Fig. 2.1
(a) Young female with proptosis and bilateral upper lid retraction and lacrimal gland prolapse. (b) Axial computerized tomography (CT) scan of same patient showing marked proptosis from fat expansion but minimal muscle enlargement. Lacrimal glands are displaced beyond lateral rim
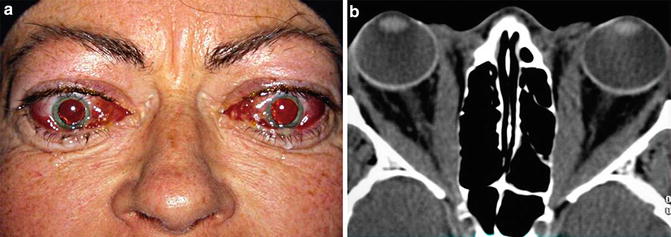
Fig. 2.2
(a) Older woman showing features of periorbital inflammation with restricted ocular movements and compressive optic neuropathy (CON). (b) Axial CT scan of same patient shows enlargement of muscles with proptosis and apical crowding
The more severe form of TED follows a biphasic course, with a progressive or active phase lasting up to 18 months, followed by a stable or inactive phase. The plot of orbital disease severity against time is called Rundle’s curve (Fig. 2.3), and a steeper slope in the active phase reflects a more acute onset with the possibility of more serious sequelae [4–6]. During the early active phase, immunomodulators and radiotherapy may be offered with the hope of limiting the destructive consequences of the immune cascade [7, 8]. Once the disease has stabilized, surgery may be considered to improve orbital comfort, cosmesis, and function. Surgery is sometimes necessary during the active phase to prevent visual loss from CON or severe corneal exposure. The stages of the disease are graded as “clinical activity.”
Fig. 2.3
Modified Rundle’s curve shows biphasic course of thyroid eye disease. The active (inflammatory) phase is represented by progression in orbital symptoms and signs on the Y-axis, typically lasting 0.5–1.5 years. This is followed by a stable phase, represented by a flattening of the curve. Immunosuppressive therapy (medication or radiotherapy) is offered during the active phase with the hope of reducing orbital sequellae, shown by a displacement of the upper untreated curve to the lower treated curve. Once the disease has stabilized, reconstructive therapy may be considered
Although TED is self-limited, it may cause permanent cosmetic disfigurement and functional visual impairment, and has been shown to impact quality of life more than chronic lung disease or diabetes mellitus [9]. Understanding the natural history of this disease helps in earlier diagnosis, in identifying those at risk for serious disease consequences, and in choosing appropriate therapy.
Incidence, Epidemiology, and Relationship to Other Autoimmune Disorders
TED is the most common orbital disease in the Americas and Europe, with an annual incidence in females of approximately 14 per 100,000 and approximately one-fifth of that for males [10]. It occurs in all races and ages and is most prevalent between the second and sixth decades [11].
TED is strongly associated with autoimmune thyroid diseases such as Graves’ disease (90 %) or Hashimoto’s thyroiditis (3 %). Autoantibodies are believed to target common receptors such as TSH-R or IGF1-R within the thyroid gland, orbital fibroblasts, and skin [1, 10, 11]. Ninety percent of patients with orbitopathy have a current or past history of abnormal systemic thyroid hormone levels (usually hyperthyroid), while others may develop abnormal levels in the future. Between 25 and 50 % of patients with immune thyroid diseases develop orbital involvement, and of those, up to one third may develop more severe consequences as mentioned above [12–14]. Graves’ dermopathy (pretibial myxedema) and acropachy/clubbing of fingers may occur in 5–10 % of patients [15].
Clinical Features
Appearance and Exposure Changes
Over 80 % of patients with TED develop upper eyelid retraction, often with an insidious onset that is first noticed by others [2]. The “thyroid stare” has a characteristic lateral flare that fluctuates with emotion or fixation giving the patient an angry look. It is associated with lid lag on downgaze, apparent spasmodic lid overaction on upgaze, and incomplete lid closure while asleep (lagophthalmos). Proposed mechanisms include increased circulating catecholamines, overaction of the levator palpebrae superioris in conjunction with the superior rectus muscle to compensate for inferior rectus restriction, or inflammation with scarring of the levator muscle or aponeurosis [16].
