Nasal Fractures
Grant S. Gillman
Carlos M. Rivera-Serrano
INTRODUCTION/PERSPECTIVE
The face is the most visibly apparent feature of the body, and even a subtle alteration or asymmetry may be appreciable to the untrained eye. Due to the thin skin overlying the nasal dorsum, it has been said that a displacement of even as little as a few millimeters may be perceptible (1). Furthermore, beyond the aesthetics of the nose, it is equally important to consider the functional impact that trauma may bring to bear on the nasal airway.
Not surprisingly given the prominence of the nose as a facial feature, the nasal bones are the most commonly fractured of all facial bones and the third most common fracture of the adult human skeleton (2,3,4,5,6,7,8,9,10,11,12,13,14). It has been estimated that there are approximately 50,000 nasal fractures per year in the United States though the actual number is likely higher due to underreporting, patients not seeking medical attention, and fractures that are overlooked in the multitrauma setting (7,9). Nasal fractures occur two to three times more frequently in males and are most commonly seen between 14 and 50 years of age (7) with a peak incidence between the second and third decades of life (6).
Of all facial fractures, about 40% involve the nose (3,9,15). When one considers all patients with facial skeletal fractures, about 20% will have multiple facial bone injuries and so even in those cases where only an isolated nasal fracture is suspected, it becomes critical to complete a thorough examination (16). Kim and Yoon (17) have reported that 47% of all nasal bone fractures are associated with fractures of the nasal septum, and in a different study where the septum was explored in all patients undergoing fracture reduction, Rhee et al. (11) reported that septal fractures were actually identified in over 90% of nasal fractures (8).
Individuals with a prior history of nasal fractures have a 15% to 20% chance of sustaining another nasal trauma in the future, as the “lifestyle” of some patients may increase their predisposition to repeated nasal trauma (7). In those who have had a prior rhinoplasty, the nasal bones may fracture more easily and the incidence of nasal bone fractures may also be higher than in the general population (18).
There are multiple considerations, treatments, and differing opinions when it comes to the treatment of nasal fractures but surgeons generally agree that an optimal outcome should address both cosmetic and functional issues. Recommended treatments for nasal fractures range from no intervention at all (if undisplaced and asymptomatic) to extensive surgery using rhinoplasty techniques through open approaches (19,20). One of the most challenging aspects of managing nasal fractures remains the high incidence of a posttraumatic nasal deformity, either externally or in terms of the nasal airway. At a minimum, the goal of nasal fracture management should be to reestablish the preexisting nasal airway and cosmesis. Beyond that, if there was already preexisting pathology, one is very unlikely to attain an optimal nasal airway and cosmetic result with closed reduction techniques alone. The difficulty in the management of nasal fractures is that even when they are recognized, the mechanism of injury and pathophysiology are often poorly understood leading to inappropriate treatment and suboptimal outcomes.
STRUCTURAL ANATOMY
The external nose is pyramidal in shape and mainly composed of the thin nasal bones, the thick frontal (ascending) process of the maxilla, the nasal process of the frontal bone, and the upper and lower lateral cartilages. The paired nasal bones articulate with each other at the midline, with the frontal bone superiorly and ascending process of the maxilla superiorly laterally (Fig. 83.1). The nasal bones tend to be thinner and broader at their caudal end and are therefore more vulnerable to fractures inferiorly than superiorly (21).
