Fig. 10.1
Histologic appearance of extraocular muscle in Graves’ ophthalmopathy (hematoxylin and eosin). The focal and perivascular interstitial inflammatory mononuclear cell infiltrate is in close association with intact striated extraocular muscle fibers widely separated by amorphous granular material. From Bahn RS. Graves’ ophthalmopathy. N Engl J Med. 2010;362:726–38. Copyright © 2010 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society
After orbital decompression surgery, volumetric changes of EOM have been observed. Increased medial rectus muscle volume has been shown postoperatively in patients with stable TED, in whom there were clinical signs of recurrent orbital inflammation [10, 11]. The etiology of postoperative extraocular muscle volumetric changes is still unclear. If the disease process is still active at the time of decompression surgery, progression of extraocular muscle enlargement with and without compressive optic neuropathy could occur as a continuation of the process. However, this should not occur in the context of inactive disease [12]. There are several hypotheses regarding the cause of these changes. It could be reactivation of TED after orbital decompression that may have been induced by activation of antigen presenting cells and fibroblasts in the T-cell mediated inflammatory process incited by the surgery. Even a subclinical inflammatory reaction postoperatively could play a role in the early postoperative period. Alternatively, hydrostatic pressure change within the orbit and muscle secondary to the expanded orbital volume and relatively reduced intraorbital and intramuscular pressures could allow for muscle volume expansion. Glycosaminoglycans, known to be present in extraocular muscles during the inactive phase of TED by transmission electron microscopy, may be the driving force behind these changes in muscle size [7].
Imaging Findings
Neuroimaging of TED plays an important role in the differential diagnosis and interdisciplinary management of patients with TED and is required in patients with asymmetric ptosis, in suspected compressive optic neuropathy and prior to decompression surgery. Orbital imaging, such as magnetic resonance imaging (MRI), computed tomography (CT), and ultrasound show enlargement of the EOM, an increase in orbital fat tissue volume and enlargement of the lacrimal glands. Orbital MRI with fat saturation and gadolinium should be considered in a patient with decreased vision to evaluate for compressive optic nerve changes and to differentiate them from non-compressive neuropathy, in determining the appropriate intervention, and to monitor the progress or response to medical or surgical treatment. Orbital CT is the modality of choice for planning orbital decompression surgery since it provides precise imaging of the orbital apex especially of the osseous structures and it also may be considered when MRI is not available. MRI is preferred for studies assessing disease activity because of its better performance in the evaluation in soft tissues. Usually MRI is considered as both quantitative and qualitative rather than CT, which is considered as only quantitative. Orbital ultrasound offers the advantage of availability in most offices, but it has a high inter-observer variability. Orbital tissue edema, enlargement of extraocular muscles, and increase of retrobulbar fat volume are usually observed [13]. The classic morphological findings in TED are spindle-shaped expansion of typically more than one of the extraocular muscles (>4 mm) without involvement of the corresponding tendon, seen best on axial views of either imaging modality. Additionally, presentation of preferential muscle involvement, starting with early involvement of the inferior rectus followed by the medial rectus, the superior rectus, and finally the lateral rectus muscle is a characteristic finding, seen best on coronal views. In the case of long-lasting TED, a spontaneous bony decompression is noted with an impression of the normally parallel laminae papyraceae leading to the so-called “Coca Cola sign”.
MRI
MRI may help to detect disease activity and to predict the response of medical therapy. Increased T2 signal in the EOM is associated with a good response to orbital irradiation (Fig. 10.2), and STIR (Short T1 Inversion Recovery) imaging, an inversion recovery pulse sequence with specific timing to suppress the fat signal, is useful for predicting the outcome of immunosuppressive therapy. High signal intensity in T2 also is associated with a good response to methylprednisolone pulse therapy. Exophthalmos from the increase in fat tissue volume is observed more in young female patients and exophthalmos from enlargement of EOM is more typical in older male patients. Because prolonged T2 relaxation time theoretically reflects free water content as a manifestation of inflammation in the tissue, an increase of T2 signal intensity may indicate the active stage with swelling in the enlarged eye muscles. The appearance of low T2 signal intensity may indicate the progress of fibrotic changes in EOM with subsequent adhesion of the muscles to the retro-ocular tissues [14].
