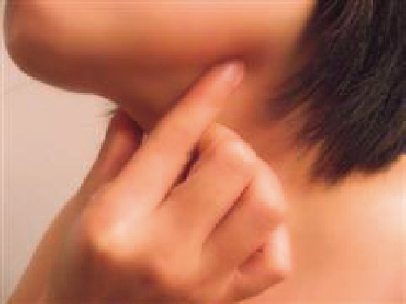
20 Muscle Tension Dysphonia Muscle tension dysphonia (MTD) is a condition that is defined by increased tension of the intrinsic and extrinsic muscles of the larynx that results in a pathological disturbance of voice. MTD was originally described by Morrison et al in 1983 in response to the observation of voice changes in response to stress.1 Since then MTD has evolved considerably in both the use of the term and its clinical definition. The condition of MTD has been plagued by a lack of standardization in its use. MTD is often incorrectly used interchangeably with the term “functional dysphonia” and has been used to categorize the amalgam of voice conditions that are not considered secondary to a defined lesion. This ambiguity has led to the use of MTD as a catchall diagnosis for dysphonia not otherwise specified by otolaryngologists who are not well versed in the management of voice patients. Further complicating the diagnosis of MTD is the lack of evidence and agreement in the literature describing the epidemiology, etiology, pathophysiology, methods of diagnosis, and management. There is great variability in the clinical presentation of MTD. As a result of this variability, making the diagnosis may be challenging and the condition may be equally challenging to treat. The purpose of this chapter is to provide the otolaryngologist with a better understanding of MTD and provide a practical approach to its diagnosis and management. There are very few studies existing that attempt to characterize the epidemiology of MTD. The true prevalence is unknown, although estimates of those with “voice disorders” range from 0.65 to 15% of the general population.2,3 Roy et al found that almost 30% of their study group had a voice disorder sometime during their lives.3 Several studies report that MTD accounts for at least 10 to 40% of visits to voice centers.4–6 Yet, true incidence data are difficult to obtain given the aforementioned inconsistency in terminology and the variable nature of the disease. It has been shown that 40% of dysphonic patients do not have an obvious organic cause.7 The data that exist show a strong correlation with voice use. As a result, singers, teachers, salespeople, and those whose occupation requires daily intensive voice use are much more likely to be diagnosed with MTD. Laryngopharyngeal reflux (LPR), high stress levels, recurrent respiratory illness, exposure to inhaled irritants, female gender, and advanced age have all been associated with greater risk of developing MTD as well.3,8–10 MTD is generally divided into two different subtypes, primary and secondary. Primary MTD is characterized by dysphonia with increased laryngeal tension, without any identifiable mass or neurogenic lesions, and in the absence of any psychological disorder.4 Secondary MTD is characterized by excess muscle contraction that develops in association with or as a presumed response to an identifiable organic lesion, such as a vocal fold mass or nerve paresis which impairs glottal function. The response of the body to the glottal malfunction is to attempt to regain “normal” function through increased activity in the intrinsic and extrinsic laryngeal musculature. Due to this increased activity, patients with long-standing primary MTD may have an increased propensity to develop organic lesions, thus creating a self-reinforcing cycle.11–13 MTD can be caused by a multitude of inciting events as they relate to the risk factors discussed previously. Most often the clinician is not able to identify the specific cause for the maladaptive voicing pattern. However, regardless of the etiology, the end result of increased laryngeal tension follows a typical physiological pattern. These patients develop into a state of hyperfunction of the tongue base, neck, and laryngeal muscles, often both during phonation and at rest. The muscles affected include two groups: the intrinsic laryngeal muscles and the extrinsic muscles. The intrinsic muscles include the thyroarytenoid, cricothyroid, lateral and posterior cricoarytenoid, and interarytenoid muscles. The extrinsic group is further divided into those in the perilaryngeal region and those more closely related to the tongue base and floor of the mouth. In the perilaryngeal region, these include the sternohyoid, sternothyroid, thyrohyoid, omohyoid, and sternocleidomastoid muscles. In the tongue base region, these include the digastric, mylohyoid, genioglossus, and hyoglossus muscles. The upper esophageal sphincter (UES), comprised of the cricopharyngeus and thyropharyngeus muscles, has also been implicated by some as contributing to laryngeal position and tension. This could in part help explain the association that LPR may have with MTD.14 The extrinsic muscles are generally responsible for elevation of the laryngeal complex during swallowing. They are not activated under normal circumstances during voice production. In patients with MTD, however, they are found to be chronically contracted during voicing, and often even at rest. This hyperfunction generally results in elevation in the position and alteration in the tilt of the larynx.4,13,15 Changes in the position and forces on the larynx then ultimately lead to changes in the intrinsic muscle function. This may lead to abnormal stress within the vocal fold and specifically the