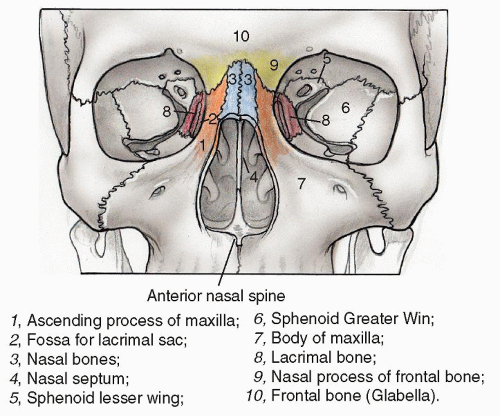 Figure 83.1 Structural anatomy of the nose. |
The cartilages that contribute to nasal structure are the upper lateral, lower lateral or alar, sesamoids, and the quadrangular septal cartilage. The triangular or trapezoidal- shaped upper lateral cartilages, by virtue of their attachments to the undersurface of the nasal bones superiorly and the dorsal septum medially help provide significant support to the midline location of the septum and the stability of the middle nasal vault (5,22). The lower third of the nose is made up of a complex architecture and relationships between the cartilages, nasal septum, and soft tissue. The lower lateral cartilages are one of the major nasal tip support mechanisms and the strength, resiliency, and orientation of these structures will affect both tip projection, tip symmetry/alignment, and stability of the lower third of the nasal sidewall and the external nasal valve (23).
The nasal septum is made up of the quadrangular cartilage anteroinferiorly, the perpendicular plate of the ethmoid bone superiorly, and the vomer posteroinferiorly. The quadrangular cartilage articulates along its dorsal edge with the upper lateral cartilages and inferiorly along the floor of the nose with the maxillary crest. The septal cartilage acts as a central strut or “tent pole,” supporting the middle and lower thirds of the nasal dorsum (20,21). The perpendicular plate of the ethmoid and the vomer articulate with the posterior end of the septal cartilage caudally and the nasal bones anteriorly, but provide less support to the upper third of the nasal dorsum than the quadrangular cartilage does to the lower two-thirds of the nose (20,21).
The nose has a very rich blood supply. The blood supply of the external nose is provided through branches of the internal and external carotid systems—the facial artery anteriorly (which becomes the angular artery superomedially) and the infraorbital and ophthalmic arteries dorsally. Internally, the blood supply to the lateral nasal wall comes from the sphenopalatine artery posteroinferiorly, and the anterior and posterior ethmoidal arteries superiorly (24). The skin and soft tissue of the nose varies in thickness, being loose and thinner in the dorsum and upper third, and thicker and more adherent at the tip (22). Sensory innervation of the nose is provided by branches of the ophthalmic (V1) and maxillary (V2) divisions of the trigeminal nerve.
PATHOPHYSIOLOGY—MECHANISM OF INJURY
Less force is required to fracture the nasal bones than any other fracture of the facial skeleton (14,25,26). Blunt nasal trauma is a more commonly seen mechanism of injury than penetrating nasal trauma, and lateral forces occur more frequently than frontal or inferior forces. Inherent variations in anatomy as well as the amount and direction of applied forces will influence the fracture pattern and resulting deformity (14,25,26).
With respect to individual anatomic variation, comminuted fractures are more likely to occur in elderly patients because their nasal bones tend to be thinner. In children, dislocations are more common than fractures owing to the fact that the nose has a higher proportion of cartilage to bone in the pediatric population.
In general, the greater the force of impact the more significant the expected nasal deformity. Furthermore, because the caudal end of the nasal bones is thinnest, a fracture of the thicker more cephalic aspect of the nasal bones requires greater force and is therefore more likely to be associated with other facial fractures.
While variability is inevitable with respect to both susceptibility to nasal fractures and nasal fracture patterns, cadaveric studies have enabled some general observations to be made (25,27,28). Although fractures are more commonly caused by a lateral force, a blow from any vector can fracture the nose. A greater force is required to fracture the nose from a frontal impact than lateral impact, because the nasal bones are to some extent buttressed to a frontal blow by the perpendicular plate of the ethmoid bone, the elasticity of the septal cartilage, the anterior nasal spine, and the frontal process of the maxilla.
