Midface Fractures
Brendan C. Stack Jr
Francis P. Ruggiero
ANATOMY
Buttresses
The structure of the midfacial skeleton is related to its mechanical adaptation to forces generated by mastication. Forces of up to 200 pounds per square inch are developed during chewing. Additionally facial contours result from paranasal sinus pneumatization. These sinuses are involved in voice resonance, act as shock absorbers, and account for an approximate lightening of the head of 1 kg if they have otherwise been solid bone. The concept of buttresses describes the relatively stronger areas of the midfacial skeleton that bear the bulk of the vertically oriented forces produced during mastication. These forces are absorbed and transmitted to the base of skull (Fig. 81.1) (1).
The vertical buttress system has seven components, including three paired pillars and one unpaired structure: (a) The nasomaxillary (NM) (aka medial, nasofrontal) buttresses extend from the anterior maxillary alveolus along the pyriform aperture and medial orbit, through the nasal and lacrimal bones to the frontal bone. (b) The zygomaticomaxillary (ZM) (aka lateral) buttresses extend from the lateral maxillary alveolus along the lateral maxilla to the malar eminence of the zygoma, then superiorly along the lateral orbital rim to the frontal bone. (c) The pterygomaxillary buttresses extend posteriorly from the maxilla to the pterygoid plates of the sphenoid bone. (d) A midline buttress, consisting of the vomer and perpendicular plate of the ethmoid bone, connects the palatine process of the maxilla to the frontal bone (2).
The mostly curved, vertical buttresses are reinforced by a number of horizontal buttresses. These include the frontal bar (superior orbital rims plus the frontal bone), the inferior orbital rims, and the maxillary alveolus, among others (3).
Maxilla
The maxilla consists of paired bones also called maxillae. Each has a hollow body that is the maxillary antrum. Projections from the maxillary body extend superiorly and medially to the frontal and nasal bones, and laterally to the zygoma. The inferior and medial palatine process of the maxilla forms the bulk of the primary hard palate. The alveolar process of the maxilla extends inferiorly and holds the roots of the upper teeth (4).
The bone of the maxilla is for the most part quite thin. The lateral wall of the maxillary antrum however includes a wedge of thicker, compact bone. It is in this area that the ZM buttress arises. It appears that the greatest occlusal load is borne by this buttress.
Zygoma
The zygoma is a relatively sturdy bone that is important structurally, as an integral component of the buttress system, and also forms the aesthetically vital malar prominence. It is related to the surrounding facial bones via articulations with four bones—the frontal, maxillary, temporal, and sphenoid bones.
The superficial projections of the zygoma define two critical external arcs of facial contour (Fig. 81.2). The vertical arc follows the course of the ZM buttress (concave), running from the zygomatic process of the frontal bone, over the zygoma itself to the lateral antral wall of the maxilla (convex). The horizontal convex arc runs from the maxilla in the area of the lacrimal fossa, across the zygoma, to the zygomatic process of the temporal bone. The point of intersection of the vertical and horizontal arcs defines the location of the malar prominence.
The deep projections of the zygoma are the sphenoid projection, which articulates along the lateral orbital wall with the orbital plate of the sphenoid bone, and the orbital floor projection, that articulates with the orbital surface
of the maxilla along the lateral aspect of the orbital floor. The zygoma therefore constitutes the majority of the lateral orbital rim and wall, and a portion of the inferior rim and the orbital floor.
of the maxilla along the lateral aspect of the orbital floor. The zygoma therefore constitutes the majority of the lateral orbital rim and wall, and a portion of the inferior rim and the orbital floor.
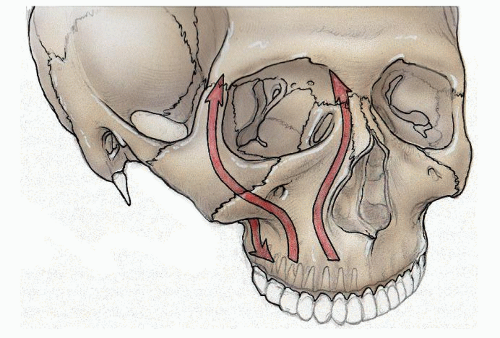 Figure 81.1 Vertical buttresses of the facial skeleton: The NM (medial), ZM (lateral), and pterygomaxillary buttresses of the facial skeleton are illustrated. |
PATHOPHYSIOLOGY/MECHANISM OF TRAUMA
With the midfacial skeleton adapted to the vertical forces of mastication, it is the force delivered at other vectors that cause the bulk of midface fractures. Common etiologies of midfacial fractures include motor vehicle accidents, assaults, and sporting events (5).
