and Yi Ning J. Strube2
(1)
Wright Foundation for Pediatric Ophthalmology and Adult Strabismus Medical Center, Los Angeles, CA, USA
(2)
Queen’s University, Kingston, Ontario, Canada
Electronic supplementary material
The online version of this chapter (doi: 10.1007/978-1-4939-1480-7_22) contains supplementary material, which is available to authorized users.
Keywords
Minimally invasive strabismus surgeryCentral muscle-sclera plicationMini-plicationCentral tenotomyMini-tenotomyMinimally invasive strabismus surgery provides a valuable option for our strabismus patients with small deviations, and offers an additional or alternative treatment option to the use of prism glasses. The techniques described below can be performed in the office under topical anesthesia, are less invasive than standard strabismus muscle surgeries, and preserve the integrity of the muscle insertion, presumably sparing the anterior ciliary vessels.
22.1 Central Muscle-Sclera Plication
This procedure is similar to the Wright plication described in Chap. 14, but only the central rectus muscle fibers are advanced (Fig. 22.1). The mini-plication was developed by the author (KWW) as a minimally invasive way to treat small-angle strabismus [1]. A 5-mm mini-plication will correct approximately 8 PD of vertical or horizontal strabismus. Cooperative patients can easily have the procedure with topical anesthesia and mild sedation.
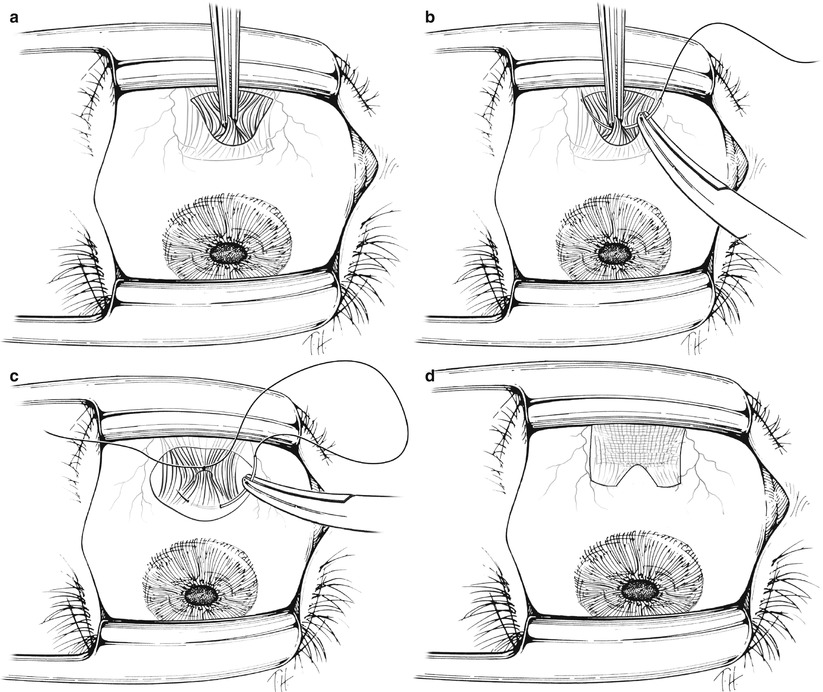
Fig. 22.1




Central muscle-sclera plication procedure for tightening the rectus muscle. (a) If topical anesthesia is used, two drops of tetracaine are instilled in the eye, followed by lidocaine gel. Phenylephrine 2.5 % and an antibiotic drop are administered prior to surgery. After a Swan incision is made over the muscle insertion, the conjunctiva is dissected off the muscle belly about 6 mm posterior to the muscle insertion, and the muscle is grasped centrally about 5 mm from the insertion. (b) The muscle is lifted off the sclera and a double-armed 6–0 polyglactin 910 suture is placed underneath the forceps. The suture is tied in a square knot. (c) The suture is placed anterior to the insertion into the sclera and then tied in place to plicate the central portion of the muscle. (d) The final appearance of the muscle after the procedure
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
