 esterase inhibitor
Deficiency of C1 esterase inhibitor
 Recurrent attacks of mucocutaneous oedema
Recurrent attacks of mucocutaneous oedema
 Adrenaline
Adrenaline
 Corticosteroids
Corticosteroids
 Antihistamines
Antihistamines
 Aminophylline
Aminophylline
 Airway management as required
Airway management as required
 Prophylactic danazol
Prophylactic danazol
 Fresh frozen plasma acutely
Fresh frozen plasma acutely
41.5 Neurological Disorders Causing Laryngeal Dysfunction
 Cerebrovascular accident (bilateral vocal cord involvement)
Cerebrovascular accident (bilateral vocal cord involvement)
 Parkinson disease (soft voice + other features of Parkinson disease)
Parkinson disease (soft voice + other features of Parkinson disease)
 Progressive supranuclear palsy
Progressive supranuclear palsy
 Pseudobulbar palsy—vascular and degenerative disease affecting corticobulbar tracts—bilaterally
Pseudobulbar palsy—vascular and degenerative disease affecting corticobulbar tracts—bilaterally
 Multiple sclerosis
Multiple sclerosis
 Myoclonus
Myoclonus
 Amyotrophic lateral sclerosis
Amyotrophic lateral sclerosis
 Myasthenia gravis—may have hypernasal speech/nasal regurgitation and dysphagia
Myasthenia gravis—may have hypernasal speech/nasal regurgitation and dysphagia
 Wallenberg syndrome (posterior ICA occlusion)
Wallenberg syndrome (posterior ICA occlusion)
 Postpolio syndrome
Postpolio syndrome
41.6 Functional Voice Disorders
41.6.1 Spasmodic Dysphonias (SD)
 Adductor SD—uncontrolled closing of VFs
Adductor SD—uncontrolled closing of VFs
 Abductor SD—prolonged VF opening for voiceless sounds extending into vowels
Abductor SD—prolonged VF opening for voiceless sounds extending into vowels
 VF tremor—modulations in pitch and loudness most evident during prolonged vowels
VF tremor—modulations in pitch and loudness most evident during prolonged vowels
 Onset between 30 to 50 years of age
Onset between 30 to 50 years of age
 60% female
60% female
 Aetiology unknown but believed to be part of a neurological problem with other dystonic features, e.g., blepharospasm, dyskinesias, oromandibular dystonia, or tremor
Aetiology unknown but believed to be part of a neurological problem with other dystonic features, e.g., blepharospasm, dyskinesias, oromandibular dystonia, or tremor
 Reflexive and emotional aspects of voice function unaffected, e.g., coughing, shouting, laughter
Reflexive and emotional aspects of voice function unaffected, e.g., coughing, shouting, laughter
 Diagnosed by listening to voice, which sounds like patient is straining on the toilet
Diagnosed by listening to voice, which sounds like patient is straining on the toilet
 Consider neurology referral to exclude other dystonias
Consider neurology referral to exclude other dystonias
 Medication—anticholinergics effective in 50% cases
Medication—anticholinergics effective in 50% cases
 Voice therapy
Voice therapy
 Surgery—Botox, though often requires multiple procedures
Surgery—Botox, though often requires multiple procedures
 Surgery on recurrent laryngeal nerve including avulsion procedure
Surgery on recurrent laryngeal nerve including avulsion procedure
41.6.2 Paradoxical Vocal Fold Movement
 Idiopathic focal dystonia
Idiopathic focal dystonia
 Part of Meige syndrome
Part of Meige syndrome
 Associated with or masquerading as asthma
Associated with or masquerading as asthma
 Exercise-induced stridor
Exercise-induced stridor
 Psychogenic
Psychogenic
 Associated with GORD
Associated with GORD
41.6.3 Disorders of Vocal Misuse
41.6.4 Psychogenic Voice Disorders
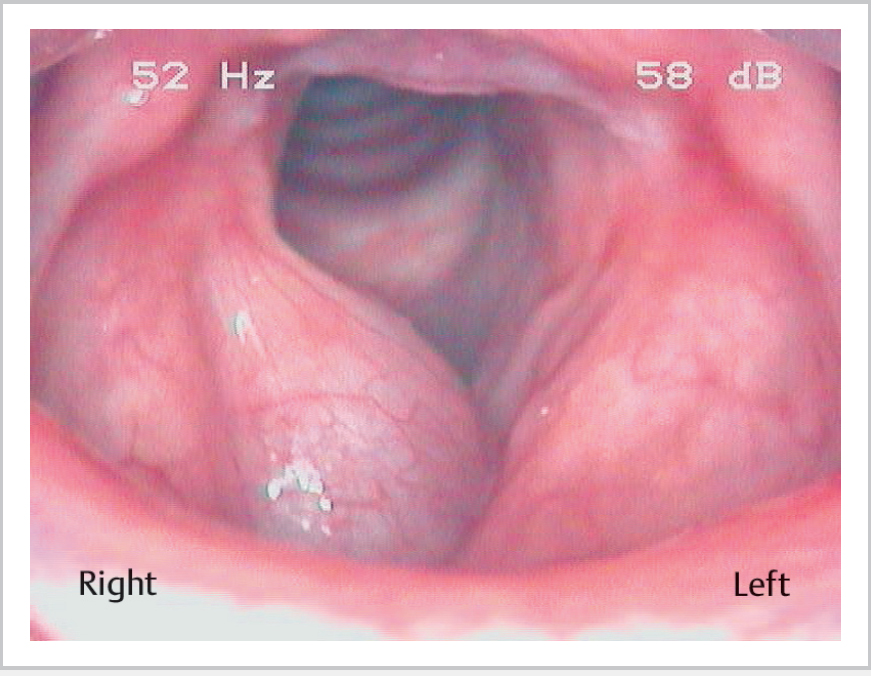
41.7 Laryngocele (Fig. 41.1)
 Neck swelling that increases with increased intralaryngeal pressure
Neck swelling that increases with increased intralaryngeal pressure
 Internal laryngocele presents hoarseness and dyspnea and stridor
Internal laryngocele presents hoarseness and dyspnea and stridor
 Smooth dilation at false-cord level
Smooth dilation at false-cord level
 Acute infection with pus formation (laryngopyocele): pain ± airway obstruction
Acute infection with pus formation (laryngopyocele): pain ± airway obstruction
 May expand internally through vallecula or externally (more common) through thyrohyoid membrane to neck or in combination
May expand internally through vallecula or externally (more common) through thyrohyoid membrane to neck or in combination
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