Proptosis is the second most common finding in TED, resulting from expansion of the orbital fat and/or muscles. It may be less conspicuous in East Asians with tight eyelids limiting forward protrusion. Complete subluxation of the globe beyond the lids is a rare but troubling complication that may lead to visual loss if treatment is delayed. Prolapse of the orbital lacrimal gland may cause a tender fullness in the superotemporal orbital rim.
The lower lid margin typically rests at or slightly above the inferior limbus. Lower lid retraction is present when sclera is visible inferiorly and is associated with increasing proptosis.
Lid retraction is measured with a ruler from the pupillary light reflex to the lid margin and proptosis is measured with an exophthalmometer or from CT scan images.
The combination of lid retraction and proptosis increases corneal exposure and may lead to symptoms of irritation, grittiness, photophobia, secondary epiphora, and blurred vision. Signs of exposure are best assessed with the slit-lamp microscope and may include corneal epithelial erosions, frank abrasions or in severe cases, ulcerations and risk of perforation. The latter complications typically result from a combination of significant lagophthalmos and the absence of the normal protective Bell’s phenomenon due to a tight inferior rectus muscle.
Periorbital Soft Tissue Inflammation and Congestion
Symptoms and signs of periorbital soft tissue inflammation or congestion include orbital ache at rest or with movement, conjunctival and caruncular injection and edema, eyelid redness and edema, and diurnal variation (worse with the head dependent after sleeping). Assessment is subjective although reliability can be improved using precise verbal descriptors or by reference to an atlas of standardized photographs [17].
Eyelid redness may be difficult to assess in darkly pigmented individuals, while lid edema may be confused with orbital fat prolapse. Orbital discomfort (at rest or with gaze) must be distinguished from ocular surface irritation, which is usually relieved by topical lubricants and anesthetics.
Various grading schemes have been described for each of these features: the simplest binary scale (present/absent) has good reproducibility, but is relatively insensitive at documenting change. Wider scoring systems may be more sensitive but have poorer concordance between observers.
These soft tissue changes may be an indicator of active inflammation but are also seen in patients with chronic congestion. Congestive features typically reflect significant involvement of orbital muscles, and thus should increase vigilance for more serious complications of the disease [2].
Restricted Ocular Motility and Strabismus
The extraocular muscles become clinically involved in only a third of patients with TED, more commonly in older individuals. Early evidence of involvement may include discomfort with ocular movement and injection over the muscle insertion sites [18]. During the active inflammatory phase, progressive restriction of motility develops, initially intermittent or in certain positions of gaze. Later in the course of disease, motility restriction may be related to secondary fibrosis.
The symptoms for strabismus are best graded using the Bahn-Gorman scale: 0 = no diplopia, I = intermittent diplopia (present with fatigue), II = inconstant diplopia (with vertical or horizontal gaze), III = constant diplopia in straight gaze, correctable with prisms, IV = constant diplopia, not correctable with prisms.
Ocular ductions can be graded from 0 to 45° in four directions using the Hirschberg principle: as the patient looks maximally in four cardinal positions, the observer points a bright light at the eyes and studies the light reflex on the surface of the eye. If the light reflex hits the edge of the pupil, the eye has rotated 15°, between the pupil edge and the limbus, 30° and at the limbus, 45°. This technique is as reliable as the “gold standard” Goldmann perimetry technique with a coefficient of reliability of 12° [19]. Strabismus can be measured objectively by prism alternate cover testing in different gaze directions.
A field of single binocular vision provides a plot of area where the patient sees single versus double because of ocular restriction. The patient keeps both eyes open and follows a specified light target on the Goldmann perimeter, indicating when the image splits into two.
Orbital CT imaging identifies which muscles are enlarged and with contrast may show increased enhancement in the fat surrounding effected muscles during the active phase [20]. In disease quiescent for many years, lucent zones are identified in the enlarged muscles, thought to be areas of hyaluronate deposition. T2-weighted MR scans may show enhancement of muscles thought to be due to edema during the active, inflammatory phase [21].
