28
Neuronavigation in the Temporal Bone
Image guidance technology has found widespread use in otolaryngology since its inception in endoscopic sinus surgery. Although initially touted as a way of inviting inexperienced surgeons to initiate difficult surgery, image guided surgical navigation systems hold promise in facilitating safer surgery and resident education.1 By contrast, its role in otology and neurotology is still evolving. The primary concern lies with the level of precision that is required in temporal bone surgery to avoid substantial complications.
Image guidance technology facilitates intraoperative anatomical localization by employing high definition radiographic images, either computed tomography (CT) or magnetic resonance imaging (MRI), that are correlated to defined anatomical points on the patient. Thus points in contact with the surgical instrument on the patient can be correlated with their anatomical points on the radiograph, facilitating safer, more limited dissection. What results is a surgical field that is cylindrical in shape rather than the traditional funnel shape with open techniques. A smaller surgical field potentially should result, with a smaller wound, shorter recovery time, and increased margin of safety.
The temporal bone is theoretically ideal for image guidance technology for four reasons, according to Staecker et al: (1) the anatomy of the temporal bone and lateral skull base is fixed along bony landmarks minimizing shifts caused by intraoperative changes such as edema and cerebrospinal fluid (CSF) shifts, (2) the complexity of the anatomy within the temporal bone, (3) variability of the anatomy secondary to congenital or pathological conditions, and (4) the dependence of temporal bone surgery on anatomical landmarks and the extensive periods of dissection that are required to identify these landmarks.2 Despite this, image guidance technology has yet to be universally received by otologists and neurotologists.
This chapter discusses the image guidance technology that exists, the experiences reported, and the pitfalls of its use. Because the stereotactic systems utilizing a frame-based Cartesian coordinate system employed by our neurosurgical colleagues leave the temporal bone inaccessible, limiting its applicability in otology and neurotology, the discussion here focuses on frameless image guidance systems.
■ Overview
The current image guidance systems require, at base, a computer, a position sensor, and a digital image of the surgical field in question. Fig. 28–1A,B shows the LandmarX system (Medtronic USA Inc., Jacksonville, Florida). Image coordinates are correlated to the surgical field using three or more noncolinear points in common between two coordinate systems. This can be defined using fiducials. The fiducials may involve specific anatomical landmarks or reference markers applied to the head at consistent, immovable sites. These markers must be in place at the time that the radiographic image is obtained. For otologic and neurotologic uses, a Mayfield head holder or a skull post may hold reference markers similar to a sinus head holder used in endoscopic sinus surgery.
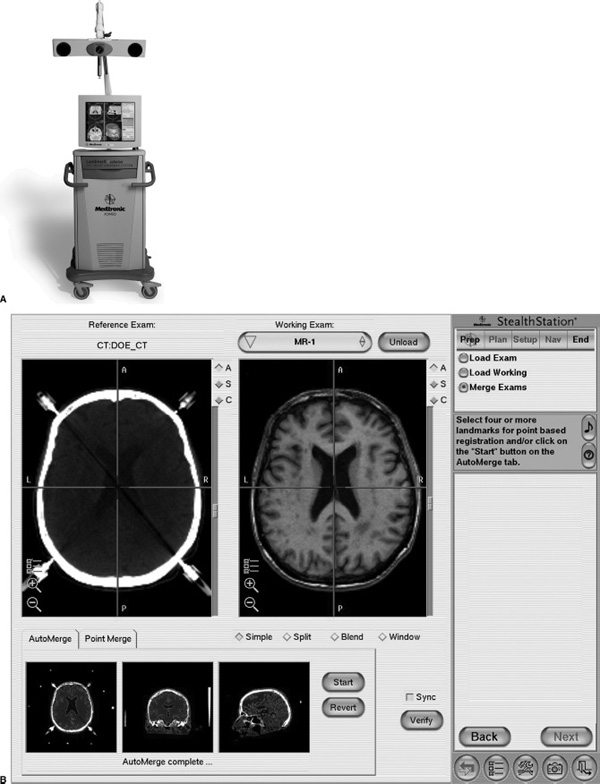
FIGURE 28-1 (A) The LandmarX system consists of the infrared signal emitter, the monitor, and a computer. (B) The computer interface with the magnetic resonance image (MRI) is seen with localization of the instrument to the anatomical site relative to the MRI image. (Courtesy of Medtronic USA Inc., Jacksonville, Florida.)
Prior to use in surgery, the specific reference points on the patient must be correlated to the radiographic image previously obtained. Precise calibration is necessary to optimize the system’s accuracy. Calibration requires that positional data from a wand or a surgical instrument be transferred from the positional sensor on the wand or instrument to the computer utilizing either a mechanically linked system or a nonmechanically linked system. Calibration should result in an error that is less than 1 mm for temporal bone surgery. Once calibration is completed, the surgeon is able to apply the positional sensor within the surgical field and correlate its position to the previously obtained radiographic image. The neuronavigation systems currently available are presented and their characteristics compared in Table 28–1
■ Mechanically Linked Systems
Mechanically linked systems are based on articulated arms that are mounted on the operating table.3–5 After calibration, the angle detectors and sensitive potentiometers at the articulated points relay positional information to the computer providing real time anatomical data. Secondary to the bulk of the instrumentation, versatility is lacking. Therefore, there has been limited use within otology and neurotology.
■ Nonmechanically Linked Systems
Nonmechanically linked sensor systems have found most acceptance. These systems rely on the detection of signals transmitted by emitters that are most often coupled to a surgical instrument or a suction. Using triangulation concepts utilized by satellite systems, the precise location of the instrument is tracked and coupled to the properly referenced radiographic image. The systems vary according to the mode of signal transmission.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


