Neuro-Ophthalmologic Examination—Efferent System
Disorders of the efferent visual system result in either ocular misalignment or abnormalities in ocular motility without ocular misalignment. The most frequent symptom that prompts a neuro-ophthalmologic examination of the efferent system is diplopia. other symptoms such as head tilts, face turns, etc., also require that evaluation of the efferent system be performed looking for disorders of ocular motility even when the patient does not appreciate double vision.
The patient who presents with the symptom of diplopia should be approached in a systematic way to most efficiently identify the cause of diplopia and whether the diplopia has a potentially neuro-ophthalmic cause. There are several steps to follow to arrive at the correct diagnosis.
IDENTIFY MONOCULAR DIPLOPIA
The most important initial aspect of the diplopia evaluation is for the examiner to understand if the double vision is present only with both eyes open or is appreciated monocularly. Monocular diplopia is almost invariably due to an ocular disorder and is very rarely a manifestation of neuroophthalmologic disease. Patients with monocular diplopia therefore need not be subjected to intensive neurologic and neuroradiologic investigations. If the patient has not cross-covered his eyes and does not know if the double vision persists when either eye is occluded, that is the first maneuver the examiner should perform. If the patient perceives double vision with one eye occluded, this is monocular diplopia. Monocular diplopia is most often produced by an ocular disorder that will disrupt the incoming parallel rays of light, preventing them from coming to a point focus on the retina. Instead, a blur circle is formed on the retina and a ghost image that is often described as diplopia results. The most frequent causes of monocular diplopia are as follows:
• Refractive error, especially astigmatism
• Cataract, usually of the nuclear sclerotic variety
• Corneal scarring
• Iris abnormalities, such as atrophy or generous peripheral iridotomies
• Subluxated lens or implant
• Nonphysiologic causes
The easiest way to document that monocular diplopia is due to a refractive or an anterior segment problem is to use the pinhole. An occluder with multiple pinhole openings from 2 to 2.5 mm each is placed in front of the patient’s symptomatic eye (Fig. 9-1A,B). The patient is then asked if the monocular diplopia is improved or has disappeared. An affirmative answer establishes the anterior segment or a refractive error as the cause of the problem.
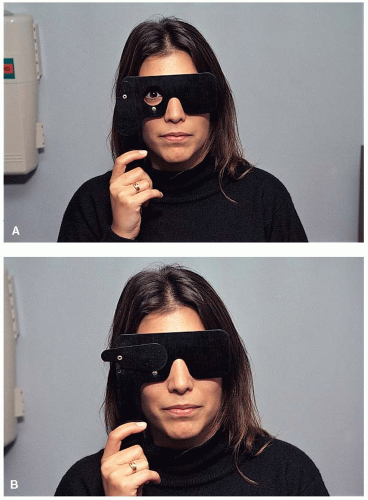 Figure 9-1. Patient complains of diplopia in the right eye (A) that disappears when the pinhole occluder is placed before the eye (B). |
DETERMINE WHETHER MISALIGNMENT IS COMITANT OR INCOMITANT
If the patient indicates that diplopia is present only with both eyes open, the patient has true binocular diplopia. This symptom is almost always due to ocular misalignment. The purpose of this step and the next several steps is to identify the pattern of the misalignment to see if it corresponds to isolated or combined cranial nerve (CN) palsies.
A comitant strabismus is one in which the amount of deviation is the same in all directions of gaze and irrespective of which eye is fixating. A strabismus is incomitant when the angle of deviation varies with the direction of gaze or depending on which eye is fixating. Comitant ocular misalignments are usually decompensated congenital deviations. Incomitant misalignments are usually acquired disorders and caused by paralytic or mechanical processes. Certain congenital decompensated phorias, for example, congenital CN IV palsies, may produce incomitant misalignments. The presence of a comitant deviation, particularly when ocular ductions and versions are full (page 223), usually indicates a nonneurological cause for the diplopia.
There are several ways to measure the pattern of the ocular misalignment.
Prism Cover Test
By introducing prism in front of one eye and utilizing a cover/uncover or alternate cover test, the amount of ocular misalignment is measured in prism diopters (PD). All measurements should be performed in at least six directions of gaze: primary position, right, left, up and down gaze, and at near. oblique gaze and measurements on head tilt are employed under special circumstances. The measurement is then recorded on a chart, which
signifies these directions of gaze (Fig. 9-2). In the appropriate clinical setting, the ocular misalignment is measured on right and left head tilt. This is usually used when either a CN IV palsy or an ocular tilt reaction is suspected. The patient is seated in the upright position; the head is tilted to the right and then to the left, and the vertical misalignment is measured in the right and left head tilt positions. In CN IV palsies, the vertical misalignment will be greater when the head is tilted toward the side of the palsy.
The primary deviation refers to the amount of ocular misalignment measured when the patient is fixating with the nonparetic eye. The secondary deviation is the measured angle of deviation when the patient is fixating with the paretic eye. Patients with nonparalytic strabismus do not measure a difference between the primary and secondary deviations; the ocular misalignment is the same when they fix with either eye. The patient with a paralytic strabismus, however, will have a much larger ocular misalignment when the paretic eye is fixing (secondary deviation) and less of a misalignment when the nonparetic eye is fixing (primary deviation) (Fig. 9-3). In patients with paralytic strabismus the secondary deviation is always greater than the primary deviation. This is due to Hering’s law of equal innervation to yoke muscles because an increase in innervations is needed when the paralytic eye is fixating. Consequently, the contralateral yoke muscle also receives more innervations resulting in a larger deviation.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