A less forceful lateral impact may result in undisplaced sidewall fractures, without symptomatic nasal obstruction and should not require any manipulation or treatment. With increasing lateral force an ipsilateral displaced nasal bone infracture first occurs, without affecting either the septum or contralateral nasal bone (Fig. 83.2). This will be apparent externally and can affect the nasal airway as well and as such reduction is recommended. The ipsilateral depression may create the illusion of curvature to the nose (Fig. 83.3), but typically the contralateral bone is not particularly tender, thereby suggesting the diagnosis of a unilateral fracture. As force increases, a lateral impact will break both nasal bones (often an ipsilateral infracture and contralateral outfracture) (Fig. 83.4) as well as the bony and/or cartilaginous septum secondarily with lateral displacement of the entire nasal pyramid and obstruction of the nasal airway (Fig. 83.5).
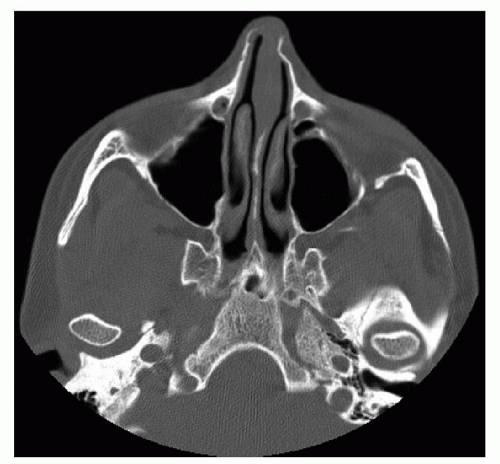 Figure 83.2 Axial CT scan showing unilateral depressed fracture of left nasal bone. |
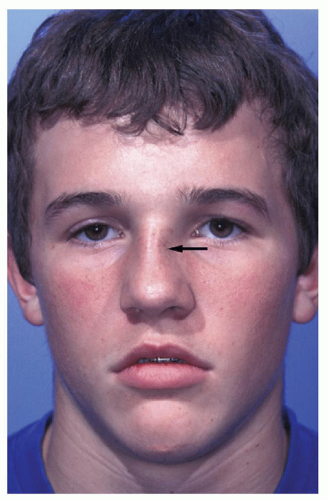 Figure 83.3 Unilateral impacted left nasal bone fracture (arrow) generating the illusion of an apparent curvature of the nose to the patient’s right. |
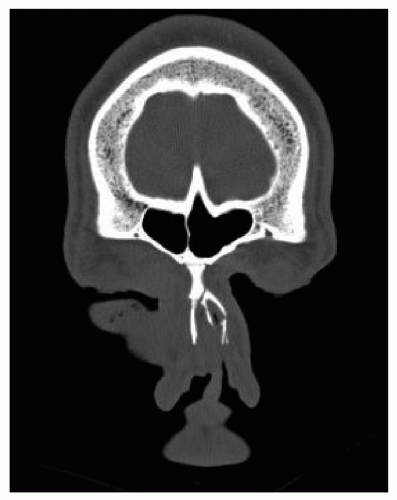 Figure 83.4 Coronal CT scan showing bilateral displaced nasal bone fractures with concomitant nasal septal fracture. |
Similar to the situation with lateral forces, a lesser amount of frontal force may fracture the thinner distal end of the nasal bones without visible displacement or external deviation. If there is sufficient force for displacement of the nasal bones, the upper lateral cartilages, which are attached to the undersurface of the nasal bones may get impacted with the nasal bones or avulsed from the nasal bones with both an external deformity and a reduction in nasal air- flow. As the force from a frontal impact increases, the septum may buckle, dislocate, or fracture and the bony nasal cap can be impacted (Fig. 83.6), comminuted, and splayed with widening of the nasal bridge and lateral displacement of the nasal bones. Fracture or dislocation of the septum will inevitably lead to nasal airway obstruction.