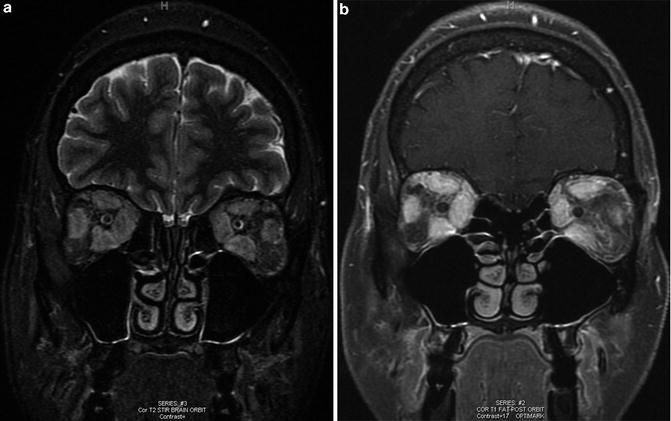
Fig. 10.2
Magnetic resonance imaging of orbit in a patient with strabismus. (a) Coronal T2 STIR, (b) Coronal T1 fat suppression postcontrast MRI, marked enlargement of the extraocular muscles bilaterally, with greatest involvement of the superior, medial, and inferior recti. There is heterogeneity within the orbital fat
CT
CT is generally the preferred imaging modality for the initial diagnosis of patients with TED because of its ability to visualize bone and soft tissues in the orbit (Fig. 10.3). It also aids the evaluation of the orbital walls, sinuses, cribriform plate, and orbital fat in planning for decompression surgery. Compared to MRI, CT is less efficient in the evaluation of soft tissue changes. CT findings in TED may include bone changes, especially in the lamina papyracea of the ethmoid, with medial bowing resulting from chronic mechanical pressure by enlarged EOM. Lacrimal gland displacement and enlargement, exophthalmos, anterior soft tissue swelling and superior ophthalmic vein dilation may also be observed. In chronic disease, fatty degeneration of the extraocular muscles might be detected as hypo-attenuated areas on CT. CT imaging may be useful in deciding whether recession and/or resection can be considered. For example, if patients have greater proptosis and larger superior rectus muscles on imaging preoperatively, they are more likely to develop late overcorrection after inferior rectus muscle recession for restrictive hypotropia. Therefore, combined superior and inferior rectus muscle recession may be considered. If the muscle is not enlarged or inflamed on imaging, resection of EOM, especially the lateral rectus muscle, may be performed.

Fig. 10.3
Computed tomographic findings in a patient with strabismus from thyroid ophthalmopathy. Coronal view, soft tissue window, showing marked enlargement of the medial and inferior rectus muscles with moderate enlargement of the superior rectus muscles. There is relative sparing of the lateral rectus muscles
Ultrasound
Both A-scan and B-scan echography are performed for evaluation of TED (Fig. 10.4). Interpretation of the images can be challenging and requires clinical expertise of a certified orbital echographer. Normal extraocular muscle has relatively lower internal reflectivity than surrounding tissue since it has homogeneous arrangement of muscle fibers. A-scans are used to assess these tissue characteristics and are particularly sensitive for identifying thickening or thinning of the muscles and for differentiating underlying pathologies. However, it is easier to visualize the orbital structures using B-scan techniques, and B-scans are very helpful in topographic evaluations and in the initial identification of individual rectus muscle enlargement. The internal reflectivity of the EOM may change as a result of tissue swelling and cellular infiltration. In the active phase, the EOM have a lower internal reflectivity, due to swelling, whereas in the inactive, chronic phase, the muscles tend to show irregular high reflectivity from the echogenic fibrotic scar tissue.
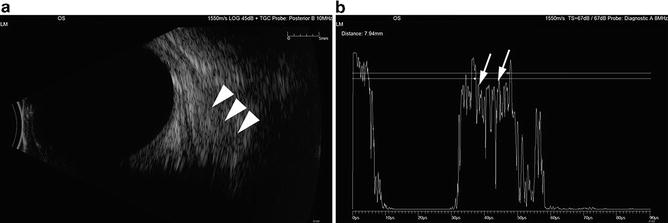
Fig. 10.4
Echographic findings. (a) B-scan ultrasound image shows enlarged EOM in retrobulbar space (arrowhead). (b) A-scan demonstrates high internal reflectivity (arrows) characteristic of thyroid ophthalmopathy
Timing of Onset of Strabismus
The incidence of strabismus in TED is somewhat variable depending on the population and timing. Between 15 and 51 % of TED patients develop strabismus, and it is most commonly secondary to restriction of extraocular motility from inflammatory and fibrotic changes [15–18]. Data from a large cohort of TED patients demonstrate that 9.2 % of patients required strabismus surgery; in comparison, 6.7 % underwent decompression procedures [19]. Most patients with TED and strabismus have a history of hyperthyroidism; however they may be euthyroid, or even hypothyroid at the time of presentation. In a large cohort of patients with TED, appearance of diplopia was seen up to 11 years after diagnosis of TED based on other orbital or eyelid findings [20]. Other signs and symptoms of TED typically start 2 years prior to the onset of diplopia. Exophthalmos, when present, usually precedes diplopia. Subclinical eye involvement is common in nearly 70 % of adult patients with Graves’ hyperthyroidism, with extraocular enlargement detected on MRI or CT [21].
