Neuro-ophthalmic Aspects of Orbital Disease
Manoj M. Thakker
James C. Orcutt
The orbit is a unique structure, a bony cave of approximately 1-fluid ounce volume, opened widely at the entrance and tapering to an opening smaller than a pencil at the apex. Through this space runs the most complex nerve of the body, the optic nerve, which contains more than a million individual nerve fibers. More than half our sensory knowledge about our environment travels to the brain through the 2 optic nerves. In addition, there are 10 other nerves, 4 major blood vessels, and the origins of 5 muscles surrounding the optic nerve at the orbital apex—all in a space no larger than a dime. It is not surprising that examination of these nerves, vessels, and muscles can help the ophthalmologist exquisitely localize an orbital disease process.
The techniques of neuro-ophthalmic examination and orbital examination are both discussed elsewhere in Volume 2. The readers of this chapter should acquire an appreciation of the usefulness of neuro-ophthalmic examination techniques applied to orbital diagnosis. This chapter is divided into three sections: the afferent system—vision and sensation; the efferent system—eye movement, autonomic nerves and facial innervation; and examples of clinical cases demonstrating the applications of the neuro-ophthalmic examination to orbital diagnosis. Anatomy remains the bridge between examination and diagnosis and so is reviewed with each section. Additional anatomic detail is available elsewhere in these volumes as well as in other texts.1,2,3
THE AFFERENT SYSTEM
ANATOMY
Orbit
The orbital apex has two major openings, the orbital fissure and the optic canal (Fig. 1). The orbital fissure is divided into a superior and inferior portion by the tendon of Zinn, the inferior insertion for the tendinous anulus of Zinn (Fig. 2).1,4 (The anulus of Zinn is completed by the origins of the rectus muscles and the superior tendon of Lockwood.) Structures emanating through the optic canal (the optic nerve, ophthalmic artery, and orbital sympathetic nerves) as well as some structures coursing through the superior orbital fissure (the superior and inferior branches of the oculomotor nerve (cranial nerve III), the abducens nerve (cranial nerve VI) and the nasociliary branch of the ophthalmic division (cranial nerve V1) of the trigeminal nerve pass through the anulus of Zinn.
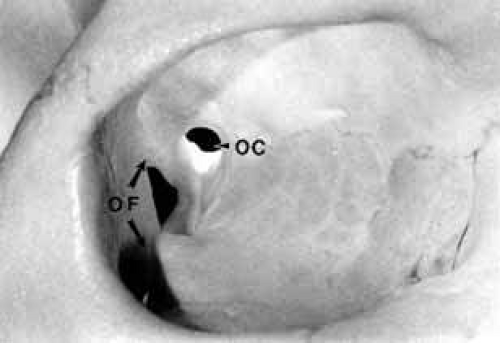 Fig. 1 Two openings are present at the orbital apex: the orbital fissure (OF) and the optic canal (OC). |
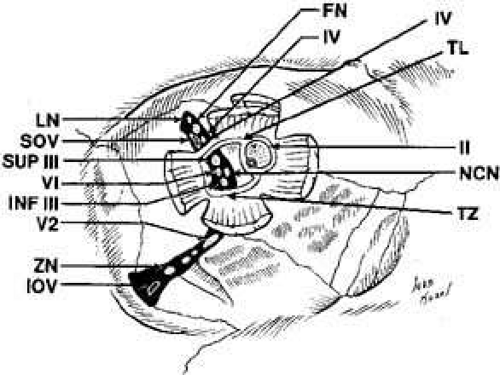 Fig. 2 Structures at the orbital apex. The anulus of Zinn is composed of the tendon of Zinn (TZ), tendon of Lockwood (TL), and the insertions of the rectus muscles. Structures exiting the superior orbital fissure outside the anulus of Zinn include the lacrimal nerve (LN), superior ophthalmic vein (SOV), the frontal nerve (FN), the trochlear nerve (IV). and the anastomotic branch between the middle meningeal artery and lacrimal artery (not shown). Structures passing through the anulus of Zinn include the superior (SUP III) and the inferior (INF III) branch of the oculomotor nerve, the nasociliary nerve (NCN), the abducens (VI), and the optic nerve (II) with its associated ophthalmic artery and sympathetic nerves. Structures exiting through the inferior orbital fissure include the infraorbital nerve (V2), the inferior ophthalmic vein (IOV), and the zygomatic branch of the infraorbital nerve (ZN). (Courtesy of Deborah D. Sherman, MD, Nashville, TN) |
The orbital vascular supply is provided primarily by the ophthalmic artery (Fig. 3), and its branches, the central retinal artery, muscular branches, posterior ciliary arteries, posterior and anterior ethmoidal arteries, and the lacrimal artery. Venous drainage of the orbit is primarily by the superior ophthalmic vein into either the cavernous sinus or the pterygoid plexus (Fig. 4). A variable but generally lesser amount of venous outflow leaves through the inferior orbital vein into the pterygoid plexus. Numerous anastomoses are generally present between the superior and inferior ophthalmic veins.
