Pediatric Ophthalmology
Edited by P. F. Gallin
Thieme Medical Publishers, Inc.
New York ©2000

11

Motor and Sensory Tests
To understand strabismus in patients of any age, it is necessary to thoroughly evaluate motor and sensory status. With this evaluation, the examiner makes a diagnosis, plans therapy, and predicts the prognosis.
To accurately perform the various tests, it is necessary that the patient maintains fixation on the object of regard (target). To assure this, a constant flow of conversation by the examiner is helpful. In the verbal patient, this conversation is usually in the form of questions. Most children want to answer correctly and enjoy this rapport with the examiner. Ask the child about clothes, activities, siblings, birthdays, and nursery school. Also, attentive fixation assures better control of the accommodation.
 Motor Evaluation
Motor Evaluation
Heterophoria vs. Heterotropia
The first step in evaluating motor status is to determine whether the eye alignment is a latent (hiding), intermittent, or constant deviation. If stabismus is present, it is essential to be aware of any variability in the angle of deviation.
Cover-Uncover Test
Currently, one of the most accurate methods of evaluating the motor picture is the cover-uncover test. Each eye in turn is covered and uncovered, allowing binocularity to exist in the interval between the covering maneuver. The occlusion can be with a plastic occluder, the hand, or the fingers. Fixation is controlled by an accommodative target (at distance or near) throughout the testing procedure.
Two observations are made (Table 11-1). (1) The uncovered eye is observed when the other eye is covered. No movement of either eye when one eye is covered indicates no strabismus. Movement of the uncovered eye indicates strabismus. Care is taken that alternate fixation does not occur during the binocular situation. An esotropia is present if the uncovered eye moves out to fixate the target, an exotropia is present if the uncovered eye moves in to fixate, and a hypertropia or hypotropia is present if the uncovered eye moves up or down to fixate, respectively. (2) A tropia is present when the uncovered eye moves. A phoria is present when the covered eye moves. The covered eye is observed as the cover is removed. In the presence of heterophoria, the eye under the cover assumes a fusion-free position. When the cover is removed, the eye performs a fusional movement to resume bifoveal fixation. After determining the status of the deviation (i.e., heterophoria vs. heterotropia) with the cover-uncover test, the next step is to measure the amount of the deviation.
| Cover-Uncover Alternate Cover | Prism Direction | Diagnosis |
|---|---|---|
| No movement | No movement | No strabismus (orthophoria) |
| Uncovered eye moves out | Prism base out | Esotropia |
| Uncovered eye moves in | Prism base in | Exotropia |
| Covered eye moves out | Prism base out | Esophoria |
| Covered eye moves in | Prism base in | Exophoria |
Alternate Cover and Prism Test
Clinically, the most accurate test to measure the full amount of the deviation in patients with central fixation is the alternate cover and prism test. The patient fixates a target, controlling accommodation by having the child identify different optotypes or features of a picture or toy. The cover is alternated from one eye to the other eye. If there is no movement of the eyes after prolonged alternate cover, orthophoria is suspected. However, to prove that orthophoria exists, a 2-prism diopter (pd) is introduced base in, base out, base up, and base down. If reverse movement is noted in all four directions, then orthophoria exists. If there is movement of the eyes with alternate cover, a deviation is present. The cover is alternated from one eye to the other as appropriately held prisms are increased until the end point is reached (i.e., no movement of the eyes).
