Neurotologic Skull Base Surgery: Introduction
Although in widespread use, the term “skull base surgery” is somewhat of a misnomer. Only a minority of such procedures are undertaken to expose lesions actually located primarily within the skull base. Most procedures are conducted to expose deep-seated intracranial lesions situated either adjacent to the brainstem (eg, midbrain, pons, or medulla) or beneath the cerebral cortex. Previously, many such tumors were approached via simple openings in the calvaria, which require vigorous and often injurious degrees of brain retraction.
The fundamental principle in transbasal craniotomy is removal of the skull base bone to minimize the need for brain retraction. Although current techniques represent a major enhancement in our ability to control inaccessible tumors while minimizing morbidity, they are not panaceas. For example, experience has shown that these procedures are far more suitable for benign lesions (eg, meningiomas, schwannomas, and paragangliomas) and even for low-grade malignant growths (eg, chordomas and chondrosarcomas) than for high-grade malignant lesions (eg, squamous cell carcinoma, adenocystic carcinoma, and soft tissue sarcomas). Currently, more emphasis is placed on the preservation of function, especially cranial nerves, than on the necessity for radical resection in every case. The value of neurophysiologic nerve monitoring for motor nerves within the surgical field has become well established. In the developmental years of skull-base surgery, two-stage procedures were common. More recently, single-stage procedures have become preferred in most centers, even for tumors with sizable intra- and extracranial components, as well as those involving multiple cranial fossae. Computerized imaging modalities provide localizing information that guides the surgeon around vital structures and helps to enable thorough tumor removal.
Approaches to Cranial Base Lesions
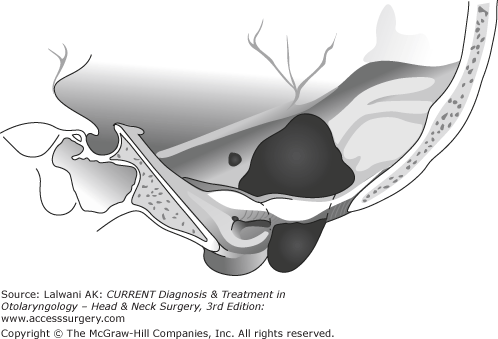
Temporal bone resection is a fairly radical operation conducted for malignant disease, particularly squamous cell carcinoma originating in the external auditory canal. Some other indications include adenomatous tumors, such as the aggressive papillary adenocarcinoma of the endolymphatic sac and those arising in salivary tissue (eg, adenocystic carcinoma). In most cases, the lateral portion of the temporal bone housing the ear canal is removed en bloc (Figure 66–1). The posterior margin consists of the dural lining of the petrous pyramid, which is exposed via mastoidectomy. The anterior margin often includes some or all of the parotid gland and, at times, the mandibular condyle and the temporomandibular joint (Figure 66–2).
Figure 66–1.

The degrees of temporal bone resection. The solid lines demarcate the so-called sleeve resection of the soft tissue of the canal. This is an insufficient approach to malignant tumors of the region. The dotted lines depict subtotal temporal bone resection. The dashed lines illustrate total temporal bone resection. (Reprinted with permission of Jackler RK.)
Most surgeons remove more deeply involved regions (eg, the cochlea, semicircular canal, and internal auditory canal) piecemeal, using a high-speed drill as resection en bloc risks injury to the internal carotid artery. In advanced lesions, the resection can be carried medially to the internal carotid artery, but its resection is seldom justified. After resection of the condyle, exenteration of the pterygoid muscles, including the third division of the trigeminal nerve to the level of the pterygoid plates, may be accomplished in deeply penetrating lesions. As a general rule, if the facial nerve works preoperatively, a diligent effort should be made to preserve it, although this is not always feasible and engraftment may be needed.
Reconstruction of the defect needs to anticipate the need for radiation therapy. Leaving an open cavity increases the risk of osteoradionecrosis. For this reason, the external auditory meatus is typically sewn shut. A rotation flap of temporalis muscle is often desirable to reinforce the closure with well-vascularized tissue. Regional (eg, pectoralis or trapezius) or even free (rectus abdominis) flaps may be needed for closure in cases where auriculectomy has been required.
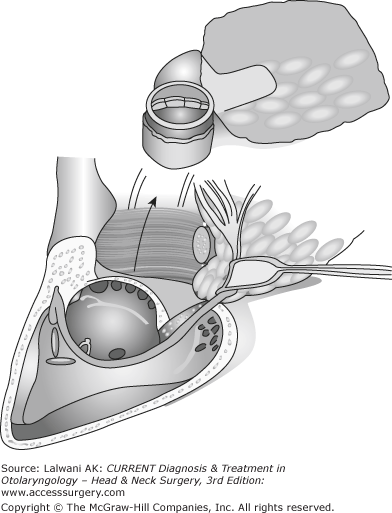
The majority of procedures conducted for disease in the petrous apex involve creation of a narrow drainage pathway that circumnavigates the inner ear. Such procedures, which are usually carried out to drain petrositis or cholesterol granulomas, are best-termed petrous apicotomy (Figure 66–3). In the subcochlear route, a channel is excavated along the floor of the external auditory canal and the hypotympanum, which traverses the narrow window between the cochlea, the carotid genu, and the dome of the jugular bulb.