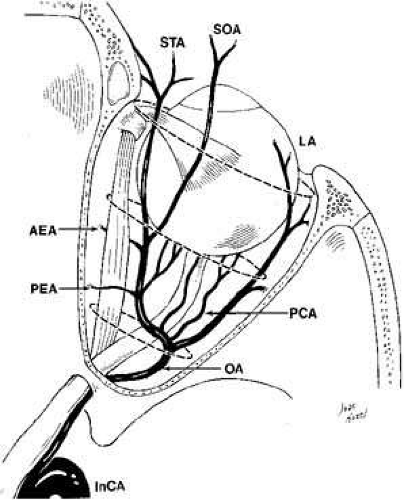 Fig. 3 Orbital arterial supply derives from the internal carotid artery (InCA) by the first major intracranial branch, the ophthalmic artery (OA). The OA branches into the central retinal artery, muscular branches, posterior ciliary artery (PCA), posterior ethmoidal artery (PEA), anterior ethmoidal artery (AEA), and the lacrimal artery (LA) eventually terminating as the supratrochlear artery (STA) and supraorbital artery (SOA). (Courtesy of Deborah D. Sherman. MD, Nashville, TN) |
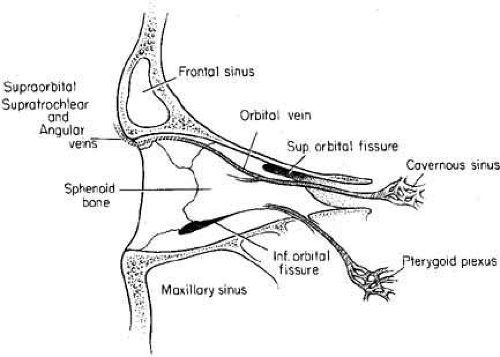 Fig. 4 Orbital venous drainage occurs primarily by the superior ophthalmic vein (SOV) through the superior orbital fissure into the cavernous sinus, A lesser venous drainage occurs by the inferior orbital vein (IOV) through the inferior orbital fissure into the pterygoid plexus. Numerous anastomoses are common between these veins. |
Cranial Nerve II (Optic Nerve)
The optic nerve is contained within a dural sheath, which is continuous at the orbital apex with the periosteum of the optic canal. Intracranially the periosteum is continuous with the dura, thus providing access of cerebrospinal fluid to the sub-arachnoid space surrounding the optic nerve (Fig. 5). Elevated cerebrospinal fluid pressure, meningeal inflammation, or air from pneumocephalus can extend into the orbit within the optic sheath (Fig. 6).5
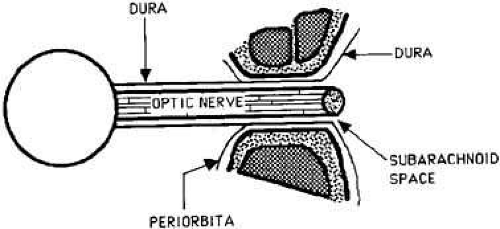 Fig. 5 Longitudinal section of the optic nerve through the optic canal. The intracranial subarachnoid space is continuous with the subarachnoid space surrounding the optic nerve. The subarachnoid space extends anteriorly to the level of the lamina cribrosa. |
 Fig. 6 T2-weighted magnetic resonance imaging (MRI) shows cerebrospinal fluid (CSF) surrounding the optic nerve within the subarachnoid space (arrow). The CSF extends to the posterior pole of the globe. An optic nerve meningioma is present on the contralateral side. |
The optic nerve remains vulnerable to compression within the bony confines of the orbit. Compressive optic neuropathy is most likely to occur where the optic nerve is tethered to the bone, that is, at the orbital apex (Fig. 7A). The optic nerve in other areas of the orbit can be displaced markedly without suffering vision loss (Fig. 7B).
