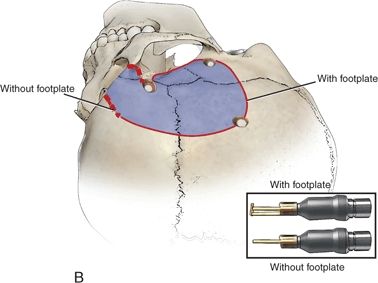
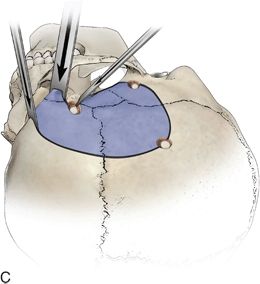
FIGURE 30.1 A. Planned ¾ coronal incision for a right modified orbitozygomatic craniotomy. B. Burr hole placement and cranial osteotomies for right modified orbitozygomatic craniotomy. C. An osteotome is used to weaken the attachment of the bone flap along the sphenoid wing and roof of the orbit.
Burr Holes
The McCarty burr hole is essential in performing the one-piece modified OZ craniotomy (Fig. 30.1B). The burr hole is placed over the frontosphenoidal suture 1 cm posterior to the frontozygomatic suture. This burr hole exposes the periorbita and dura of the frontal lobe. Two additional burr holes are made. One is placed in the posterior frontal region near the superior temporal line and the other is in the temporal squamosa area just above the root of the zygoma.
Creating the Bone Flap
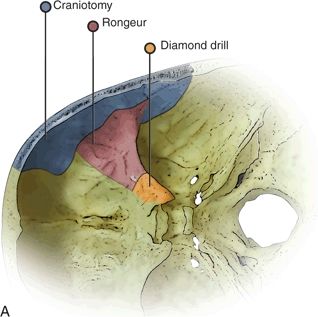
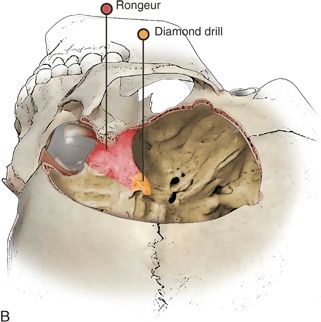
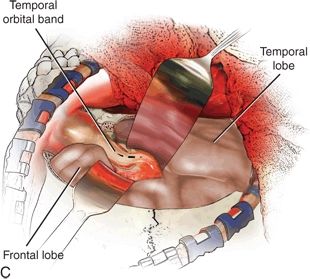
Using a high-speed drill with a footplate attachment, the first cut is made from the temporal burr hole to the posterior frontal burr hole in the extradural plane. The cut is then extended forward to the level of the supraorbital notch or foramen. The second cut is made from the McCarty burr hole down to the sphenoid wing. The third cut is then made from the temporal burr hole forward and up to the sphenoid wing. A side-cutting bit on the high-speed drill is then used to cut the bone of the zygoma near the frontozygomatic suture down to the McCarty burr hole. This side-cutting bit drill is also used to weaken the orbital rim at the supraorbital notch or foramen. Using an osteotome, the attachment of the sphenoid wing is loosened (Fig. 30.1C). The osteotome is then used along the orbital rim to propagate a fracture line in the anterior roof of the orbit. The modified OZ flap is then cracked forward and separated from the dura and periorbita in one piece. The bone flap should be harvested easily, and the “crack” should not be forced. Upon removal of the bone flap, the anterior contents of the orbit and the frontal and temporal dura are exposed. A small rongeur can then be used to remove additional bone from the roof of the orbit and the sphenoid wing (Fig. 30.2A and B). The surgeon should remove this bone leaving the periorbita intact. Upon removal of the roof and wing, the surgeon will encounter the superior orbital fissure. Bone lateral to the superior orbital fissure down to the foramen rotundum can be removed easily with a rongeur. By removing bone over the superior orbital fissure, the temporal–orbital band is fully exposed.