Maxilla
Le Fort Fractures
Rene Le Fort introduced a classification of midfacial fractures on the basis of cadaver experiments he performed in the early part of the 20th century (6). He noted that fractures tend to occur at characteristic locations, which correspond with relatively weak areas of the facial skeleton.
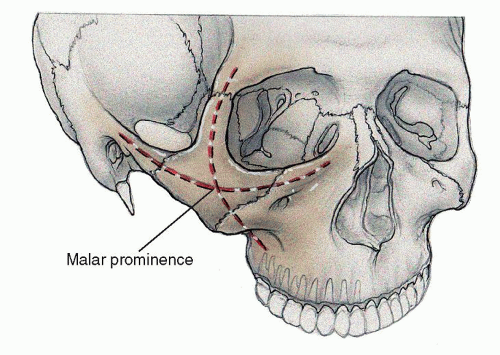 Figure 81.2 Vertical and horizontal projections of the zygoma. Their intersection defines the location of the malar prominence. |
Le Fort Level I fractures are transverse fractures separating the maxillary alveolus from the rest of the midfacial skeleton (Fig. 81.3).
These injuries generally result from anterior force directed at the lower midface. The NM and ZM buttresses are disrupted (7). The fracture line then extends transversely through the maxillary sinus and nasal septum and posteriorly across the pyramidal process of the palatine bone and pterygoid processes of the sphenoid bone (2).
Le Fort Level II fractures create a pyramidal NM fragment separate from the upper craniofacial skeleton. They result from either direct anterior force against the midface or inferior impact at the mandibular symphysis transmitted to the midface via the dentoalveolar segments of the mandible. Once again the NM and ZM buttresses are disrupted, this time more superiorly than the Le Forte I level. The fracture line extends from the nasal root via the lacrimal bone and medial orbital wall, then anteriorly along the orbital floor to the infraorbital canal. From this point, the fracture line follows the ZM suture to anterolateral maxillary wall. Posteriorly, the fracture line passes across the infratemporal surface of the maxilla through the lower pterygoid plates (7, 8).
Le Fort Level III fractures, which result in complete separation of facial skeleton from the skull base, are less common. They usually result from anterior force directed obliquely to the plane of the vertical buttresses (1). The vertical buttresses are disrupted at their superiormost extent. The fracture line extends through the root of the nose, across the lacrimal bone and medial orbital wall, across the orbital floor to the inferior orbital fissure. From this point, one fracture line traverses the lateral orbital wall as it approaches the frontozygomatic suture; a second line passes over the back of the maxilla to the lower pterygoid plates. An additional fracture line through the zygomatic arch completes the craniofacial dysjunction (8, 7).
In clinical practice, the patterns of maxillary fractures encountered are rarely as orderly as the above suggests. Le Fort’s original work demonstrates that he was certainly not unaware of this. The level I to III classification scheme is a distillation of some of his most significant experimental observations. In his experiments, and most definitely in real-life trauma, force is delivered unevenly to each side of the face, at varying angles, and at variable locations. The resulting fractures may be asymmetric from one side of the face to the other (i.e., Le Fort II on the left, Le Fort III on the right), may combine with other fractures to create a more complex pattern (e.g., a Le Fort II fracture and a zygomaticomaxillary complex (ZMC) fracture on the same side of the face constituting a “complex” Le Fort III fracture), or may be maxillary fractures not described by the classification at all.
Other Maxillary Fractures
Anterior forces localized between the nose and malar prominence may produce anterior maxillary wall fractures. Significant force delivered to the lower anterior midface, in addition to generating the classic fracture patterns described by Le Fort, may less commonly cause fractures
of the palate. While they may occur in isolation, palatal fractures tend to accompany extensive facial injuries (9). Most often, the palate is fractured in a sagittal fashion, in a paramedian plane (see Fig. 81.11). Fractures in a number of other orientations and locations are also possible (10). Clinical indicators of palatal fractures include palatal lacerations, lip lacerations that extend into the gingivolabial sulcus, maxillary tooth loss, and malocclusion.
of the palate. While they may occur in isolation, palatal fractures tend to accompany extensive facial injuries (9). Most often, the palate is fractured in a sagittal fashion, in a paramedian plane (see Fig. 81.11). Fractures in a number of other orientations and locations are also possible (10). Clinical indicators of palatal fractures include palatal lacerations, lip lacerations that extend into the gingivolabial sulcus, maxillary tooth loss, and malocclusion.