 Fig. 7 A. A cavernous hemangioma measuring 1.5 cm in longest dimension is located at the orbital apex displacing the optic nerve (arrow). Visual acuity is 20/40. there is a relative afferent pupil defect, and visual field shows a central scotoma. B. A cavernous hemangioma measuring 2 cm in longest dimension is located in the midorbit displacing the optic nerve (arrow). Visual acuity is 20/20. There is no relative afferent pupil defect and the visual field is normal. |
Cranial Nerve V (Trigeminal Nerve)
The ophthalmic branch of the trigeminal sensory nerve (cranial nerve V1) arises in the trigeminal ganglion, travels forward within the infralateral wall of the cavernoussinus and divides into its three major branches, the nasociliary, lacrimal, and frontal branches (Fig. 8).
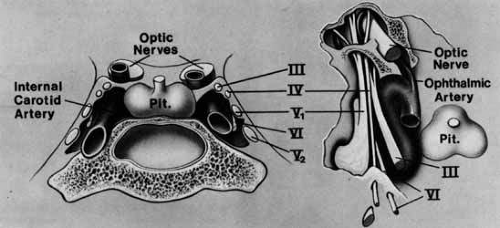 Fig. 8 Anatomy of motor and sensory nerves within the cavernous sinus. |
The lacrimal and frontal nerves pass above the anulus of Zinn along with the trochlear nerve (cranial nerve IV), the superior ophthalmic vein, and the anastomotic branch of the middle meningeal artery to the lacrimal artery. The frontal branch of cranial nerve V1, provides sensory input from the upper eyelid and forehead, while the lacrimal branch receives its input from the lacrimal gland and the superior temporal eyelid. The lacrimal branch is unique because its terminal branches carry the efferent parasympathetic fibers for lacrimal gland secretion, received from the zygomaticotemporal nerve near the lateral orbital wall.
The nasociliary branch of cranial nerve V1 gives off branches to the globe (long and short posterior ciliary nerves) before terminating as the infratrochlear nerve that provides sensory innervation to the superior medial eyelid. A small, external nasal branch is also given off with the anterior ethmoidal artery that extends under the nasal mucosa to innervate the tip of the nose.
The infraorbital fissure transmits the infraorbital nerve, a branch of the maxillary division (cranial nerve V2) of the trigeminal nerve (see Fig. 2). Branches of the infraorbital nerve rise in the lateral orbit, providing sensation to the temple (zygomaticotemporal nerve) and the lateral malar area (zygomaticofacial nerve) (Fig. 9). The infraorbital nerve continues anteriorly within a bony tunnel until it appears through the maxillary bone to innervate the ipsilateral face to the midline from the lower eyelid to the upper lip. Prior to innervating the face, the infraorbital nerve sends three major descending branches to the upper teeth. The most proximal branch is given off prior to entering the infraorbital fissure (superior posterior alveolar nerve) and innervates the upper molars; the next two branches (middle superior, and anterior superior alveolar nerves) are given off within the infraorbital fissure and canal. These nerves innervate the remainder of the ipsilateral teeth to the midline (Fig. 10). The infraorbital fissure also transmits the inferior orbital vein that drains the inferior orbit into the pterygoid plexus (see Fig. 4).