Prism base-out for esodeviation
Prism base-in for exodeviation
Prism base-down or -up for hyperdeviation
The point of the prism is in the direction of the deviation, for example, eye moves in in esotropia so base out/point in. However, to ensure the maximum end point, the prisms are increased until reversal of movement is noted. To uncover the full amount of the deviation, prolonged dissociation of the eyes with the cover along with slowly increasing the prism strength is helpful. The patient should never be allowed to see binocularly until the measurements are determined. At times, more deviation can be elicited by asking the patient to relax and give up eye control. This is particularly true for patients with heterophoria or intermittent deviations, yielding a range of prism measurements. Correcting both horizontal and vertical deviations to the end point with the appropriate prisms is advised. Correcting one meridian may influence the amount of deviation in the other meridian. The secondary component of a deviation may become more prominent postoperatively, and this could be disturbing if not previously detected and measured. These measurements are done and recorded at distance fixation in primary position. (They are also done at distance fixation in right and left gaze to rule out lateral gaze incomitance and in up and down gaze to rule out A and V patterns. If a vertical deviation is measured in any of the previosly mentioned directions, then the measurements are done at distance with the head tilted to either side approximately 30 degrees. The results of this head tilt test will help incriminate the offending vertical muscle. The prism is held parallel to the lower lid fissure.1) Alternate cover-prism measurements are repeated at near fixation, with and without +3.00 in primary position. (Measurements are done at near fixation in four diagnostic positions of gaze: right, up and down, and gaze left, up and down.) The results of these measurements are recorded as follows:
| Latent Deviation | Manifest Deviation |
|---|---|
| Esophoria = S or E | Esotropia = ST or ET |
| Exophoria = X | Exotropia = XT |
| Right hyperphoria = RH | Right hypertropia = RHT |
| Left hyperphoria = LH | Left hypertropia = LHT |
The amount of the deviation is expressed in pd. A prime (’) after the initial indicates the measurements were done at near fixation, i.e., ST 30 distance esotropia and ST’ 40 near esotropia.
For example,
SC | CC |
ST = 10 | ST = 5 |
ST′ = 20 | ST′ = 10 |
bifocal = 0 | |
[+3 or+3.50 | |
(state amount)] |
| Note: | SC (without optical correction) CC (with spectacles) bifocal |
Corneal Reflection Tests
These tests are used for infants and patients with marked amblyopia.
Hirschberg Method
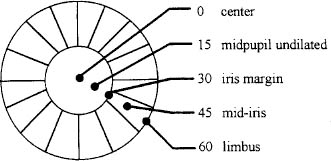
The patient fixates on a light while the examiner compares the relative location of the corneal reflection of each eye. Strabismus is usually present if the corneal reflections are not symmetric. The angle of strabismus can be grossly estimated by the amount of horizontal displacement of the corneal reflections. (This can be done vertically but is classically applied horizontally.) Each millimeter of displacement is roughly equivalent to 14 pd of deviation. For example, in general
Center = 0
Midpupil(halfway from center to iris margin) = 15
Iris margin = 30
Mid-iris = 45
Limbus = 60
Krimsky Method
In this method the corneal reflexes are centered by the use of prisms. The amount and type of deviation should be determined with the fixating eye remaining in primary position at near fixation. Therefore, it is suggested that the prisms be placed over the deviating eye until the corneal reflexes are centered. At distance fixation it is difficult to accurately evaluate the corneal reflections. In this case the prism is placed over the fixating eye until the usually deviating eye appears straight in the orbit.
Simultaneous Prism and Cover Test
Strabismus frequently exhibits a certain variability in amount of deviation for various reasons, i.e., physical or emotional state, the accommodative and proximal convergence, poorly developed reflexes, amblyopia, etc. The examiner should be aware of any variability in the angle of deviation under different testing as well as under nontesting conditions (casual observation of the patient) and the parents’ history of variations of the deviation. Therefore, every effort is made to determine the minimum as well as the maximum angle of deviation. Both these angles of deviation may have functional as well as cosmetic importance. The prolonged alternate cover and prism test is used to elicit the full amount of the deviation, whereas the simultaneous prism and cover test is used to measure the ordinary binocular condition deviation. While the patient fixates a target, the fixating eye is covered with an occluder at the same time that a prism is placed over the deviated eye. The prism is held base out if an esotropia is present and base in with an exotropia. Covering the fixating eye forces the deviating eye to fixate. If the appropriate prism is used, there is no movement of the newly fixating eye, as the prism has deflected the image onto the fovea. However, if there is movement, the prism is used inappropriately, and the test is repeated with a deterrent prism starting again from a binocular situation.
4Δ Base-Out Test
Another test that is useful in determining whether bifixation (central fusion) or monofixation (absence of central fusion) exists is the 4Δ base-out test. While the patient fixates on a letter at distance, a 4Δ prism base out is introduced before each eye separately. There are three basic responses to this test.
1. A convergence movement indicating a heterophoria with bifoveal fusion
2. No movement indicating a heterotropia, and the prism has been placed before the suppressed nonfixating eye
3. Parallel movement of the eyes toward the apex of the prism indicating a heterotropia, and the prism has been placed before the fixating eye
FIGURE 11-1. The accommodometer: side facing patient.
Near Point of Convergence
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