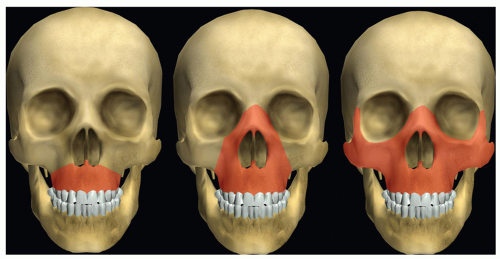 Figure 81.3 Anterior view of facial skeletons. Shaded areas correspond to Le Fort levels I, II, and III fractures. LifeART image copyright (c) (2012) Lippincott Williams & Wilkins. All rights reserved. |
Palatal fractures, and in particular those oriented sagittally, alter the width of the maxilla and permit the rotation of the maxillary dentoalveolar segments. One of the fundamentals in management of severe facial fractures is the intraoperative restoration of normal maxillomandibular occlusion, with anatomic reduction of fractures following from this basis. Palatal fractures, by complicating the restoration of occlusion, can confound this strategy if not appropriately addressed first (10, 11).
Zygoma
Zygomaticomaxillary Complex Fractures
Various terms are used to describe fractures involving the zygoma and its articulating bones. These include malar fractures (12), zygoma or zygomatic fractures (13), ZMC fractures (14), tripod fractures (15), tetrapod fractures, trimalar fractures, zygomatico-orbital fractures (16), and orbitozygomatic fractures (17). All of these terms emphasize certain salient features of this type of injury. For example, the term “tripod” underscores the observation that blunt force to the zygoma tends to disrupt not the zygoma itself, but rather, its three superficial articulations, to the frontal, maxillary, and temporal bones; the intact body of the zygoma has a tripod-like appearance (Fig. 81.4). The terms “zygomatico-orbital fracture” and “orbitozygomatic fracture” stress that because it forms portions of the lateral and inferior orbit, fractures that involve the zygoma are necessarily also orbital fractures. The most important point for the surgeon-in-training to understand is that all of the terms refer to the same injury. Henceforth within this chapter, the term ZMC fracture is used for uniformity.
ZMC fractures generally result from blunt trauma to the malar eminence, the most prominent feature of the lateral midface. They are the second most common facial fracture, after nasal fractures (18). Routinely, they involve disruption of the projections of the zygoma. The severity of ZMC fractures seems most related to the force and velocity of impact (14). In the most severe injuries, the sturdy zygoma itself may be fractured.
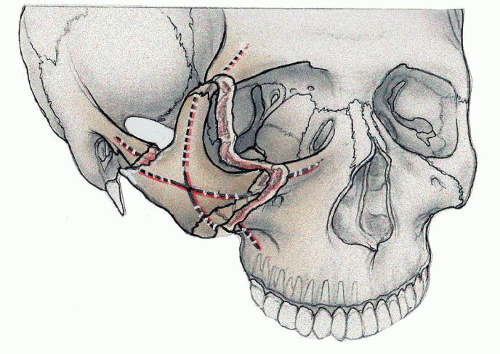 Figure 81.4 ZMC fracture—ZMC fracture, illustrating the tripodlike appearance of the displaced zygoma, as well as the orbital involvement in the injury. |
A distinctive clinical feature of ZMC fractures is orbital injuries that differ somewhat from those found in isolated orbital trauma. In a typical orbital floor blowout fracture, orbital volume expands; the extent of expansion predicts the likelihood of enophthalmos and diplopia, and the need for surgical repair. In ZMC fractures, the typical inward and medial displacement of the zygoma often results in a decrease in orbital volume (19). Therefore, acute enophthalmos is rarely seen at the time of presentation of a ZMC fracture. The need for floor exploration/repair in ZMC fractures must also take into account the effect that reduction will have on orbital volume.
Another common clinical feature of ZMC fractures is facial numbness and paresthesia. This is caused by damage to the infraorbital nerve (V2) at its exit from the midportion of the inferior orbital rim, which lies directly within one of the fracture lines. These symptoms are present in as many as 90% of ZMC fracture patients at presentation (20). The symptoms resolve spontaneously in many, but not all, patients after disimpaction of the fragments.
Zygomatic Arch Fractures
The zygomatic arch is most frequently disrupted as a component of a ZMC fracture (21). Less common, and distinct from this type of injury, is the isolated zygomatic arch fracture. Isolated arch fractures result from a direct lateral force to the arch, most frequently the result of a motor vehicle accident or fisticuffs (21).