As noted above, the effect of hyperthyroidism on the EOM occurs in two stages. The inflammatory phase, characterized by a lymphocytic infiltrate of the EOM and orbital tissues, may result in strabismus that changes when EOM fibrosis causes restriction of extraocular motility. Because the inferior rectus and medial rectus muscles are most often involved, hypotropia and esotropia result. Any of the rectus muscles may be involved, and recent data demonstrate more frequent involvement of the oblique muscles (particularly the inferior oblique) than previously recognized [22, 23]. Patients are often bothered by diplopia in primary gaze at distance because of common involvement of inferior rectus and medial rectus muscles. Torsional changes may also be noted because of the secondary actions of the vertical rectus muscles in addition to oblique muscle tightness.
Differential diagnosis of acquired strabismus in an adult includes cranial nerve palsies, orbital inflammatory conditions such as myositis and orbital pseudotumor, and extraocular muscle involvement with a systemic disease such as myasthenia gravis or chronic progressive external ophthalmoplegia. Graves’ disease may occur in approximately 5–10 % of patients with myasthenia gravis, and myasthenia gravis has been reported in 0.2 % of patients with Graves’ disease. Myasthenia gravis often presents with a history of variability and worsening of symptoms with fatigue. In order to differentiate these acquired strabismic conditions, orbital imaging with CT or MRI can be done to assess the extraocular muscles. In TED, the inferior and medical rectus muscles are most commonly involved. Classically, there is an enlargement of the muscle belly with sparing of the muscle tendon, which is in contrast to myositis where there is diffuse enlargement of the muscle from the origin to the tendon. Laboratory tests including thyroid hormone levels (TSH, T3, free T4, thyroid-stimulating immunoglobulin, TSH receptor antibodies) as well as acetylcholine receptor antibody tests need to be considered to evaluate for myasthenia gravis in conjunction with Graves’ disease.
Typical Findings
Over 90 % of patients with TED develop upper eyelid retraction, which is a typical and highly sensitive sign and is seen mostly in the hyperthyroid state. Proposed mechanisms for lid abnormalities in TED include increased circulating catecholamines, overaction of the levator palpebrae superioris, and superior rectus muscles to compensate for inferior rectus restriction, or inflammation and scarring of the levator complex. Similarly, lower eyelid retraction, or inferior scleral show, is associated with inferior rectus tightness. Thus, the eyelid signs should prompt the clinician to evaluate extraocular motility and alignment carefully, even if strabismus is not readily apparent and/or diplopia is not reported. Proptosis is the second most common finding in TED, but it does not correlate well with the presence or absence of extraocular motility disturbances. Lower lid retraction may be exacerbated by increasing proptosis. A tight inferior rectus muscle, which impairs the normal Bell phenomenon, together with lower eyelid retraction may worsen the corneal exposure and eye irritation that results from proptosis. The resulting blurred vision also may impair normal fusion and can induce diplopia by unmasking an underlying phoria. EOM engorgement may result from crowding at the orbital apex, and secondary orbital venous hypertension can cause conjunctival redness and caruncular swelling. It is important to distinguish this type of redness and swelling from the signs associated with active orbitopathy, as the former will not respond to typical anti-inflammatory therapies.
