Microvascular Reconstruction: Introduction
The basic goal of head and neck reconstruction is to replace soft tissue and bony defects with similar tissue, restoring function, and optimizing cosmesis. Reconstructive surgical options are typically thought of in a hierarchy called the reconstructive ladder. (Table 78–1) Each step on the ladder increases the invasiveness and complexity of the reconstruction. Selection of the appropriate procedure depends on the defect and the goals of reconstruction.
Microvascular free-tissue transfer is a reconstructive technique in which tissue units are separated from their native blood supply and moved from one part of the body to a new location. The donor tissue has an identifiable artery and vein that are reanastomosed to recipient vessels, thus reestablishing blood flow. The potential for sensory reinnervation also exists through the reanastomosis of cutaneous nerves.
Refinements in free-tissue transfer over the last two decades have revolutionized the reconstruction of head and neck defects resulting from trauma, congenital anomalies, and ablative procedures for neoplastic processes. Free-tissue units are custom-designed for defects to provide characteristics similar to those of the original tissue. This versatility allows free flaps to serve multiple purposes, such as lining oropharyngeal defects and providing soft tissue support for maxillary defects. Free flaps offer other advantages because they do not have the anatomic constraints of regional pedicled flaps; they can be completed in a single stage, allow a simultaneous two-team approach, and have allowed ablative surgeons to expand their resection boundaries.
Preoperative Considerations & Planning
Important considerations in patient selection for free-flap reconstruction include age, comorbidities, and functional needs. Older patients are more likely to have comorbid factors that may increase their risk of exposure to prolonged anesthesia, affect wound healing, and decrease their tolerance for donor site morbidity. Some patients may not need the additional functional advantages gained from free-flap reconstruction. The risks and benefits of free-flap reconstruction must be considered for each individual patient.
Preoperative planning and communication with the anesthesia, nursing, and other involved surgical teams facilitate an efficient and well-executed surgical procedure. The tissue defect, functional needs of the patient, or both must be anticipated so that the optimal free flap is selected. Factors to be considered are donor tissue characteristics and composition, the length of pedicle, color match, soft tissue bulkiness, and the functional disability of the donor site. Communication about the patient’s intraoperative position and the preservation of adequate recipient vessels in the head and neck for anastomosis should also be relayed with the appropriate teams.
Although careful preoperative planning, patient selection, and flap design are important factors in free-tissue transfers, a meticulous microvascular technique is essential for the successful insetting and revascularization of tissue units. Critical to the execution of microvascular techniques are proper instruments, an operating microscope, and the expertise of microvascular surgeons who are trained in the techniques of vessel selection, handling, and preparation.
As a rule, vessel handling should be minimal to decrease the risk of trauma or injury. Vessels should be handled by the adventitia because direct contact with the intima may cause spasm, endothelial damage, and thrombosis, all with the potential of compromising blood flow to and from the transferred tissue. Vessels in the donor vascular pedicle are skeletonized, freeing the arteries from the veins within the vascular pedicle. Atraumatic vascular clamps are then placed. The ends of the vessels are transected and irrigated intermittently with dilute heparinized saline solution to prevent thrombosis. Finally, the excess adventitia is removed from the vessels to expose the media; adventitia trapped in the lumen at the suture line may initiate clot formation.
After both donor and recipient vessels are prepared, arterial anastomosis is followed by venous anastomosis. End-to-end anastomosis is the most commonly used technique, using appropriately sized monofilament sutures (8–0, 9–0, or 10–0). The end-to-side technique is used when there is a significant size mismatch between vessels (>3:1) or when the internal jugular vein is the recipient vessel. Significant tension should not exist at the suture line and vessels should be sutured to lie without twists or kinks.
Classification of Flaps
Free-tissue flaps are generally categorized by the types of tissues that are included in the transfer. Flaps most commonly contain skin (cutaneo-), muscle (myo-), bone (osseo-), or fascia (fascio-). For example, a flap that primarily contained bone and skin would be described as a osseocutaneous flap. Enteric flaps contain visceral structures and fall into their own category.
The cutaneous portion of each free-tissue flap is ultimately supplied by the main pedicle through perforating vessels. These small caliber perforators branch off the pedicle in somewhat predictable locations, although anatomic variation can exist. The perforating vessels travel from the pedicle to the skin to ramify in the subcutaneous plexus that then provides the vascular supply to the skin. Each perforator supplies a limited area of skin, therefore including an adequate number of these vessels in the flap design is essential for survival of the cutaneous paddle. Failure to do so can result in total or partial necrosis of the cutaneous portion of the flap. The course of these perforators from the main pedicle to skin must be preserved during flap elevation. They can travel through the fascial septum between muscles (septocutaneous perforators) or through the muscles themselves (musculocutaneous perforators). Similar vessels branch off the main pedicle to supply the periosteum of the osseous flaps.
Fascial & Fasciocutaneous Free-Tissue Flaps
Fascial and fasciocutaneous free-tissue flaps are commonly used flaps in head and neck reconstruction. They are characterized by thin, pliable fascia or skin without the bulk of pedicled myocutaneous flaps. Furthermore, they have the potential for crude sensation through the reanastomosis of an accompanying cutaneous nerve to nerves at the recipient site. They are primarily used for complex intraoral, pharyngeal, and cutaneous defects of the head and neck.
