15b

Nd:YAG Laser and the Treatment
of Nasal and Sinus Pathology
This chapter presents an innovative concept for the management of nasal sinus disorders: the coupling of a flexible fiberoptic endoscope with the neodymium: yttrium-aluminum-garnet (Nd:YAG) laser. This provides a video image of the interior of the nose and sinuses and delivers laser energy to manage many different types of pathology. This chapter describes the equipment, technique, and results accumulated over the author’s many years of experience.
In 1914, Albert Einstein1 discovered the principle of light amplification by stimulated emission of radiation: the laser. With the Nd:YAG laser, the emission originates from the active center, the neodymium crystal, which is a garnet crystal, composed of yttrium and aluminum. The krypton lamp power can reach 100 watts, allowing for crystal stimulation. The Nd:YAG laser emits energy at 1060 nm, which is about the speed of infrared light. This wavelength allows the emission to be transported intact by fiberoptics without damaging the fiber. It is an excellent laser for flexible fiberoptic intranasal surgery and has been used since 1987 by the author to treat benign lesions of the nasopharynx of adults and adolescents.
In popular culture, laser is associated with mythical futuristic significance and endowed with extraordinary powers. In medicine, however, it remains a surgical tool and nothing else. Its applications are now precisely defined. The otolaryngologist using the laser needs to have specific training and in-depth clinical experience as with any surgical technique.
 Biophysical Notions: Nd:YAG Laser and Tissue
Biophysical Notions: Nd:YAG Laser and Tissue
The laser’s applications in medicine are based on the conversion of light energy into heat in the irradiated tissue. The extent and the degree of the thermal effect depend on beam geometry and the energy of incident light, as well as the optical and thermal tissue properties. The laser beam is emitted in visible light such as argon and dye lasers or in invisible light such as Nd:YAG or CO2 laser.
The Nd:YAG Laser Beam Differentiated from the CO2 Laser Beam
The differences between the Nd:YAG and CO2 laser determine the condition in which the laser is used. The CO2 laser emits light at 10,600 nm, penetrating the tissue surface and its depths. All tissues absorb it. It is used essentially as a scalpel, but it can vaporize and coagulate tissue.
The Nd:YAG laser emits light at 1060 nm and is moderately absorbed by water, glass, and plastic. It can be transported by a quartz fiber without being changed. The proteins of all opaque tissues absorb it. The more pigmented the tissues, the more absorbed the light is. For this reason, the superficial cell layers do not absorb the beam, as is the case with the CO2 laser. The energy absorbed becomes effective at a depth of 2 or 3 nm. At this particular depth, Nd:YAG distributes its heat uniformly. The heat makes a pear-shaped coagulation effect that extends to a depth of 2 to 6 mm, as a function of the power irradiation time and tissue properties. This deep pear-shaped thermal effect causes very little damage to the surface. This is confirmed by electronic microscopic examination that reveals good preservation of the surface tissue. A thin fibrin sheet covers the surface tissue after the Nd:YAG irradiation, without any contact between the fiber and the mucosa.
Interaction between Nd:YAG Laser and Tissue
In 1979, Frank and colleagues2 showed that the Nd:YAG laser irradiation of the bladder wall, with 40 W of power, created several different findings in the tissue.
In the superficial layers, there is a zone of edema. In the deeper layers, there are protein drops or clusters deposited in cellular interstices and on sections of smooth muscles. On the deeper layers, there is necrosis of 2 to 4 mm, without elevation of the surface temperature above 100°C. This is observed only on histological sections. Even deeper, there is heat distribution in the bladder wall that never reaches the critical temperature of 58°C on the external bladder wall.
These observations have been seen in animals and humans with the help of thermocameras and thermometric probes during laser irradiation. These methods give valuable information with the following histological conclusions.
1. There is coagulation and destruction of lesions without any significant alteration of surface tissues.
2. The mechanical stability of the irradiated wall is preserved.
3. Several laser-irradiated sessions at 40 W by the Nd:YAG laser during a period of 2 seconds did not produce any intestinal perforation.