An alternate pathway is the infralabyrinthine approach, conducted between the posterior semicircular canal and the jugular bulb, immediately behind the descending portion of the facial nerve. However, because most apical cysts are located anteriorly medial to the cochlea, the infralabyrinthine route is deeper, more difficult, and creates a less adequate drainage portal. Apical cysts which extend medial to the carotid artery can sometimes be marsupialized onto the nose via an endoscopic transsphenoidal approach.
Petrous apicectomy, the formal removal of the petrous apex, is conducted for neoplasms of the apex and petroclival junction. It is conducted via a low subtemporal craniotomy, which exposes the anterior face of the petrous pyramid (Figure 66–4). Anatomically, the resection is limited inferiorly by the horizontal portion of the internal carotid artery, laterally by the cochlea and internal auditory canal, and medially by Meckel cave and the trigeminal nerve. Exposing the infratemporal fossa beneath the internal carotid artery requires downfracture and subsequent repair of the zygomatic arch. The characteristic tumor of this region is the chondrosarcoma of the petroclival junction, which arises in the cartilaginous section of the foramen lacerum (Figure 66–5). Although it is not often necessary, apicectomy is sometimes used for the resection of cholesterol granulomas that have proven recalcitrant to drainage procedures.
Figure 66–4.
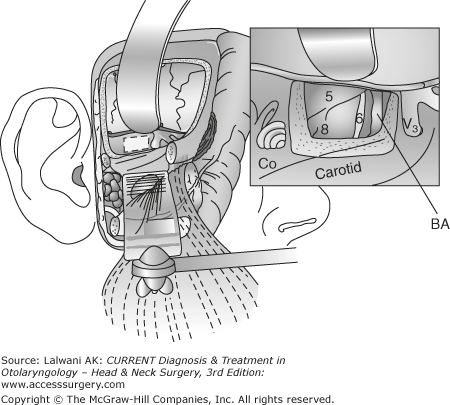
Petrous apicectomy is the surgical resection of the petrous apex and is carried out through a subtemporal exposure of the ventral surface of the petrous pyramid. Note the transapical view of the superior aspect of the cerebellopontine angle. Downward displacement of the zygomatic arch is optional. BA, basilar artery; Co, cochlear. (Reprinted with permission of Jackler RK.)
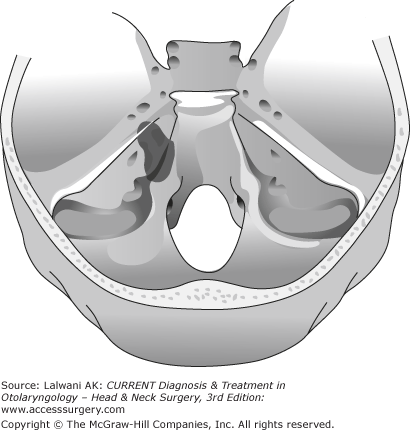
The clivus is not a bone in and of itself, but is rather a region composed of the dorsal part of the sphenoid bone and the portion of the occipital bone located anterior to the foramen magnum. The clivus, which, in Latin, means slope, spans from the posterior clinoid to the anterior margin of the foramen magnum. Adjacent to its dorsal surface is the entire brainstem and the vertebrobasilar system. The subject of clival tumors falls into two categories: (1) intrinsic tumors (especially chordomas) and (2) meningiomas arising from the dural lining of its dorsal surface.
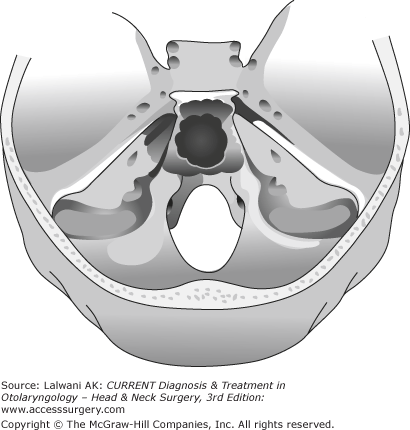
Chordomas arise from notochordal remnants in the midline of the skull base (Figure 66–6). Initially, they grow to fill the clival marrow compartment but later erode its cortical plate to spread intradurally. This brings them into contact with the brainstem, which may be compressed posteriorly. Intrinsic clival lesions, which remain extradural, are approached anteriorly via either a transsphenoethmoidal or transoral approach. The transsphenoethmoidal approach is well suited for lesions of the mid and upper clivus, whereas the transoral approach is preferred when lower clival and craniovertebral junction exposure is needed. Recently, endoscopic techniques are increasingly used in surgery of clival tumors.