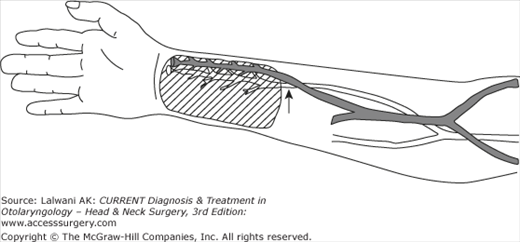
The free-tissue flap of the radial forearm is based on the radial artery, its associated venae comitantes, and the cephalic vein. The skin is supplied by fasciocutaneous vessels in the intermuscular septum between the brachioradialis and flexor carpi radialis.
The main advantages of the radial forearm flap are its thin and pliable tissue characteristics. This flap is an excellent choice to reconstruct oral cavity and oropharyngeal defects without limiting mobility of the tongue or remaining structures. Furthermore, this tissue can be tubed for pharyngeal, laryngeal, and esophageal defects. Crude sensation may be achieved through the reanastomosis of the lateral and medial antebrachial cutaneous nerves to nerves at the recipient site.
Possible ischemic injury to the hand is the main disadvantage to this flap. Preoperatively, the Allen test is performed to verify collateral flow to the hand from the ulnar artery via the palmar arch. Other potential drawbacks include tendon exposure, dysesthesia, motor dysfunction of the hand, and cosmetic results at the donor site from coverage with a split-thickness skin graft (Figure 78–1).
The fasciocutaneous flap of the lateral arm is supplied by the posterior branches of the radial collateral vessels from the profunda brachii artery. This flap has both a superficial and a deep venous system, the cephalic vein and paired venae comitantes, respectively. The perforators travel to the skin via the lateral intermuscular septum.
The advantages of this flap include a pliable skin paddle, the potential for sensory innervation through the posterior cutaneous nerve, and a donor site that can be closed primarily with minimal functional impairment. The disadvantages of this flap include smaller-caliber vessels and the variability of subcutaneous fat, which depends on the patient’s body habitus.
The fasciocutaneous flap of the posterior lateral thigh receives its blood supply from the cutaneous perforators of the profunda femoris artery, with the dominating third perforator. Venous drainage occurs through paired venae comitantes that accompany branches from the third perforator. The lateral femoral cutaneous nerve may also provide some sensation to the skin paddle.
The advantage of this flap is the availability of a sizable amount of pliable skin. The long axis of the skin paddle is designed over the intermuscular septum between the long head of the biceps femoris and the vastus lateralis muscles. This flap has been used after laryngopharyngectomy, and the ample subcutaneous tissue is useful in total glossectomy and skull base defects. Donor site morbidity is minimal but may include wound dehiscence and compartment syndrome. Another disadvantage is the potential anatomic variation of the vascular bundle.
The anterior lateral thigh flap was initially described at the time of the lateral thigh flap, but it did not gain widespread acceptance and popularity until recently. This flap is similar to the lateral thigh flap in tissue characteristics, yet in a more favorable position for simultaneous harvest, since the approach is to the anterior thigh. The anterior lateral thigh flap is based on a septocutaneous or septomyocutaneous perforator off the circumflex femoral artery and vein. The vascular pedicle travels between the rectus femoris and vastus lateralis muscles until giving off perforating branches that supply the cutaneous segment. This perforator is situated within a 3 cm circle located midway between the anterior iliac crest and the lateral patella.
Advantages of the flap include the minimal donor site morbidity, since primary closure is usually achievable and minimal muscular loss is required. Disadvantages include the somewhat short vascular pedicle, requirement for delicate perforator dissection, and the somewhat small vessel diameter. The clinical uses of this flap are similar to those of the lateral thigh free flap.
The scapular fasciocutaneous flap is based on the circumflex scapular artery and vein and may be harvested either as a fasciocutaneous or an osseocutaneous flap (see the next section “Osseomyocutaneous Free-Tissue Flaps”). The circumflex scapular artery originates from the subscapular artery and terminates into the transverse and descending branches, which may be used to supply two separate skin islands—the scapular and parascapular flaps, respectively. Two skin flaps supplied by a single vascular pedicle offer an excellent choice when both intraoral and external coverage are needed. The scapular region provides a large amount of tissue (14–21 cm) useful for larger defects, large-caliber vessels, and an acceptable color match to facial skin.
The major drawback of this flap is the lateral decubitus position of the patient during flap harvest, which limits a simultaneous two-team approach. Furthermore, no potential for sensory reinnervation exists. Although the donor site can be closed primarily with minimal morbidity, patients may require an arm sling and need physical therapy for a short period of time postoperatively.
The temporoparietal fascial flap derives its blood supply from the superficial temporal artery and vein. The temporoparietal fascia is thin, pliable, and well vascularized, allowing it to mold into complex facial defects and drape over skeletal frameworks such as the ear. This flap also has the unique property of providing a viscous gliding surface that is excellent for tendon excursion. The temporoparietal fascial flap is most often used as a pedicled flap for reconstruction of lateral temporal bone, orbital, limited oropharyngeal, and intracranial defects. As a free flap, it can be used for orbital reconstruction and a nasal lining in the setting of total nasal reconstruction; it has recently been described for laryngeal reconstruction after partial laryngectomy.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