In 1979, Halldorson showed that the interaction between the Nd:YAG laser and tissue could be easily controlled. The risks are far less than with the CO2 or the argon laser all the more before the exposure of tissue to the CO2 laser at 0.5 W over 4 seconds produces a thermal elevation equivalent to that provoked by 40 W with the Nd:YAG, which is even slower.
In general, the Nd:YAG laser beam can be transmitted by a quartz fiber without being absorbed until the energy reaches the tissue. Only there does energy emission take place. The Nd: YAG laser is a defocused beam that produces a pear-shaped shot similar to an explosive bullet, producing a deep tissue disintegration and a retraction by a cicatricial phenomenon.
These experiments were conducted at the same time by other researchers, notably Buiter3 in Groningen, Germany, who used the Nd:YAG laser with various rigid tubes. At the end of the 1970s, he used rigid fiberoptics or surgical microscopes under general anesthesia to ensure palliative treatment of head and neck cancers, to vaporize and destroy mucosa, to manage choanal atresia, and to coagulate the epistaxis caused by hereditary hemorrhagic telangiectasia (Rendu-Osler-Weber syndrome).
 Advantages of the Nd:YAG Laser as Compared with the CO2 Laser
Advantages of the Nd:YAG Laser as Compared with the CO2 Laser
The Nd:YAG laser is relatively easy to use after appropriate training and after the operator gains experience.
Because of the flexible fibers through which the Nd:YAG laser energy is passed, there is better accessibility to various lesions in the nasal cavity, paranasal sinuses, and nasopharynx. An eye safety filter prevents any eye injury that may occur by transmission of energy from the operative site. Surgical precision is in the order of tenths of a millimeter. In addition, the deep retractile scarring is definitive and consistent. This is not always the case with the CO2 laser, which has more surface action.
The Nd:YAG laser has a superior hemostatic and sterilizing effect resulting from the thermal energy compared with the CO2 laser.
The postoperative effects are practically nonexistent: There is minimal postoperative edema. Postoperative infections rarely occur. Therefore, there is little justification for the use of systematic antibiotics. Postoperative hemorrhage also rarely occurs.
 Preoperative Preparation
Preoperative Preparation
A meticulous history is obtained to clarify patients’ complaints and to be certain they are candidates for fiberoptic office laser management. Care is taken to look for the etiology of continuous or intermittent nasal obstruction that is position dependent or the presence of anterior or posterior nasal drainage and its character (serous or purulent). It is important to understand what type of previous medical or surgical treatment had been tried. Any surgical contraindications are evaluated.
A complete ear, nose, and throat examination is performed, including nasal endoscopy that gives precise details on anatomical abnormalities and pathology within the nasal cavity and sinus recesses. Appropriate laboratory examinations may be necessary to determine if there is any allergy infection present.
Rhinomanometry is occasionally used. It measures the degree and location of obstruction. The airflow of each nasal fossa before and after vasoconstriction is measured to help determine the degree of turbinate involvement in the nasal obstruction.
 Therapeutic Indications of the Nd:YAG Laser
Therapeutic Indications of the Nd:YAG Laser
There are several different indications for the use of the fiberoptic laser in the management of nasal and sinus pathology. In the nasal cavity, this includes hypertrophic rhinitis that can be caused by allergic rhinitis, vasomotor rhinitis, postoperative compensation after septoplasty or rhinoplasty, nasal fracture, endoscopic sinus surgery, nasal polyposis, membranous choanal atresia, synechiae, and recurrent epistaxis (e.g., hereditary hemorrhagic telangiectasia, superficial vessels in Kiesselbach’s area, and pyogenic granuloma). In rhinopharynx pathology, adenoid residues, cicatricial adhesions, inflammation, and nasopharynx cysts can benefit from fibroscopic therapy. The same is true for edema, cyst, or nodulus on the posterior pad of the eustachian tube.
