Microbiologic Diagnosis of Ocular Infections
Kirk R. Wilhelmus
Establishing the etiology of ocular infections requires collecting appropriate specimens and performing definitive laboratory studies.1,2 Some physicians process and examine clinical specimens in their offices,3 but most ophthalmologists use a microbiology laboratory. The microbiologist efficiently handles small samples and differentiates microorganisms commonly associated with healthy and infected eyes.
SPECIMEN COLLECTION
Material is collected for smears, cultures, and other diagnostic tests when available. Scrapings and swabbings are used to obtain material from the ocular surface. Intraocular fluids are obtained by syringe aspiration or vitrectomy instrumentation.4 Material is put into a transport container or inoculated directly onto enriched microbiologic media. A tissue biopsy is aseptically placed in a transport medium or preservative-free saline for homogenization.5,6 Foreign bodies, ophthalmic solutions, contact lenses, and other biomaterials can also be sent for microbiologic analysis.
Clinical samples are labeled with the patient’s name, type of tissue or fluid, and the date of collection. Universal precautions are followed during collection and processing. Specimens that are shipped elsewhere are put inside double mailing containers with a biohazard label and sent according to current postal regulations.
Submitting specimens and a requisition form to the microbiology laboratory starts a sequence of procedures designed to identify infecting microorganisms (Fig. 1). In the laboratory, smears are stained and examined, other rapid diagnostic tests are performed if possible, and inoculated culture media or cell lines are incubated under specific temperature and environmental conditions to enhance growth.
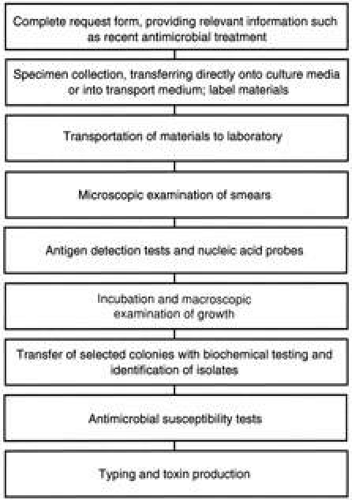 FIG. 1. Steps in the laboratory evaluation of ocular infection. |
The laboratory is staffed by accredited personnel who maintain a quality-assurance program with a procedure manual that includes periodic monitoring of equipment and supplies. Communication networks are maintained between office and laboratory personnel to facilitate timely distribution of laboratory test results. Suspected false-negative tests may indicate a need to contact the clinician for additional specimens.7 Results are also reported, when indicated, to the appropriate public health agency.
MICROSCOPY
Microscopic examination of ocular specimens is a common diagnostic test for confirming ocular infections. The instrument that collects the material must be clean and sterile to avoid particles that could cause staining artifacts.
Smearing the specimen in a thin film on a clean glass slide evenly distributes microorganisms. Thick smears cause some stains to clump, whereas excessive spreading fragments cells. Etched circles on the slide or rings made with a wax pencil help the microscopist to find the inoculation site. The examiner must be familiar with the various instruments and methods of microscopy.8
WET MOUNT
Scrapings and swabbings of the ocular surface and samples of intraocular fluids can be examined directly by brightfield illumination. Background light is reduced by reducing the microscope’s iris diaphragm. Microscopy of fresh, unstained specimens can delineate cells, but differentiation is difficult.
A saline mount is infrequently used in ocular microbiology but can demonstrate large parasites such as mites (Demodex) and lice (Phthirus pubis) from the eyelashes. Onchocercal microfilariae can be directly observed wriggling out of a scraping or biopsy submerged in saline or Hawk’s solution.9,10
Phase-contrast microscopy and Nomarski optics demonstrate the motility of viable organisms (e.g., Acanthamoeba trophozoites).11 Darkfield microscopy increases the visibility of translucent microbes such as spirochetes12 and spores.
Potassium hydroxide (KOH) 10% is sometimes mixed with the specimen to digest keratinized epithelial cells or thick mucin strands that might be confused with fungal elements. The KOH wet mount can be useful for detecting fungi from ocular specimens.13,14
Opaque suspensions of India ink or nigrosin help to outline formed elements such as fungi.15 Lactophenol cotton blue can be used in a wet mount of a clinical specimen to reveal fungi16 and amebic cysts.17 This stain is also used to examine yeasts and the spores of filamentous fungi grown on cultures.
FIXATION AND STAINING
A specimen is fixed to a glass slide so staining solutions do not wash it off. Heat fixation by passing the slide through a hot flame is satisfactory, but cytologic details are better preserved by alcohol fixation. The slide is flooded or immersed in a Coplin jar of methanol for 3 to 5 minutes. Methanol is also useful to prepare specimens for immunofluorescent processing.
Staining makes many microorganisms easier to see and helps to classify microbes and human cells.18 Examination of stained smears begins with scanning the slide under low power. The microscopist looks for inflammatory cells, epithelial cells, other tissue cells, and mucus with an eye to recognize the cytopathologic pattern.18 Without seeing at least 10 cells in a low-power field, the laboratory will probably question whether sufficient material was obtained. Stained smears are efficient in the evaluation of bacterial and fungal infections19 and are often the easiest way to confirm parasitic disease.20
Several staining methods are available to evaluate ocular specimens (Table 1). Basic dyes (e.g., hematoxylin) stain acidic structures such as nuclear chromatin. Acidic dyes (e.g., eosin) stain basic substances in the cytoplasm. Stains capable of fluorescence glow under ultraviolet light and make it easier to find microorganisms scattered on a smear. Extra, unstained smears are frozen to prevent breakdown of microbial and viral components. Several stains have high predictive value (Table 2) for confirming chlamydial conjunctivitis,21,22,23,24 bacterial keratitis,25,26,27 fungal keratitis,14,26,27,28,29,30 or endophthalmitis.31
TABLE 1. Microscopic Procedures Used in Ocular Microbiology | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
TABLE 2. Performance of Microscopic Examination Compared to Culture for Ocular Infections | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
LIGHT MICROSCOPY
Gram’s Stain
Gram’s staining is a standard method in bacteriology laboratories. Crystal violet is applied, then bound to bacterial cells by a weak iodine solution. An acetone-alcohol solvent removes the dye from bacteria whose cell walls lack teichoic acid cross-links that resist decolorization. Dye-retaining, gram-positive bacteria remain dark blue, while gram-negative bacteria are counterstained pink-red with safranin. Color and shape help in presumptive classification. Modifications such as the Brown-Hopps stain are applicable to tissue sections. A fluorescent modification is not as sensitive as the conventional Gram’s stain.32
In microbial keratitis, Gram’s staining successfully identifies the responsible organism in many culture-positive cases.33 During endophthalmitis, the Gram’s stain is also useful, although less sensitive, in evaluating vitreous aspirates.34 Gram’s staining has some utility for diagnosing bacterial conjunctivitis35,36,37 but has high predictive value for gonococcal and meningococcal conjunctivitis. Caution is needed to avoid overinterpreting the Gram’s-stained smear. Presumptive identification must be verified by culture isolation.
Giemsa Stain
Methylene blue stains nucleic acids in microorganisms, leukocytes, and tissue cells blue against a light gray background. Giemsa’s methylene blue derivative enhances visualization. Modified Giemsa staining highlights DNA in human cell nuclei and cytoplasmic RNA in lymphocytes. Bacteria, intracellular chlamydial elementary bodies, and many viral inclusions stain dark blue. Fungi and parasites are visualized by precipitation of the stain upon their outer walls.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