A very forceful frontal or central impact to the osseous and cartilaginous nasal structures can be transmitted posteriorly to the nasoorbitoethmoid (NOE) complex leading to nasoethmoidal fractures (8). A NOE fracture is a complex fracture that can involve the nasal, ethmoid, frontal, lacrimal, maxillary, and orbital bones as well as the cribriform plate. A complete review of NOE fractures is beyond the scope of this chapter, but they should be recognized as the treatment is far more complicated and the sequelae, if untreated, much more disabling. These patients will present with additional signs and symptoms that can include marked periorbital edema and ecchymosis, telecanthus, enophthalmos, epiphora, telescoping of the nasal dorsum with a flattened nasofrontal root and midfacial retrusion, and possibly a cerebrospinal
fluid (CSF) leak. Further discussion and management is reviewed elsewhere in this text.
fluid (CSF) leak. Further discussion and management is reviewed elsewhere in this text.
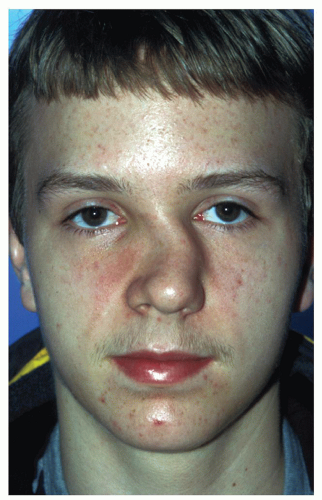 Figure 83.5 Patient with acute, bilateral displaced nasal bone fractures. |
Injury to the nose from an inferior vector is more likely to traumatize the cartilaginous septum with or without a fracture of the nasal bones themselves. Sufficient impact from below can dislocate the caudal septum off of the anterior nasal spine or maxillary crest with displacement to one side or the other. This can result in asymmetry of the nostrils and nasal base, inferior septal spurs, and even twisting of the nasal tip because of the proximity of the caudal septum to the lower lateral cartilages. Fractures of the septal cartilage can also occur with telescoping of segments leading to columellar retraction and/or nasal obstruction.
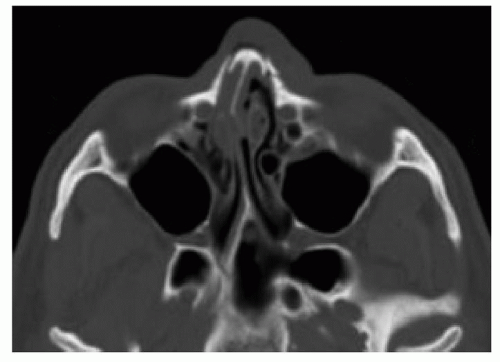 Figure 83.6 Axial CT scan showing impacted fracture of bony nasal cap. |
The severity of airway obstruction accompanying nasal fractures depends on the location of the septal fracture and the presence of septal displacement with the latter being the most important variable in nasal obstruction (10). The nasal septum functions somewhat as an energy-absorbing structure (8), with the ability to dissipate a certain amount of force and rebound without significant deformity. Beyond that point, the septum will either dislocate or fracture.
Dislocations, as opposed to fractures, are more commonly seen where the cartilage tends to be thicker and stronger—namely right at the bony-cartilaginous interfaces (28), either posterosuperiorly at the perpendicular plate of the ethmoid bone or inferiorly at the maxillary crest. On physical examination, this would correspond, respectively, to either angulation of the quadrangular cartilage at the junction with the perpendicular plate of the ethmoid or the appearance of a long septal spur inferiorly.
Fractures of the septum on the other hand tend to occur in the thinner central portion of the quadrangular cartilage above the bony cartilaginous interface or through the bony septum (ethmoid and/or vomer) (28). In separate cadaveric studies, Murray et al. (25) and Harrison (28) noted remarkably similar septal fracture patterns with application of sufficient impact force. The fracture line in the cartilaginous septum was typically several millimeters above the maxillary crest, extending posteriorly into the bony septum and curving upward through the vomer into the vertical plate of the ethmoid to yield a C-shaped fracture pattern (Fig. 83.7). Fracture fragments can then either overlap, telescope, or pivot to obstruct the nasal airway. Rohrich and Adams (29) likewise noted that low-velocity injuries tended to occur inferiorly as either dislocations or fractures, while high-velocity injuries or frontal impacts resulted in more extensive fractures in the thin central portion of the septal cartilage extending posteriorly into the ethmoid or vomer.