Several fracture patterns may be seen in isolated arch injuries. The most common pattern is two mobile fragments of arch resulting from a total of three fractures. In this pattern, the fragments are displaced medially, in a v configuration (Fig. 81.5).
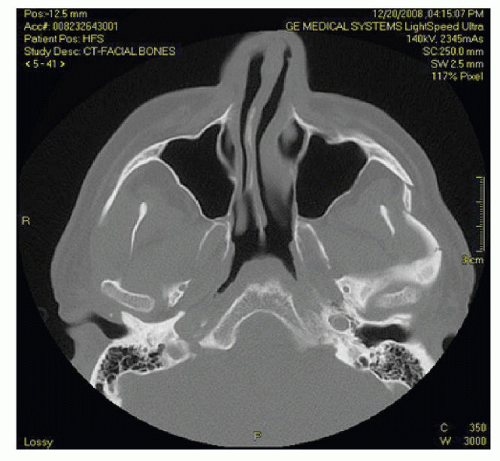 Figure 81.5 Axial bone-window CT demonstrates the most common pattern of isolated fractures of the zygomatic arch: a total of three fractures create two fragments, displaced medially in a V-like configuration. |
 Figure 81.6 Patient who suffered an isolated fracture of the left zygomatic arch after direct blow from a batted softball. Depression of the lateral midface is quite visible in this case. |
Patients with isolated arch injuries, particularly those with the characteristic v pattern, will have a palpable, and frequently visible, deformity of the lateral midface (Fig. 81.6). This finding is often accompanied by a degree of trismus, resulting from the impingement of the fracture segments on the underlying coronoid process of the mandible or the temporalis muscle.
PATIENT EVALUATION
Evaluation of the patient is the critical first step to assure complete and accurate fracture repair and optimal aesthetic results. There may be a temptation to truncate the physical exam, in deference to the almost universal use of admission pan computerized tomography (CT) for trauma patients. Although high-resolution CT has been a great advance in the diagnosis, treatment, and postoperative critical evaluation of facial trauma, imaging is not a substitute to the laying on of hands in a focused head and neck trauma evaluation. Poor aesthetic results should not be accepted in facial fracture repair, as the primary motivation for their repair in many cases is cosmesis.
Physical Exam
Regardless of the existence of scans, or the putative diagnosis offered by the consulting physician, each new facial trauma patient should be evaluated in a systematic fashion, beginning with the history and physical exam.
All facial trauma patients are trauma patients, and are best served by the standardized Advanced Trauma Life Support (ATLS) approach taught by the American College of Surgeons. This evaluation process ensures the orderly evaluation and prioritization of treatment of the most lethal injuries first. All residents and those practicing surgeons who manage facial trauma must be familiar with the trauma
evaluation process, and should consider certification in ATLS. We shall highlight portions of the trauma evaluation process that are particularly germane to the care of the maxillofacial trauma patient.
evaluation process, and should consider certification in ATLS. We shall highlight portions of the trauma evaluation process that are particularly germane to the care of the maxillofacial trauma patient.
Airway issues can potentially be seen with any head and neck trauma sufficient to result in midface fractures. While isolated midfacial trauma is unlikely to compromise the airway, accompanying mandible fractures are particularly significant in this regard. A loss of continuity of the mandible arch results in retrusion of the tongue and larynx, which may create an obstructed upper airway. When evaluating such a patient, consideration should be given both to immediate need for airway management and its implications for fracture repair. If elective intubation (as opposed to an emergent airway) is possible, alternatives to oral intubation should be entertained if maxillomandibular fixation (MMF) will be required for fracture repair.
Concomitant C-spine injuries are also common in patients with facial fractures, with an incidence approaching 10% (22). All facial trauma patients should thus be managed with C-spine precautions as proscribed by ATLS, even though this can significantly complicate the evaluation and management of the facial injuries.
Neurologic deficits should be sought and well documented if they exist. Of particular pertinence in the facial trauma patient are cranial neuropathies. A regimented exam of cranial nerves II-XII should be performed. Findings of significance that may impact the timing and approach to repair include neuropathies affecting the eye (cranial nerves II, III, IV, and VI), the trigeminal nerve, and the facial nerve.
Eye-related cranial neuropathies might make surgery an emergency, especially if associated with an open globe. Conversely, the presence of a compromised optic nerve (optic neuropathy) may delay facial fracture management. More details of the ophthalmologic evaluation of facial trauma patients are presented below.