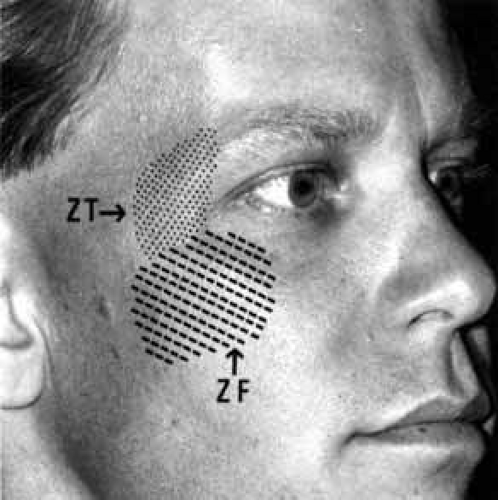 Fig. 9 Peripheral distribution of the zygomaticotemporal (ZT) and zygomaticofacial (ZF) nerves. |
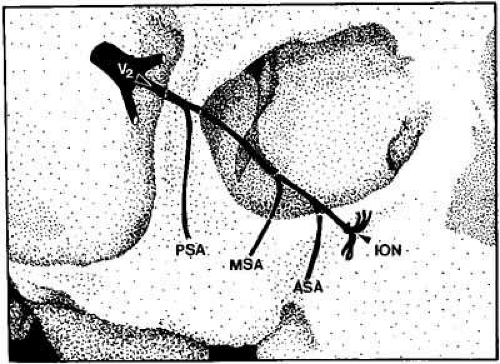 Fig. 10 The infraorbital nerve (ION) is the major branch of the maxillary division (V2) of the trigeminal nerve. Three branches to the upper teeth originate prior to facial innervation. The posterior superior alveolar nerve (PSA) decussates from the infraorbital nerve prior to entering the infraorbital fissure or canal, while the middle superior alveolar nerve (MSA) and the anterior superior alveolar nerve (ASA) decussate within the orbital portion of the infraorbital nerve. |
OPTIC NERVE
The tempo and character of vision loss can be important diagnostically. The tempo of visual acuity deterioration varies from optic nerve tumors with characteristically chronic and progressive loss to that of cellulitis or idiopathic orbital inflammation which may be apoplectic. Characteristics of visual change are also important; for instance, gaze-evoked vision loss is most commonly associated with intraconal tumors such as [MT1]optic nerve meningiomas or cavernous hemangiomas.6 This symptom may also occur in patients with orbital fractures, intraconal foreign bodies, or extraconal tumors that compress the central retinal artery.7,8 Transient obscurations of vision, a fleeting blurring of vision lasting seconds, may be associated with papilledema.9 This symptom can be differentiated from amaurosis fugax (complete loss of vision of moderate duration), which is more likely to be secondary to embolic occlusion of the ophthalmic or central retinal artery.10
Every patient with a suspected orbital abnormality deserves a complete eye examination, whether he or she needs it or not.11 Visual acuity with current correction, a manifest refraction, and a cycloplegic refraction are important to detect induced hyperopia from an intraconal tumor. A rough approximation is 3 D of induced hyperopia for each millimeter of globe shortening. Evaluation of afferent visual function should include tests of color vision, relative afferent pupillary defect, and visual field.
Ophthalmoscopy can be very helpful in orbital diagnosis. Optic disc edema may be caused either by papilledema (increased intracranial pressure) (Fig. 11A), papillitis (anterior optic neuritis) (Fig. 11B), or vasculitis (e.g., lupus erythematosus, sarcoidosis, Wegener’s granulomatosis, and giant cell arteritis) (Fig. 11C).12 Papilledema (Fig. 11A) is usually present with near-normal visual function, although some patients may lose vision.9 In contrast, papillitis (Fig. 11B) characteristically leads to reduced visual function, commonly is associated with orbital pain, and is associated with inflammatory cells in the vitreous overlying the disc. Optic disc vasculitis (Fig. 11C) may be present with other findings of vasculitis, and commonly is associated with poor acuity and evidence of vascular occlusion (e.g., cotton-wool spots, hemorrhages). The differential diagnosis of the swollen, erythematous disc is discussed elsewhere in these volumes.