Any type of strabismus is possible in TED. Common patterns of strabismus in TED are hypotropia secondary to inferior rectus restriction, esotropia secondary to medial rectus restriction, and hypertropia secondary to superior rectus restriction (Fig. 10.5). Because medial rectus tightness is far more common than lateral rectus involvement, manifest exotropia should raise suspicion for an additional or alternative etiology to TED-related strabismus, such as myasthenia gravis. However, presence of a vertical heterotropia may unmask a preexisting and unrelated exophoria, and full horizontal motility may help establish this possibility although it does not exclude myasthenia. Similarly, hypertropia and A-pattern exotropia with intorsion after recession of the inferior rectus may occur. The strabismus of TED is tremendously variable with regard to presentation, findings, and response to treatment. Intraocular pressure may increase especially in upgaze and it is usually secondary to inferior rectus restriction or orbital congestion. Because this is a mechanical form of increased intraocular pressure, topical drops for lowering the intraocular pressure are often ineffective. Optic neuropathy occurs in approximately 5 % of patients with TED and it is due to compression of the optic nerve by large indurated muscles at the orbital apex. The clinical risk factors for the development of TED-related compressive optic neuropathy include medial rectus enlargement and diplopia, and careful examination of the optic disc and evaluation of automated perimetry should be performed in patients with TED-associated diplopia.

Fig. 10.5
Photograph of a patient with restrictive strabismus in the 9 cardinal gaze positions. The patient noted vertical diplopia, consistent with the asymmetric limitation of left eye depression and right eye elevation. Eyelid retraction is present as well
Initial Workup
As discussed elsewhere in this text, the diagnosis of TED is based on recognition of clinical features and may be supported by serologic tests of thyroid function and immune testing, and orbital imaging. Specialized diagnostic tests are usually not required for bilateral eye disease in the presence of autoimmune thyroid disease. If a patient presents with symptoms and signs of TED without a history of systemic thyroid disease, endocrinologic investigation including thyroid-stimulating immunoglobulin (TSI) and thyroid-stimulating hormone (TSH) levels may be required to detect any thyroid dysfunction. Abnormalities in thyroid hormonal tests (T3, free T4, and TSH) and/or the presence of thyroid specific antibodies (anti-thyroglobulin, anti-thyroid peroxidase and anti-TSH receptor) help to support the diagnosis, but they are not essential, and their absence does not exclude the diagnosis. Orbital imaging should be performed if the diagnosis is not certain from the clinical and laboratory data, or when optic neuropathy is suspected or surgical intervention is considered.
Natural History
As described in Chap. 2, TED follows a biphasic course, with a progressive or active inflammatory phase followed by a stable or inactive phase. The initial inflammatory phase may be progressive and generally lasts for 6–18 months before a plateau phase is reached. This is followed by resolution of inflammation and the final inactive “burnt out” stage [24, 25]. Graves’ ophthalmopathy activity, as judged by inflammatory signs and symptoms, is slightly separated from the curve of severity, usually evaluated based on degree of proptosis, eyelid aperture, diplopia, and visual acuity [26, 27]. According to this model, the activity peak would precede the severity peak by a few months [28].
Overall, TED improves spontaneously in approximately 60 % of cases, remains stable in 25 %, and deteriorates in about 15 % [10, 11, 28]. Congestive changes are more likely to improve than ocular myopathic changes. Extraocular muscle fibrosis may happen early in the inflammatory process, and thus patients who develop moderate to severe restriction of eye muscle function and globe excursion are less likely to experience spontaneous recovery of single binocular vision. It is our experience that the course of TED is to a large degree independent of the thyroid status but tends to be more severe in patients with poorly controlled hyperthyroidism and those rendered hypothyroid. The role of orbital decompression in the onset of diplopia remains debated. Clearly, there is an immediate postoperative onset of diplopia in a percentage of patients undergoing decompression surgery, and the incidence will vary depending upon the decompression technique used [12, 29–32]. However, the natural history of diplopia in TED would indicate that a certain number of these cases were likely to develop whether or not the patient had a decompression early in the course of their disease. The average age of patients experiencing diplopia in TED is 50, which is higher than the average age of overall TED incidence. Older patients, white males, and cigarette smokers tend to have a more severe course of the disease [7, 33–35]. Younger patients tend to have more orbital symptoms and signs and are less likely to develop strabismus with TED, while older patients tend to have more extraocular muscle involvement rather than orbital swelling [13, 36, 37].
Management
General management of TED applies to the treatment of patients with diplopia and strabismus as well; they should stop smoking and work with their endocrinologist or primary care physician to achieve a euthyroid state, although correction of dysfunction is known to have little direct effect on the progression of thyroid strabismus. Cigarette smoking adversely affects the ocular signs of TED and is correlated with diplopia in a dose-dependent manner [14, 38]. Smoking status also correlates with likelihood of needing strabismus surgery [15–18, 39]. As it is a modifiable risk factor, all patients with Graves’ disease should be advised strongly to stop smoking and have this counseling clearly documented in the medical record.
