OVERVIEW
- Nasal physiology, key sinonasal symptoms and conditions that cause nasal discharge in children and adults are considered
- Postnasal drip is just a symptom and not a disease—it may just reflect normal physiology
- A comprehensive history is of paramount importance in managing rhinological disease
- CT scans of sinuses should be requested only after adequate medical therapy of rhinosinusitis; plain sinus radiographs are no longer recommended
- The management of rhinosinusitis and urgent referral are both considered
Nasal discharge is one of a complex of sinonasal symptoms that we all have experienced at some stage. However, once it becomes predominant and persistent it can instigate a need for medical advice.
Normal physiology
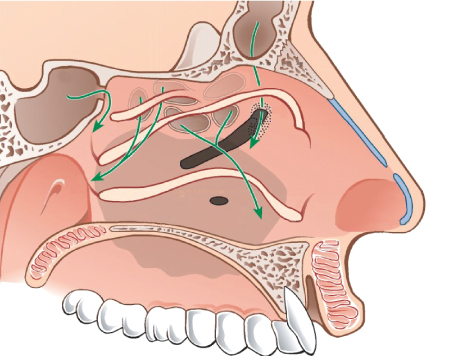
It is important to understand the normal anatomy and physiology of the nose to enable a judgement to be made about the significance of the various clinical complaints that patients describe (Figure 12.1).
Figure 12.1 Anatomy of lateral nasal wall and sinus drainage pathways. (Used with permission from Thieme Publishers.)
Mucus physiology
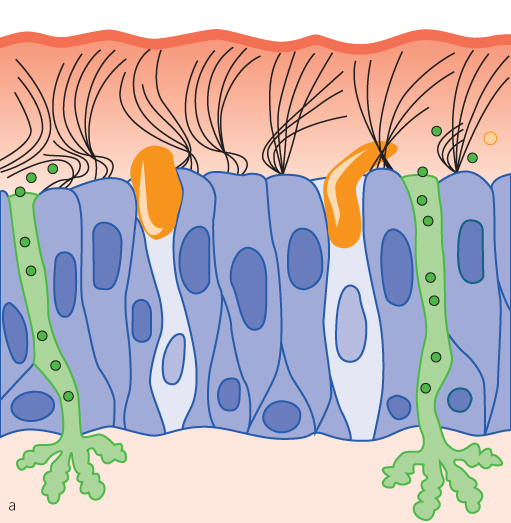
The nasal mucosa is a specialized dynamic lining that is covered with mucus (Figure 12.2). This mucus is part of the normal clearance mechanism that traps inhaled particles and is swept to the back of the nose where it flows down to the pharynx and is subsequently swallowed—a phenomenon known as mucociliary clearance. This normal physiology happens without awareness in most people. However, any alteration in awareness, mucus viscosity or volume may present with the classic symptom of so called ‘post’ nasal drip (vida infra).
Figure 12.2 Diagram of nasal mucosa and overlying mucus layer. (Used with permission from Thieme Publishers.)
Mucosal physiology
The nasal mucosa itself is dynamic due to its specialised vascular structure, particularly over the inferior turbinates. The blood vessels control the degree of blood flow and thus vary the degree of congestion of the mucosa. This variation is determined centrally by the autonomic nervous system. In a healthy nose, this induces variation in the airflow between the two sides of the nose, over the course of several hours; a process known as the nasal cycle. It is therefore normal to have a better airflow on one side of the nose that changes to the other side with time. When this normal physiology is affected by rhinitis, patients complain of their nose being either blocked or runny, often in a cyclical sequence.
Congestion of the nasal mucosa is affected by nasal reflexes: the nose will feel more blocked whilst lying in a supine position, and lying on one side causes the downmost side of the nose to block. Rhinitis will exaggerate these reflex changes. Exercise will generally clear the nose.
Taking a sinonasal history
The first challenge when dealing with nasal discharge is to gain a clear understanding of the patient’s actual symptoms. Since diagnosis normally relies on accurate history, it is best to use the words or terms that the patient recognises as part of what they actually experience.
In practice, a patient who is asked whether or not they have a nasal discharge often returns a blank or quizzical look. The use of descriptive terms and questions in a short conversation is therefore usually much more effective in eliciting the desired response. Patients should be asked whether their nose runs, drips or whether their nose is ‘snotty’ or if they need to sniff or blow their nose excessively. They should also be asked about mucus dripping into the throat, and whether they can cough or spit this out.
Once the history of discharge is established, the nature of the discharge can be explored. Key factors include the tenacity, colour, persistence and variation. Nasal discharge from the nostrils is termed anterior in contrast to mucus passing into the throat, which is termed posterior discharge.
Nasal discharge is a normal occurrence with head colds and usually this takes about 3 weeks to clear. The normal nose will also run temporarily in extreme cold conditions or when exposed to irritants.
Young children do not naturally blow their noses and their nasal airway is anatomically compromised. Nasal discharge is therefore a common and normal finding.
Excess mucus may be produced without any obvious underlying cause and patients may describe this as “catarrah”. Discoloured or green-yellow mucus is consistent with chronic rhinosinusitis, but mucus that is not cleared quickly from the nose will become discoloured, particularly in the early morning after sleep.
The ‘postnasal’ drip
This term refers to the sensation of mucus at the back of the nose, but in most patients no abnormality can be seen.
There is a common misunderstanding that this mucus drips into the lower airway and then infects the lungs, but this is untrue. It is, however, true that inflammatory disorders of the nose are closely linked with those of the chest.
Chronic infection within the sinuses may cause a mucopurulent discharge into the nasopharynx. Mucus may be visible in the oropharynx but endoscopy of the nose is often required to see the more subtle findings of a mucus track.
Primary and associated sinonasal symptoms
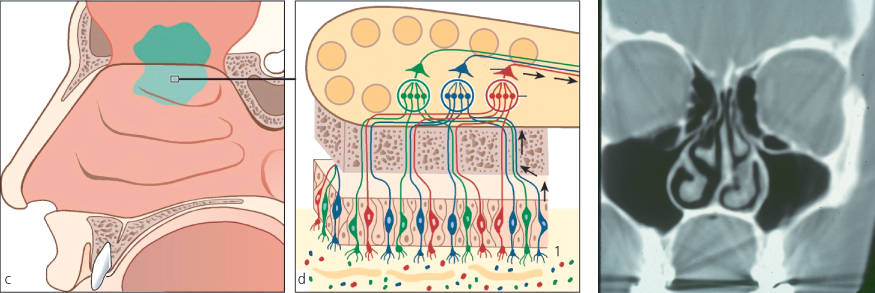
Most patients with sinonasal disease complain of nasal obstruction and discharge is an important accompanying symptom. The other primary symptoms include facial discomfort/pain and loss of the sense of smell (Figure 12.3).
Discharge may be anterior from the nares or posterior when it induces throat clearing. In patients with rhinitis, discharge may alternate with obstruction.
The following symptoms need to be assessed in order to build up the sinonasal profile (Box 12.1).
I. Sinonasal symptom list
- Nasal obstruction
- Nasal/post nasal discharge
- Headache/facial pain or discomfort
- Sense of smell
- Recurrent episodes of acute sinusitis
II. Other relevant factors
- Asthma or symptoms of asthma if not previously diagnosed, should be sought
- Allergy, particular to inhaled allergens should be identified
- Sensitivity to aspirin should be recognized in patients with nasal polyps and asthma
- Smoking or exposure to irritants should be noted
- Family history of polyposis
- History of previous polyp surgery is essential information
The extended rhinological history
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