 Equipment
Equipment
Therapeutic fiberoptic Nd:YAG laser therapy employs a flexible fiber and flexible endoscope with an internal operating channel (Fig. 15b–1). Imaging is either through the endoscope or from an attached camera and video monitor, depending on the comfort of the operator.
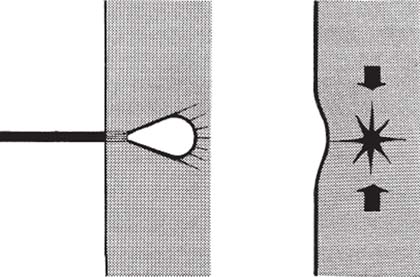
FIGURE 15b–1 YAG effect. The energy absorbed becomes effective at a depth of 2 or 3 mm. The absorption draws a pear-type coagulation to a depth of 2 to 6 mm, then a retraction by a cicatricial phenomenon.
The Nd:YAG Laser
Although the Nd:YAG laser has maximum power ranging from 40 to 100 W, depending on the model, the customary power in otolaryngology is generally less 30 W. Because the Nd:YAG laser beam is invisible, a helium neon-aiming beam is available on the system. This second red coaxial ray permits accurate aiming of the Nd:YAG beam.
There are several Nd:YAG models available for surgical use. The 100 W model is the oldest and needs cooling by water under high pressure. The slightest fall in water pressure will set off the automatic security blocking system, preventing its use. This model is found in many surgery centers where colleagues from other specialties require higher power and may have been using the system for many years.
The 40 to 60 W model is a more recent addition to surgical armamentarium. It is air cooled, has sufficient power for otolaryngology, is generally simple to operate, and is easily movable. Its small size and lower price make it a popular laser.
The Fiber
The Nd:YAG fiber is typically a bare quartz fiber and is 3 m long. The fiber has a thin Teflon sheath, giving it more strength. The fiber diameter is either 400 or 600 micron, depending on the size of the endoscopic operating channel. Most of the time, the 600-micron fiber is chosen because it is less brittle and enables more powerful delivery of laser energy. However, being less flexible, it is more difficult to handle.
When introducing the bare quartz fiber into the operating channel of the endoscope, care must be taken to avoid damage to the inner channel liner. The Teflon sheath, which increases the diameter of the fiber, helps to prevent such injury. This protective sheath is a flexible tube inserted into the operating channel of the endoscope to protect it. The bare quartz fiber slides into the sheath. It can be reused and changed at very little cost.
The Endoscope
A flexible fiberoptic endoscope is used, and viewing is done either through the scope itself or from a small monitor. The flexibility of the endoscope facilitates nontraumatic access to lesions that otherwise would be difficult to approach with a rigid endoscope or nasal speculum.
Several different endoscopes have been used. A 3.6 mm diameter endoscope with a 1.1 mm operating channel delivers an inadequate picture on the monitor, and the choice of fibers available is insufficient. A 4.1 mm diameter endoscope with an operating channel of 1.1 mm gives a better image, but the operating channel permits only 400-micron bare fibers. This fiber can only deliver the necessary power for treatment with energy so high that there is retrograde heat production, which can damage the endoscope. A 4.8 mm diameter endoscope equipped with an operating channel of 2 mm is most often used. This allows the passage of a 600-micron bare fiber.
Of course, the best fiberoptic endoscope is one that gives the best image, has the smallest external diameter, and offers the most precise handling. From year to year, the fiberoptic endoscope forges a better image quality thanks to the scope’s fiberoptic amelioration and smaller diameter, which enable greater image definition.
The Light Source
Although a 250 W light source can be used with the fiberoptic endoscope, a xenon light source is much better.
Imaging
A video camera is fitted onto the endoscope, and a video screen and a video recorder are used for observation and documentation.
 Considerations
Considerations
For the Patient
Laser nasal and sinus surgery is nearly always an ambulatory procedure. Occasionally a light sedative may be necessary.
For the Surgeon
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