Medical Management
Systemic Corticosteroids (IV or Oral)
Moderate to severe, active, inflammatory phase of TED often responds to the systemic administration of corticosteroids particularly in cases of reduced visual acuity, visual field deficits, color deficits, or afferent pupillary defects. Systemic corticosteroids may be given orally or intravenously and may improve orbital congestion, acute ocular misalignment, and optic neuropathy. Prolonged steroid therapy is not indicated because of the risks of long-term steroid use. The best evidence points to the use of pulsed intravenous corticosteroid rather than daily oral dosing [40]. A recent randomized prospective study of IV corticosteroid dosing found that the greatest improvement in overall ophthalmic status and quality of life was observed with a regimen of 830 mg weekly for 6 weeks followed by 415 mg weekly for 6 weeks (cumulative dose 7.47 g); a lower dose scheme of 540 mg for 6 weeks and then 270 mg for 6 weeks (total dose 4.98 g) was nearly as effective and carried lower risk. However, neither regimen resulted in ocular motility improvement in the majority of treated patients, and one-third of patients in the lower dose cohort progressed despite treatment [41]. Oral prednisone at a dose of 60–80 mg/day followed by dose reduction every 2 weeks for a total treatment duration of 4–6 months is known to be as effective as IV methylprednisolone infusion twice weekly for 6 weeks, but the oral steroid may be more frequently associated with side effects [42]. We recommend using corticosteroids for diplopia when there is objective worsening of strabismus (progressive limitation of ductions) with other clinical signs and symptoms (chemosis, pain, periorbital swelling) or radiographic evidence (EOM hyperintensity on T2 MRI) of active disease. We favor intravenous steroid treatment because of the side effect profile. However, strabismus may still worsen if a fibrotic response to the inflammatory phase begins prior to the treatment taking effect.
Orbital Radiotherapy
Radiation therapy (RT) has also been used as a treatment for TED-associated strabismus. Orbital irradiation is usually given over 10–12 sessions (200 cGy each session) for a total dose of 2,000–2,200 cGy. It should not be repeated because of the risk of additive radiation, and many experts avoid radiation in patients who smoke or have other vasculopathic risk factors (e.g., diabetes mellitus). It is only indicated in patients who are in the inflammatory phase. There is controversy about the role and efficacy of orbital irradiation. It remains as a viable option for patients who cannot tolerate systemic corticosteroid therapy. The efficacy of orbital XRT for strabismus was called into question by a prospective, masked trial comparing one radiated orbit in a patient to the fellow, sham-irradiated, control orbit. In this study, no difference was observed between the two sides [43]. However, improved ocular motility, specifically with attempted elevation, has been demonstrated in other prospective studies [44]. A recent meta-analysis of available data also indicates that it may be effective in the stabilization of progressive external ophthalmoplegia. The treating physician should be aware that radiation therapy frequently has a significant lag of several weeks before any anti-inflammatory effect is seen.
Other Agents Including Biologics
Limited data on the use of biologic agents in the management of refractory TED have appeared recently in the literature. The physician must be cautioned at this juncture about recommending such therapy to patients with typical TED, given the limited power of these studies with limited patient numbers, the lack of a clear understanding regarding dosage, duration of treatment for TED, and the potential systemic side effects. The biologic agents targeting the underlying molecular basis of TED may be considered as a potential alternative therapy for TED patients who are unable to tolerate corticosteroids. Rituximab is a monoclonal chimeric antibody against CD20, a transmembrane protein present on immature and mature B cells but not plasma cells. It is approved for the treatment of non-Hodgkin lymphomas, chronic lymphocytic leukemia, and rheumatoid arthritis. Rituximab effectively depletes the CD20 B-cell population for 6–9 months. Rituximab for TED has shown improvement in the clinical activity score and sustained efficacy for >18 months [45]. Optimal dosing is not yet determined and published doses have ranged from 100 mg in a single infusion to 1,000 mg per infusion for 3–4 infusions. Most patients in published studies were treated for compressive optic neuropathy, and while available data suggest that existing strabismus did not change [46], it is possible that its anti-inflammatory effect could prevent later strabismus in patients with active TED and extraocular muscle edema rather than fibrosis.