Compressive Optic Neuropathy
CON (also known as dysthyroid optic neuropathy, or DON, when relating specifically to TED) is a potentially reversible optic nerve dysfunction seen in 5–7 % of all cases of TED. Most cases are caused by direct compression of the nerve by swollen muscles in the narrow confines of the bony orbital apex, presumably impairing axoplasmic flow. In rare cases with severe fat expansion and axial proptosis, vision loss has been reported from optic nerve stretch [22].
Symptoms typically consist of desaturation of colors and blurring of central vision. This is usually confirmed on clinical examination, although a EUGOGO (European Group on Graves’ Orbitopathy) survey of its members found that 20 % of patients with diagnosed CON had Snellen visual acuity better than 6/9 [23]. Color vision impairment is a particularly sensitive test for CON, best tested with HRR (Hardy Rand Rittler) pseudoisochromatic plates. An afferent pupillary defect is a specific sign of CON but is not detected in 50 % of patients because of symmetric loss of vision. Disc edema is also a specific sign when present, but is absent in over 40 % of patients with CON [23].
CON usually presents during the active phase of TED, since the onset of visual loss provokes the patient or clinician to investigate further. However, it may also develop insidiously, sometimes with little other clinical findings of TED. Most cases are associated with muscle enlargement, with resultant subjective diplopia and motility restriction. Congestive and inflammatory features are typically present, but may be subtle. Likewise, proptosis is not typically a striking finding associated with CON, and some argue that CON is associated with tight eyelids, limiting anterior decompression of the orbit. Patients who develop CON are more likely to be male, older, and diabetic compared with their non-CON counterparts.
Coronal CT scans demonstrate the enlarged extraocular muscles crowding the optic nerve at the orbital apex and causing effacement of the surrounding fat [24]. Ancillary tests include Humphrey visual field testing, which demonstrates paracentral scotomas or generalized reduction in sensitivity in 70 % of CON cases. Visually evoked potentials (VEP) show abnormal latency in 75 % of those with CON, but are not available in many centers [23].
In spite of these clinical findings and investigations, the diagnosis of CON may be uncertain in its early stages, necessitating close follow-up.
Grading Severity
Several classification systems have been devised to grade severity of these clinical manifestations.
Dr. Werner’s “NO SPECS” classification, which clusters TED-related symptoms and signs roughly in order of presentation, provides a useful mnemonic for the different clinical features, and assigns a global severity score [25]. However, the grading system descriptors are imprecise and are often based on only one aspect of the domain, such as Snellen visual acuity for sight-threatening disease. Global ophthalmopathy scores also tend to bury the details about how the patient is specifically affected and provide insufficient information to document disease progression between visits. Finally, the NO SPECS classification does not assess clinical activity nor provide guidance for planning management.
The European Group on Graves’ Orbitopathy (EUGOGO) grades TED from mild to very severe [26]. Mild disease has minimal eyelid swelling, lid retraction, or proptosis with little or no extraocular muscle dysfunction. Moderate to severe disease implies some form of active disease with or without ocular motility dysfunction with diplopia and inflammatory features interfering with the ability to function. It may also include significant proptosis >25 mm. In these cases, medical intervention might be considered. Very severe disease refers to sight-threatening conditions such as CON or corneal ulceration, often necessitating some form of surgical intervention. This classification separates the disease into management categories, but the moderate category is a heterogeneous group comprising individuals with soft tissue changes, motility disruption, or severe proptosis. Finally, there is an implied rank order for severity that may disagree with the patient’s perception of their disease. For example, an individual with early CON might not even be aware of their color desaturation or mild central vision loss but would be categorized as severe, while another individual with marked restriction of ocular movement and bothersome diplopia would be rated as only moderately affected [2].
Clinical Activity
Rundle’s Curve
Evaluating severity of orbital changes provides a snapshot of TED on a particular visit, but equally important are measures of how the disease is progressing over time, reflecting where it lies on Rundle’s curve.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