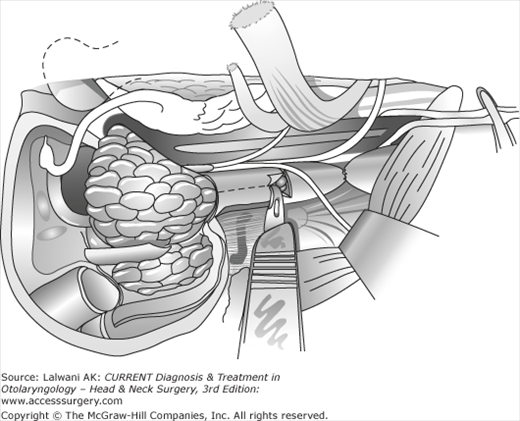
The jugular foramen is traversed by the jugular vein and the three lower cranial nerves (CN IX, the glossopharyngeal nerve; CN X, the vagus nerve; CN XI, the accessory nerve). The vertical segment of the facial nerve lies immediately lateral to the jugular foramen, presenting one of the classic challenges in cranial base surgery. The dome of the jugular bulb approaches the hypotympanic portion of the middle ear. Three tumor types predominate in tumors of this region: (1) glomus jugulare tumors, (2) meningiomas, and (3) lower cranial nerve schwannomas. These may remain confined to the cranial base, but most often possess a component in the upper neck, posterior cranial fossa, or both (Figure 66–7).
The jugular foramen approach begins control of the great vessels in the upper neck (Figure 66–8). Exposure of the foramen itself commences with a mastoidectomy and decompression of the bony covering of the sigmoid sinus. After skeletonization of the descending fallopian canal, the lateral aspect of the jugular foramen is exposed. Tumor resection commences after connecting the skull base and neck dissection followed by proximal and distal occlusion of the jugular vein (Figure 66–9).
Figure 66–8.
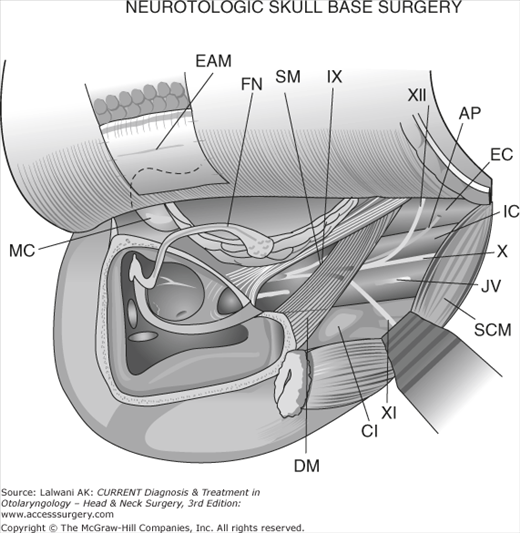
Surgical exposure of the jugular foramen region after mastoidectomy, anterior rerouting of the facial nerve, and upper-neck dissection. MC, mandibular condyle; EAM, closed external auditory meatus; FN, facial nerve; SM, styloid muscle; IX, glossopharyngeal nerve; DM, digastric muscle; C1, the transverse process of C1; XI, accessory nerve; XII, hypoglossal nerve; AP, ascending pharyngeal artery; EC, external carotid artery; IC, internal carotid artery; X, vagus nerve; JV, jugular vein; SCM, sternocleidomastoid muscle. (Reprinted with permission of Jackler RK.)
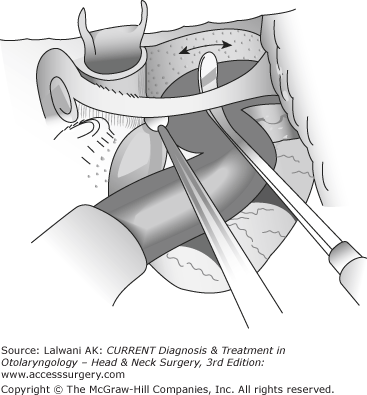
Traditionally, many surgeons rerouted the facial nerve anterior to obtain unobstructed access to the jugular foramen. However, this frequently leads to transient palsy, which does not always recover to normal. More recently, a fallopian bridge technique has gained popularity. In this procedure, the facial nerve remains in situ, and microdissection is carried out around it (Figure 66–10). Some surgeons use facial nerve rerouting selectively when encasement of the carotid artery necessitates obtaining augmented anterior exposure.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