Insulin-like growth factor 1 receptor (IGF-1R) has been suggested to play an important role in regulating the autoimmune response [47]. Graves’ autoantibodies interact directly with IGF-1R expressed on orbital fibroblasts. IGF-1R and proteins involved in IGF-1R signaling are upregulated/dysregulated in orbital fibroblasts of TED patients [48]. Graves’ autoantibodies reproduce key pathophysiological responses, specifically in orbital fibroblasts from TED patients and these responses are mimicked by IGF-1 [3]. IGF-1R and thyrotropin receptor, the two main autoantigens implicated in TED, are physically and functionally coupled in orbital fibroblasts. Inhibiting IGF-1R completely blocks pathophysiological responses in orbital fibroblasts of TED patients. The applicability of this pathway to EOM changes is not yet certain. However, it is tempting to speculate that medications that can prevent or thwart the auto-inflammatory cascades leading to extraocular muscle fibrosis would also prevent TED-related strabismus.
Conservative/Temporizing Measures
Observation may be appropriate in TED, if the strabismus is not stable and the patient does not complain of double vision in primary gaze or reading position. The patient also may choose observation when informed of the data regarding low to moderate efficacy of medical treatment to improve diplopia. If the patient is considering orbital decompression surgery for proptosis or for treatment of compressive optic neuropathy, then specific treatment of the strabismus should be deferred until decompression has been performed and orthoptic measurements are stable. One of the common complications of orbital decompression is the development or worsening of diplopia, but because the onset or worsening is frequently temporary, nonsurgical management of diplopia may be desirable. The strabismus in TED is often highly incomitant because of extraocular muscle restriction, and it may not follow specific patterns (such as worsening in gaze directed away from the tight muscle) because of multiple muscle involvement.
Prisms have been used successfully in such patients, and even high power (over 20 PD) prisms may be tolerated [49]. Press-on (Fresnel) prisms are preferable to ground-in prism when the strabismus is unstable. A properly positioned Fresnel prism can offer relief of diplopia in primary gaze and down gaze. In some patients, the degree of misalignment is too large or unstable for prism use. Other nonsurgical management options include occlusion of part or all of one spectacle lens and botulinum toxin injections into EOM. The primary goal of this management is to relieve double vision in primary and/or reading position. Occlusion with Scotch satin tape or with Bagolini filters can provide excellent and discrete relief of diplopia, compared with pirate patches [50]. Botulinum toxin may be injected into the superior rectus for the treatment of hypertropia, with a long-lasting mean reduction of 10 PD achieved after two or three injections [51]. However, post-injection ptosis is common, and patients must be aware of the high likelihood of this temporary iatrogenic ptosis.
Surgery
Principles of Surgery
Surgeries in TED usually progress in a staged, sequential fashion. Orbital abnormalities (proptosis, fat herniation) are addressed first, and they are followed by strabismus correction and eyelid repair. Not all patients require each step, of course, but the order must be considered to maximize predictability of the final results. The overall goals of surgical therapy in TED are improvement of function, reduction or elimination of diplopia, reversal of ocular surface damage, reversal of vision loss, and reduction in disfiguring proptosis and lid retraction. Successful elective surgery should be performed after appropriate medical control of hyperthyroidism or hypothyroidism with abstinence of smoking and when orbital disease has been stable [52]. The goal of strabismus surgery is to establish single binocular vision in primary gaze and reading position, to restore and maintain good fusion, and to create the largest possible field of single binocular vision. In almost all cases, surgery for thyroid-related strabismus consists of recessions of restricted rectus muscles. One of the particular challenges of strabismus surgery for TED is choosing the amount of recession to perform. In cases of a small angle strabismus, recession of a tight muscle by dosing table amounts may not have as much effect as expected because restriction is not relieved adequately. On the other hand, larger recessions can give even more effect than expected because of the combined effect of relief of the restriction and muscle retroplacement. The general concept for recession of tight muscles in TED is that larger than expected recessions are needed for small deviations and smaller than expected recession are needed for large deviations, sometimes summarized as “more is less, and less is more.” When planning surgery for vertical deviations, the effect on both primary position and down gaze for reading must be considered for optimal postoperative visual function. For hypotropia, bilateral asymmetric inferior rectus recession or placement of a posterior fixation suture on the contralateral inferior rectus may reduce the chance of overcorrection in downgaze. In other cases, if forced duction reveals the involved muscle to be too tight to prevent overcorrection, then the recession of contralateral inferior rectus muscle may be performed. Recent studies have demonstrated that selective resection of rectus muscles may be possible without creating more globe restriction [53]. Inferior oblique surgery also may be useful, as pathogenic involvement of this muscle may be more frequent than generally recognized [23].
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