Another observation of Murray et al. (25) in their cadaveric study of fracture patterns was that if the nasal bones were displaced by more than half the width of the nasal bridge there was inevitably a concomitant C-shaped fracture of the bony and cartilaginous septum as described. Under such circumstances, they concluded that open treatment of the septum with resection of the interlocked or overlapped segments incorporating the fracture inferiorly and posteriorly was required in order to achieve optimal alignment of nasal injuries of this severity. The implication of septal fractures as they relate to success or failure in the management of nasal fractures is discussed at greater length later in this chapter.
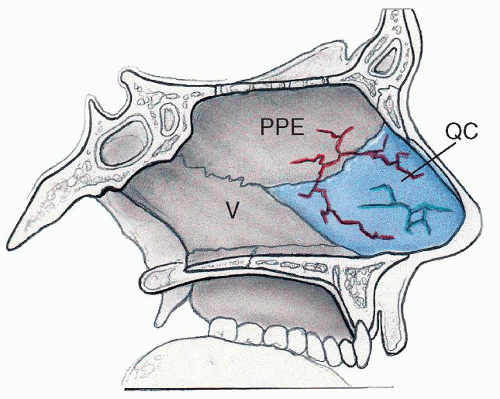 Figure 83.7 Typical nasal septal fracture pattern seen in cadaveric studies. (V = vomer, PPE = perpendicular plate of ethmoid bone, QC = quadrangular cartilage) |
DIAGNOSTIC ASSESSMENT
The diagnosis of a nasal fracture is generally made based on the history and clinical exam. Patients who present with nasal trauma may well have additional injuries and should be routinely examined in a comprehensive and orderly fashion as with any other trauma patient to minimize the likelihood of overlooking concomitant injuries.
History
A thorough history is the cornerstone of the diagnosis and will frequently guide the management of nasal fractures as well. It is helpful to know when the incident occurred, the mechanism of the trauma, the direction of the force, patient symptomatology (in particular, whether or not there has been any alteration in alignment or change in the nasal airway), whether or not there is a prior history of nasal trauma or nasal surgery, the patient’s medical history and comorbidities, age, and patient expectations. Epistaxis is considered to be a sine qua non for nasal fractures (30) and suggests a disruption of or tear in the nasal mucosa.
Understanding the mechanism of injury is helpful for the workup and management of the patient with nasal trauma, but is not as critical as the physical exam for planning the reduction or surgical technique. As discussed earlier, the velocity and force of impact will influence the pattern and extent of the underlying injury. In general, a greater impact should heighten one’s suspicion for additional injuries, for a more complex nasal fracture pattern, and for an associated septal fracture or dislocation.
The timing of the injury is another important variable to know in the scenario of a nasal fracture. Management decisions regarding nasal and septal fractures depend on reliable visual and tactile information that the surgeon interprets when first examining and later manipulating or reducing the nasal complex. Excessive soft tissue edema can mask minor or modest irregularities and preclude an accurate understanding of the fracture pattern and degree of displacement. The classical two windows of opportunity for nasal fracture management described in the literature are therefore based on the rationale of manipulating the nasal complex in the absence of significant edema. Nasal edema is generally limited within the first 2 to 3 hours after the trauma, and has settled to a certain degree 5 to 10 days after the injury. On the other hand, after 2 to 3 weeks of healing a fibrous union is developing across the fracture line making the reduction more challenging and often mandating the use of osteotomies that might have otherwise been unnecessary to enable repositioning of the nasal framework.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