superficial lamina propria.16 The effect of this abnormal and inefficient vibratory pattern on the vocal fold leads to edema within the lamina propria, which can then cause changes in vocal quality.16,17 The cumulative effect of these vocal stresses can lead to the development of benign vocal fold lesions such as nodules, cysts, polyps, and granulomas. When evaluating a patient with possible MTD, it is especially important to pay attention to details of the history and physical examination. Rarely does one point of the history or feature of the examinations allow the physician to confirm the suspected diagnosis. There is a significant variability in the way patients present. As a result, it is important to evaluate the entire set of patient data to arrive at the correct conclusion. The patient histories in MTD do, in general, follow a basic pattern. Their symptoms typically include voice changes for a prolonged duration, from months to years. They will state that they have vocal fatigue that is worse at the end of the day and exacerbated by prolonged voice use. Often they complain of throat discomfort and tightness. When probed further, they frequently have chronic throat clearing that is worse with voicing. They can have variable globus sensation as well. Interestingly, Perera et al demonstrated a significant increase in upper esophageal pressure in normal patients during phonation, which could explain in part this phenomenon.18 Frequently, patients state that they have undergone previous trials of antireflux medications without improvement in their symptoms. Clinical Pearls Most common complaints: •Hoarseness •Vocal fatigue •Reduced range when singing •Globus sensation •Throat discomfort that is worse with voice use •Chronic cough and/or throat clearing It is important to explore potential risk factors for the development of maladaptive voicing patterns. First and foremost, occupational, recreational, and home voice use should be thoroughly explored. Extended telephone use, public speaking, singing, and crowded home environments are found to be recurring themes with this population. They should be questioned about respiratory illness or laryngitis that was temporally related to the initiation of their complaints. Traumatic injury, as well as chronic neck and spine issues, can lead to an alteration in posture and consequently neck muscle activation. LPR symptomatology should be elucidated along with correlation between reflux and voice symptoms. Lastly, primary spoken language should be considered as some languages require more activation of the tongue base and extrinsic muscles. The physical examination for patients with voice disturbances builds upon the standard head and neck in important ways. First, there needs to be a greater focus on the examiner’s perception of the patient’s voice. Evaluation of the voice should include both spontaneous speech and phonemically balanced reading samples such as the Rainbow Passage, the Zoo Passage, or those sentences used in Consensus Auditory-Perceptual Evaluation of Voice tool. Voicing features can differ greatly between these two activities and help differentiate MTD from other voice disorders such as spasmodic dysphonia (SD) or Parkinson disease. Attention should be paid to the overall grade of the voice, degree of vocal strain, and whether resonance or vocal tone focus is in the throat or ideally in the anterior vocal tract. Perceptually, the typical MTD patient’s voice has a rough, strained quality with reduced airflow or a breathy strained quality. The second aspect of the examination that should receive greater attention is the manifestation of elevated tension in the tongue base and anterior neck. Difficulty in relaxation of the tongue base can be assessed when evaluating the oral cavity with a tongue depressor and more reliably on insertion of a rigid 70-degree endoscope during stroboscopy. Tongue out and lip trills (raspberries) are useful maneuvers that can help elucidate the presence of tongue base tension. The neck should be evaluated for exaggerated movement of the submental muscle groups during phonation, suggesting tongue base activation (Fig. 20.1). On palpation, the relative locations of the hyoid bone and thyroid cartilage should be assessed. In individuals without MTD, there is a relaxed nontender space between these structures (thyrohyoid space; Fig. 20.2). There is little movement of the hyoid and thyroid cartilage during relaxed voicing, while the thyrohyoid space is maintained in a relatively stable position. In MTD patients, the thyrohyoid space may be reduced or asymmetric at rest and during phonation due to contraction of the extrinsic laryngeal muscles. As a diagnostic maneuver, moderately firm circumlaryngeal palpation can be applied to the region around the larynx and thyrohyoid space. Due to chronic hyperactivity in the strap muscles, patients with MTD will generally report discomfort during this maneuver. Postural asymmetry or an irregular neck position should alert the physician to explore the reason because these can result in increased tension in the perilaryngeal muscles. Figure 20.1 Suprahyoid palpation—palpation of this region will help reveal increased tongue base activation.
Epidemiology/Etiology
Pathophysiology
Patient Evaluation
History
Physical Examination
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