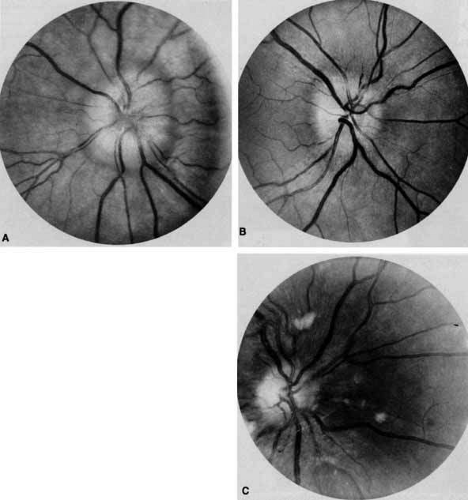 Fig. 11 A. Papilledema caused by pseudotumor cerebri. Visual acuity is 20/15 and the visual field is normal. B. Papillitis of anterior optic neuritis. Visual acuity is 20/400 with a relative afferent pupillary defect and a central scotoma. C. Vasculitis of optic disc caused by lupus erythematosus. Visual acuity is 20/200, there is a relative afferent pupillary defect, and a cecocentral scotoma. Note cotton-wool spots. |
Optociliary shunts (Fig. 12A) develop as a result of long-term obstruction of the central retinal vein. This may occur secondary to optic nerve meningiomas,13 optic nerve gliomas,14,15 optic nerve meningoceles,16 central retinal vein occlusions,17 optic nerve sarcoidosis,18 craniosynostosis,19 optic nerve arachnoid cysts,20 optic disc drusen,21 and papilledema.15 Congenital optociliary shunts, which are exceedingly rare, have not been associated with optic neuropathy or orbital disease.22,23 The presence of optic nerve pallor, poor acuity and optociliary shunts generally implies an optic nerve meningioma in the absence of other funduscopic findings (Fig. 12B).13
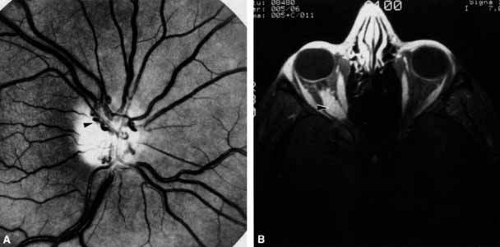 Fig. 12 A. Optociliary shunt vessels (arrow) are present on the surface of an atrophic optic disc. The patient’s visual acuity was hand motions. The patient demonstrates 2 mm of proptosis. B. Gadolinium-enhanced, fat-suppressed magnetic resonance imaging (MRI) demonstrates an intraorbital optic nerve sheath meningioma (arrow). |
Visual field testing can also be helpful in diagnosis of orbital processes. Optic disc–associated visual field changes are usually altitudinal because of the structure of the horizontal raphé (Fig. 13). This visual field defect is typically a result of anterior ischemic optic neuropathy (AION).24 Compressive lesions of the orbit or retrobulbar inflammation are more likely to produce a central or cecocentral scotoma. However, one must be aware that there is a significant degree of overlap between various types of optic nerve lesions and visual field abnormalities.25 In these cases, neuroimaging may be a useful adjunct in differentiating between different neuro-ophthalmic and orbital processes.26
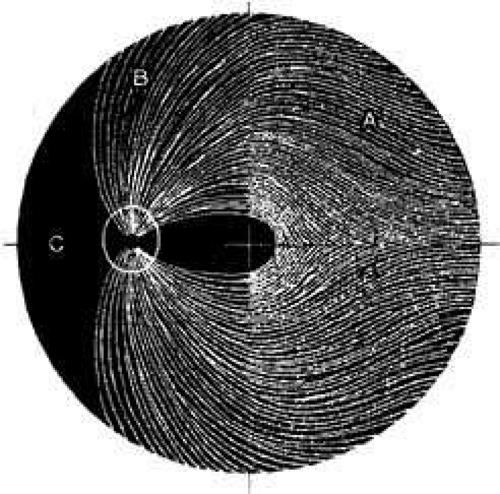 Fig. 13 Pathway of ganglion cell axons that originate temporal to the macula (A) do not cross the horizontal meridian. Any damage to the superior ganglion cell axons at the optic disc will generate atrophy within the superior nerve fiber layer (B). The visual field defect will be inferior but not crossing the horizontal plane. (Hoyt WF, Rios-Montenegro EN, Behrens MM, et al: Homonymous hemioptic hypoplasia: funduscopic features in standard and red-free illumination in three patients with congenital hemiplegia. Br J Ophthamol 56:537, 1972) |
The relationship of visual function to orbital findings often helps in the differential diagnosis. For instance, patients with cavernous hemangiomas may have significant proptosis but retain normal, best-corrected visual function (see Fig. 7B), but patients with intrinsic optic nerve meningiomas may demonstrate minimal proptosis with significant vision loss (see Fig. 12B).
Trigeminal Sensation
Historically, the progression of numbness may be helpful in diagnosis of orbital disease. For instance, adenoid cystic carcinoma of the lacrimal gland27,28 and some melanomas29 have a predilection for perineural invasion. The presence of a lacrimal gland mass, which is followed by numbness in the distribution of the lacrimal (see Fig. 2), zy-gomaticotemporal, or zygomaticofacial nerves (Fig. 9), can indicate perineural extension of an adenoid cystic carcinoma.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


