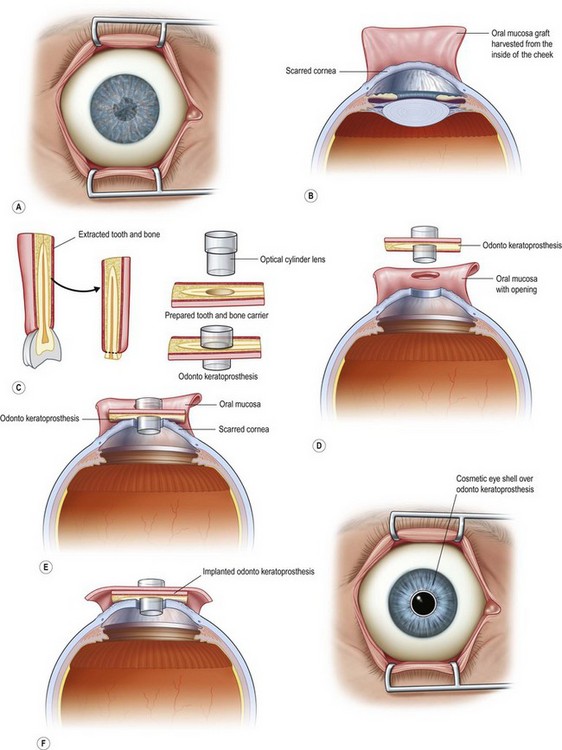
53 Corneal transplantation has revolutionized the treatment of corneal blindness. Corneal allografts into non-inflamed recipients with a healthy ocular surface (e.g. keratoconus) offers a survival rate of > 80% at 5 years under optimal conditions.1 This high anatomical allograft survival doesn’t apply to patients with corneal blindness that is associated with an inflamed ocular surface and/or vascularized cornea, such as autoimmune disease (ocular cicatricial pemphigoid, Stevens–Johnson syndrome) and limbal stem cell deficiency (aniridia, severe chemical burns). Corneal allografts in these situations have a poor prognosis, with graft survival rates of less than 25%.2 According to the World Health Organization, corneal blindness is the fourth most common cause of blindness in the industrialized world and the second most common cause of blindness in the developing world. The majority of these cases occur in the setting of end-stage ocular surface disease.3 There has been a need for a safer and effective alternative to corneal allografts. Guillaume Pellier de Quengsy initiated the idea of designing a keratoprosthesis as an alternative to corneal allograft.4 Currently, the three most common keratoprosthetic devices are the Boston Keratoprosthesis (KPro™), the AlphaCor™ artificial cornea and the osteo-odonto-keratoprosthesis (OOKP).5 The OOKP was developed more than 45 years ago. The basic concept of this keratoprosthesis is to use the patient’s own tissue (heterotopic autograft of patient’s own tooth root and alveolar bone) to support an optical cylinder of polymethyl methacrylate (PMMA), thereby significantly reducing the possibility of an immunogenic response against foreign tissue. Having autologous living material supporting the optical cylinder decreases the chance of prosthesis extrusion and offers long-term stability to the optical cylinder. The OOKP is conformed by the patient’s own tooth root and alveolar bone that are fashioned into a lamina that supports a PMMA optical cylinder. The device is covered by mucosa (preferably buccal mucosa) to offer a layer of protection from a hostile environment, such as a keratinized ocular surface (Fig. 53.1). Currently, the OOKP designed by Strampelli and modified by Falcinelli (MOOKP) is the keratoprosthesis with best visual outcomes and proven long-term follow-up to restore sight in patients with end-stage ocular surface disease.6 The MOOKP is indicated for patients with bilateral corneal blindness and associated end-stage ocular surface disease, severe vascularization of the cornea and/or end-stage limbal stem cell deficiency (Box 53.1). Relative and absolute contraindications for the OOKP surgery are listed in Table 53.1. Table 53.1 Surgical candidates for MOOKP need to have an extensive ophthalmic and medical evaluation. Evaluation includes the estimation of potential visual acuity, detailed slit lamp examination, ultrasound biomicroscopy, A-scan biometry and digital or mechanical estimation of intraocular pressure. The cornea surgeon should evaluate the eye in collaboration with a glaucoma surgeon to detect the possibility of preoperative glaucoma, and to determine a medical and/or surgical treatment strategy for either current or future glaucoma management. Approximately 50% of all patients who require a keratoprosthesis have a pre-existing diagnosis of secondary glaucoma and progressive optic nerve damage from glaucoma, which is the most common cause of vision loss in patients with MOOKP.7 Visual evoked potential (VEP) and electroretinography (ERG) can be used in the preoperative evaluation to obtain a more objective estimate of the potential visual acuity. The use of these tests is not absolutely necessary, but studies have shown that eyes demonstrating normal ERG or VEP achieved better visual outcomes than those with abnormal test results.8 A detailed evaluation of the patient’s oral mucosa and the overall oral cavity health needs to be performed prior to the MOOKP. Orthopantomography and X-ray of the tooth are mandatory, and the use of spiral computerized tomography (CT) is helpful. The healthiest tooth with the largest root is chosen for the harvesting step. According to Falcinelli et al.,6,9 the preferred choice for the tooth, in descending order of usefulness, is the upper canine, inferior canine, bother upper incisors, first or second upper premolar, first and second inferior premolar and inferior incisors. In cases of poor oral health, where it is not possible to harvest a healthy tooth, an allograft from a living relative is considered. This will mandate the use of systemic immunosuppression. Before making the decision to proceed with an allograft, the patient needs to understand the risk of immunosuppressive treatment and know that the long-term outcomes are not equal to the standard procedure. The Rome–Vienna Protocol was published under the leadership of Professor Falcinelli in 2005. This surgical protocol serves as the gold standard for OOKP surgery and provides a detailed description of the surgical technique.9 Our group strictly follows this protocol (Fig. 53.2). The MOOKP has two major surgical stages. Stage 1 involves the preparation of the globe, mucosa and the osteo-odonto lamina. Stage 2 involves the implantation of the osteo-odonto lamina. Both surgical stages require general anesthesia. It is an absolute requirement that the patient receives a pre-anesthetic evaluation. Patients with Stevens–Johnson syndrome (SJS) frequently suffer from oropharyngeal mucosal erosions, scarring, and strictures, all of which can cause a difficult intubation. Surgical stage 1 can be managed with nasotracheal or orotracheal intubation and stage 2 with orotracheal intubation.10
Modified Osteo-Odonto-Keratoprosthesis
MOOKP
Introduction
MOOKP Indications and Preoperative Considerations
Absolute Contraindications
Relative Contraindications
Pediatric patients, due to the high rate of bone reabsorption
Defective light perception, especially in the setting of known advanced glaucoma.
Phthisis bulbi
Patient unable or refusing to have close clinical follow-up
Eyes with no light perception
Eyes with inoperable retinal detachment or a severely damaged posterior segment.
Unrealistic visual and/or cosmetic expectations
Surgical Technique
Modified Osteo-Odonto-Keratoprosthesis: MOOKP