Trigeminal nerve injury is not an emergency per se but must be documented preoperatively. If not, the assumption is made that it was a surgical complication and this has been a point of litigation specifically related to facial fracture repair. Facial nerve dysfunction is usually related to a temporal bone fracture or extensive facial soft tissue injury. It is important to know if the nerve was functioning upon presentation or not. This will help with the decision to explore and perhaps repair the nerve immediately or to treat expectantly.
The Facial Assessment
There are key elements of the exam that must be appreciated and documented preoperatively. These elements will help the surgeon appreciate the full extent of the facial trauma as well as avoid problems with litigation that is a potential element in trauma cases.
The appearance of the face is examined. Is it wide or long? Is it asymmetrical? It is helpful but often difficult to obtain current pretrauma photos to assist with this assessment. Appreciation of any lacerations is important for planning surgical access as well as to focus exam for cranial nerve deficits. A full facial movement and sensory examination is also advised regardless of hard or soft tissue injury.
Overlying edema and patient discomfort may limit the utility of palpation. Still, palpation of the facial skeleton is mandatory, and can provide a more thorough understanding of the location of fractures and the extent of their displacement and mobility. A bimanual exam of the face should be performed. Placing gloved fingers in the mouth while stabilizing the head and face at various levels is used to examine for dentoalveolar and palatal stability, as well for the Le Fort fractures. Both visual and subjective (patient’s report) occlusal changes are vital to obtaining a successful reduction of facial fractures. Finally, are there exposed fracture elements and what is the status of the soft tissue? Will there be adequate soft tissue for reduction and closure of the fracture?
The Ophthalmologic Evaluation
The ophthalmologic exam of facial trauma patients deserves special emphasis and should never be deleted. Ocular injury is common in the facial trauma patient, at the time of initial injury, during the course of surgical repair, and even postoperatively. These injuries may be particularly devastating for patient and surgeon alike.
Early and complete ophthalmologic evaluation of every patient who has sustained a ZMC fracture (or any fracture involving the orbit) is an ideal yet often unrealized goal. The incidence of major (potentially blinding) ocular injury in ZMC fractures that require repair has been reported as 10% (23). Reconstructive surgeons must be sensitive to the possibility of direct ocular trauma and obtain consultation as indicated. A minimal preoperative examination includes testing of visual acuity (subjective and objective in both eyes), pupillary function, and ocular motility; inspection of the anterior chamber for hyphema; and visualization of the fundus for gross disruption. The presence of an afferent pupillary defect should be specifically sought, as this is a sensitive indicator of the presence of optic neuropathy. A decrease in visual acuity, alteration in color perception, or any abnormality observed on the other portions of this screening examination warrants detailed examination by an ophthalmologist before reconstruction of the bony injuries is undertaken.
COMPUTED TOMOGRAPHY
Evaluation of a patient with midface trauma has been greatly improved by the use of high-resolution CT. One millimeter slice thickness has become standard in many institutions, allowing for excellent coronal and sagittal
reconstructions. This modality is the “work horse” for evaluation of midface trauma. Axial and coronal scans identify fracture lines throughout the entire facial skeleton (Table 81.1). The expense of CT evaluation of patients with facial fractures other than simple nasal and mandibular fractures appears justified and can be done in virtually all emergency rooms (24).
reconstructions. This modality is the “work horse” for evaluation of midface trauma. Axial and coronal scans identify fracture lines throughout the entire facial skeleton (Table 81.1). The expense of CT evaluation of patients with facial fractures other than simple nasal and mandibular fractures appears justified and can be done in virtually all emergency rooms (24).
TABLE 81.1  DIAGNOSIS/EVALUATION DIAGNOSIS/EVALUATION | ||||||||
|---|---|---|---|---|---|---|---|---|
|
Using the CT images, the buttress system, particularly the vertical struts, must be systematically inspected preoperatively to document the degree of malalignment because of fracture fragment displacement. Fracture lines themselves through the buttresses do not mandate open reduction, but comminution, gross malalignment, and instability on physical exam all strongly suggest the need for reduction of the fractures in order to restore facial length and projection. Computed tomographic scans can show fractures of the condylar head, condylar neck, and vertical ramus of the mandible. The status of these structures must be known before fracture dislocations of the maxilla are placed into occlusion with the mandible.
The arcs of contour of the zygoma (see Fig. 81.2) are evaluated for decisions about the need for surgery and the appropriate operative approach. The CT finding of comminution and dislocation of both ends of the horizontal arc of contour indicates that exact reconstruction of the orbitozygomatic complex will be a challenge, and consideration should be given to additional access incisions, including an open approach to the zygomatic arch via a coronal incision.
FRACTURE MANAGEMENT: PRINCIPLES
Immediate Reconstruction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


